
Abstract
Abstract
Background:
The intramedullary insertion of antibiotic-impregnated cement beads is used widely for the treatment of intramedullary infection. This report describes an improved technique for removing chains of antibiotic beads inserted into the intramedullary cavity.
Methods:
We examined four cases in three patients of the intramedullary insertion of chains of antibiotic-impregnated cement beads for the treatment of osteomyelitis of the diaphysis of the tibia after the fixation of fractures with interlocking nails. During bead removal, the tip of an intramedullary guidewire was bent into a hook shape and was then engaged with the chain of impacted beads. The guidewire was removed from the intramedullary cavity, permitting the extraction of any beads adhering to the wire.
Results:
As beads came into contact with the tip of the intramedullary guidewire, they could be extracted easily. No additional incision or bone fenestration was required.
Conclusions:
The use of a hook-shaped intramedullary guidewire simplifies the removal of chains of antibiotic-impregnated cement beads without the need for an invasive procedure. This technique makes the use of chains of cement beads a favorable choice for treating intramedullary infection.
I
Patients and Methods
Between June 2010 and February 2013, we treated three patients with a total of four episodes of intramedullary infection of the tibia who had been treated through the insertion of chains of antibiotic-impregnated cement beads (Table 1). All of the patients had a history of insertion of an interlocking nail in the tibia for fixation of an open fracture of the tibial diaphysis. On the basis of the fracture classification system of the Orthopedic Trauma Association, one of the patients had a type 42-A2 fracture and two of the patients had fractures of type 42-A3. All three patients' fractures were classified as type 3B open fractures according to the Gustilo–Anderson fracture classification system. At the time of insertion of the antibiotic bead chains used to treat the patients' infections, the fracture sites in two of the patients were in a state of non-union, whereas the tibial fracture in the third patient showed complete union.
MRSA=Methicillin-resistant Staphylococcus aureus; OTA=Orthopedic Trauma Association.
According to Gustilo–Anderson fracture classification.
At a mean of 81.3 d (range 50–113 d) after their implantation, the antibiotic bead chains were removed from the patients' tibiae. For these procedures, patients were placed on a radiolucent surgical table and positioned to allow easy radiographic visualization of the tibial treatment site with an image intensifier. A longitudinal incision was made on the area of patellar tendon, at the site of the previous scar remaining from the operative treatment of each patient's tibial fracture. After dissection of soft tissue and exposure of the proximal end of the antibiotic bead chain, gentle traction was applied to the chain to remove beads in the proximal part of the intramedullary cavity. When this could not be accomplished with traction on the wire, a hook-shaped intramedullary guidewire was inserted into the cavity (Fig. 1D).

Patient 1.
A 2.4×430-mm drill-tipped passing pin for reconstruction of the anterior cruciate ligament (ACL) (Arthrocare, Sunnyvale, CA) was used to extract the antibiotic beads. The distal end of this guidewire was bent to almost 330°, giving it a hook shape (Figs. 1E and 2). The space between the tip of the hook and the guidewire was narrower than that of the intramedullary cavity, and the wire was sufficiently long to reach from the proximal end of the tibia to the distal end of the intramedullary cavity. The hook of the guidewire was positioned just below the bottom of the bead to be extracted, after which the guidewire was removed from the intramedullary cavity, thereby removing a bead caught on the hook at a time (Figs. 1D and 3). Repeated extractions lead to complete removal of the beads in the intramedullary cavity (Fig. 1E, F). Additional reaming and re-insertion of the implant used for fixation of the patient's fracture was optional and dependent upon the patient's bone-union status.

(Left) A drill-tip passing pin used as a guide for reconstruction of the anterior cruciate ligament. (Right) The tip of the wire pin has been bent to create a hook for the retrieval of antibiotic-impregnated cement beads from the medullary cavity of a long bone. The size of the hook is approximately 10 mm.
