
Abstract
Abstract
Background:
A variety of methods exist to take samples from surgical site infections for cultivation; however, an unambiguous and suitable method has not yet been defined. The aim of our retrospective non-randomized study was to compare two non-invasive techniques of sampling material for microbiologic analysis in surgical practice. We compared bacteria cultured from samples obtained with the use of the swab technique, defined in our study as the gold standard, with the indirect imprint technique.
Methods:
A cotton-tipped swab (Copan, Brescia, Italy) was used; the imprints were taken using Whatman no. 4 filter paper (Macherey-Nagal, Duren, Germany) cut into 5×5 cm pieces placed on blood agar in a Petri dish. To culture the microorganisms in the microbiology laboratory, we used blood agar, UriSelect 4 medium (Bio-Rad, Marnes-la-Coquette, France), and a medium with sodium chloride (blood agar with salt). After careful debridement, a sample was taken from the incision surface by swab and subsequently the same area of the surface was imprinted onto filter paper. The samples were analyzed in the microbiology laboratory under standard safety precautions. The cultivation results of the two techniques were processed statistically using contingency tables and the McNemar test. Those samples that were simultaneously cultivation-positive by imprint and -negative by swabbing were processed in greater detail.
Results:
Over the period between October 2008 and March 2013, 177 samples from 70 patients were analyzed. Sampling was carried out from 42 males and 28 females. One hundred forty-six samples were from incisions after operations (21 samples from six patients after operation on the thoracic cavity, 73 samples from 35 patients after operation on the abdominal cavity combined with the gastrointestinal tract, 52 samples from 19 patients with other surgical site infections not included above) and 31 samples from 11 patients with no post-operative infection. One patient had a sample taken both from a post-operative and a non-post-operative site. Coincidently, the most frequent cultivation finding with both techniques was a sterile one (imprint, 62; swab, 50). The microorganism cultivated most frequently after swabbing was Pseudomonas aeruginosa (22 cases), compared with Escherichia coli when the filter paper (imprint) was used (31 cases). The imprint technique was evaluated as more sensitive compared with swabbing (p=0.0001). The κ statistic used to evaluate the concordance between the two techniques was 0.302. Of the 177 samples there were 53 samples simultaneously sterile using the swab and positive in the imprint. In three samples colony- forming units (CFU) were not counted; 22 samples were within the limit of 0–25×101 CFU/cm2, 20 samples within the limit of 25×101–25×102 CFU/cm2, five within the limit of 25×102–25×103 CFU/cm2, and three of more than 25×104 CFU/cm2.
Conclusions:
The hypothesis of swabbing as a more precise technique was not confirmed. In our study the imprint technique was more sensitive than swabbing; the strength of agreement was fair. We obtained information not only on the type of the microorganism cultured, but also on the number of viable colonies, expressed in CFU/cm2.
I
There exist several types of sampling methods, however, there is no method accepted universally. Most authors recommend sampling from the infected site that shows the cardinal signs of local inflammation, i.e., rubor, calor, tumor, dolor, and functio laesa [2].
Samples may be taken using invasive or noninvasive methods. Invasive methods include deep tissue biopsy, curettage, and debridement. Although these methods increase validity [3], bleeding, damage to vulnerable tissues, and pain may occur [4]. Therefore, a direct and indirect imprint technique can be used as an alternative because it may provide similar information and is less traumatic.
The aim of our retrospective study was to compare two non-invasive sampling techniques used to identify the microbes of surgical site infections. The filter paper pad has been used routinely in burn clinics and centers in the Czech Republic for bacterial screening [5] but is not used routinely in surgical practice. The question was whether it would be appropriate to use this technique routinely in surgical practice; we also tried to verify its results at our surgery department during a normal day.
Patients and Methods
The study was approved by Masaryk University in Brno and the ethics committee of St. Anne's Faculty Hospital in Brno (Institutional Review Board authorized by the Czech Ministry of Health from December 2008). All patients provided written consent for participation in this study.