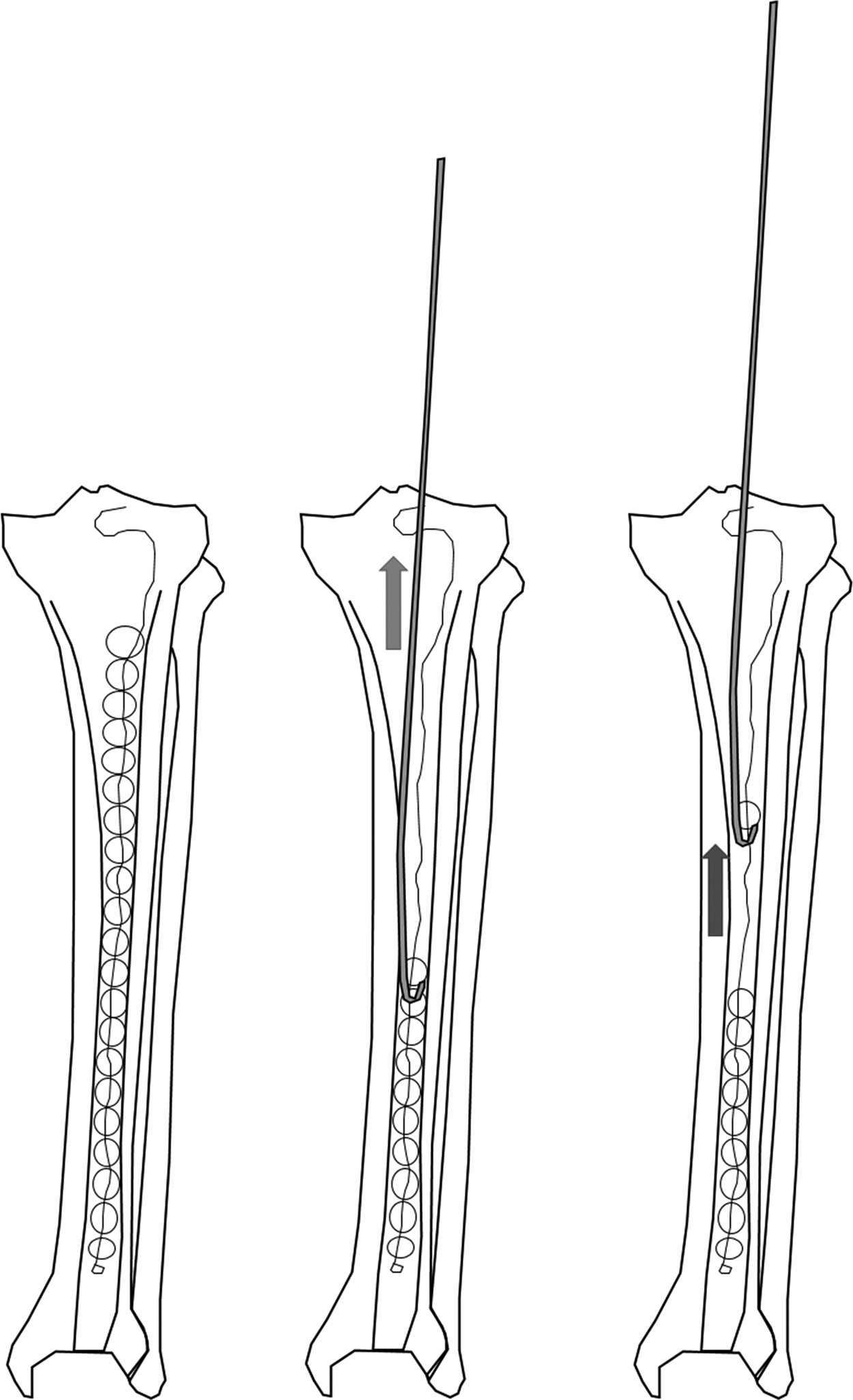
(Left) Cement-bead shain shown in intramedullary cavity of the tibia. (Center) A hook-shaped intramedullary guidewire is passed into the cavity and used to engage a bead in the cement-bead chain. The bent, hook-shaped tip of the wire is shown as positioned just below the bottom of the bead. (Right) The wire is shown being used to extract the engaged bead from the intramedullary cavity.
The guidewire technique permitted all of the beads in the intramedullary cavity of the tibia to be removed without bone fenestration or any other invasive procedure. The average time of the fluoroscopic guidance for the complete removal of the beads was 29.3 s (range 23–36 s). In one case, the chain of cement beads was removed and a new interlocking nail inserted at the time of their removal because of persistent non-union. Re-insertion of the cement-bead chain was necessary at 3 mo after the insertion of this nail because of a recurrence of intramedullary infection. After the passage of a further 3 mo the cement-bead chain was successfully removed with the hooked guidewire technique. Union of the patient's persistent fracture was achieved with the application of an Ilizarov ring fixator.
Discussion
The management of osteomyelitis relies primarily on the local delivery of antibiotics [2,6], and in contrast other manifestations of osteomyelitis, intramedullary infection in the disease usually presents no sequestrum or dead bone, making removal of the nail used for fixation of a fracture of the bone, together with reaming and lavage of the intramedullary cavity, the mainstay of treatment of such infection [1,7,8]. In this setting the insertion into the intramedullary cavity of antibiotic-impregnated cement beads to sterilize the canal is the preferred method of local delivery of antibiotics to the site of infection [3,7,9]. However, the removal of such beads from the cavity may be compromised by the ingrowth of granulation tissue between the beads [4,5]. As an alternative to the use of cement beads, some reports have suggested the use of an antibiotic-impregnated cement rod, but this has, in some cases, been accompanied by breakage of the rod, and in other cases the diameter of rod has also been too large for insertion into the intramedullary cavity. In such cases the broken rod has had to be extracted by bone fenestration [4,5].
In the cases of our patients, the hook-shaped intramedullary guidewire used for retrieving cement beads from the intramedullary cavity was passed easily into the narrow space between the wall of the cavity and the beads, despite the ingrowth of granulation tissue into the cavity. Furthermore, this guidewire had sufficient flexibility to be inserted into the intramedullary cavity and sufficient strength for use in extracting remnant beads from the cavity. This technique may therefore add value to the cement-bead-chain method for treating osteomyelitis in that it addresses the difficulty in removing the beads in a chain from the intamedullary cavity. The use of a hook-shaped intramedullary guidewire for extracting a broken cement rod would be limited by the narrow space between the wall of the cavity and the rod, and the bottom of the rod would also be too distant to reach with the hook. However, because our technique with the use of a hooked guidewire and intramedullary beads makes bone fenestration and additional incision unnecessary, it may prevent post-operative pain and the concentration of stress on the bone in the area of fenestratation.
In conclusion, the hook-shaped intramedullary guidewire described in this report can be used to remove an antibiotic-impregnated cement-bead chain from the intramedullary cavity of long bones without the need for painful and invasive additional procedures. This makes the use of such a guidewire a favorable choice for treating intramedullary infection. In particular, it allows an antibiotic-impregnated intramedullary cement-bead chain to be used over a longer period by reducing the risk of complications related to removal of the beads in the chain.
Footnotes
Acknowledgement and Author Disclosure Statement
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by grant 2013R1A1A2007989 from the Ministry of Education. The authors have no conflicting financial interests in the work reported here.