Between October 2008 and January 2014, we examined 177 samples from 70 patients with surgical site infections larger than 25 cm2 (42 males, 28 females). One hundred forty-six samples were from infections after surgical procedures (21 samples from six patients after operation of the thoracic cavity–chest wounds, 73 samples from 35 patients after operation on the abdominal cavity combined with surgery of the gastrointestinal tract–open abdomen, 52 samples from 19 patients with other post-operative infections not included above), and 31 samples were from 11 patients with no post-operative infections. One patient had a sample taken both from a post-operative and a non-postoperative infection.
Swabbing
Swabbing is the most practical and widely used method that produces reliable samples for microbiologic analysis. A cotton-tipped swab is used to sample the superficial infections site fluid and tissue debris, which allows a qualitative analysis of microflora (Fig. 1), including identity, but not inoculum size [6].
A cotton-tipped swab (Copan, Brescia, Italy) was used to sample.
Filter paper pads
In our study, we performed an indirect imprint by using filter paper as the transmission medium. We used Whatman no. 4 filter paper (Macherey-Nagal, Duren, Germany), cut into 5×5 cm pieces, which were sterilized in an autoclave at 120°C for 20 min and aseptically attached to a 24-h-old blood agar. The Petri dish with the filter paper expired no more than 48 h after the date of preparation of blood agar (Fig. 2).
Petri dish with blood agar and Whatman no. 4 filter paper (Macherey-Nagal, Dűren, Germany).
The blood agar and the filter paper were prepared at the Institute of Microbiology, Faculty of Medicine, and St. Anne's Faculty Hospital. To culture the microorganisms, blood agar, UriSelect 4 medium (Bio-Rad, Marnes-la-Coquette, France), and a medium with 10% sodium chloride were used.
Blood agar
Blood agar (Institute of Microbiology, FNUSA Brno, Czech Republic) was prepared by adding 5% sterile defibrinated sheep blood to agar base [7]. Blood agar allows monitoring of hemolytic qualities of the strains cultured.
Chromogenic media
These medium are used for a simple, rapid detection of bacteria using chromogenic substrates. The chromogenic mixture contains chromogenic substrates such as Salmon-GAL, X-Gal, and X-glucuronide. Certain enzymes, produced by some bacteria, cleave these substrates, resulting in different coloration of certain bacterial colonies. In our study we used the UriSelect 4 medium, a non-selective chromogenic medium for the isolation and enumeration of urinary tract microorganisms. A chromogenic medium often contains two or more chromogens, so the blend of microbes inoculated on the chromogenic medium grows in many types of colonies, differing in color and morphology. For example, Escherichia coli colonies are pink, Enterococcus colonies blue–green, and so on. Chromogenic media are often patented, and if they contain several chromophores, the exact composition of the media is proprietary [7].
Sodium chloride blood agar
Sodium chloride blood agar (Institute of Microbiology, FNUSA Brno, Czech Republic) is a selective medium for the isolation of staphylococci. It contains 10% NaCl.
We explained to the patient the reason for microbial investigation and what the procedure involved. Before a representative sample was collected, we removed any contaminating material such as slough, necrotic tissue, dried exudates, and dressing residues from the surgical site infection. If the site was dry, we moistened the swab tip with sterile saline to increase the chance of recovering organisms from the site. The swab was moved across the incision in a zigzag motion while rotating it simultaneously [8]. A representative area of the site was sampled, in our study a size of 25 cm2.
After sampling the incision by swabbing we imprinted the same area of the investigation surface onto filter paper. The filter paper was taken from the Petri dish with blood agar by a sterile forceps and applied onto the surface of the infected site (Fig. 3). After 10 sec the paper became wet and was removed and replaced in the Petri dish (Fig. 4), which was then transported to the microbiology laboratory as soon as possible (Fig. 5), at the same time as the swab. If samples could not be transported to the laboratory immediately, they were kept at room temperature.

Step 1: The filter paper is removed from blood agar using sterile forceps.
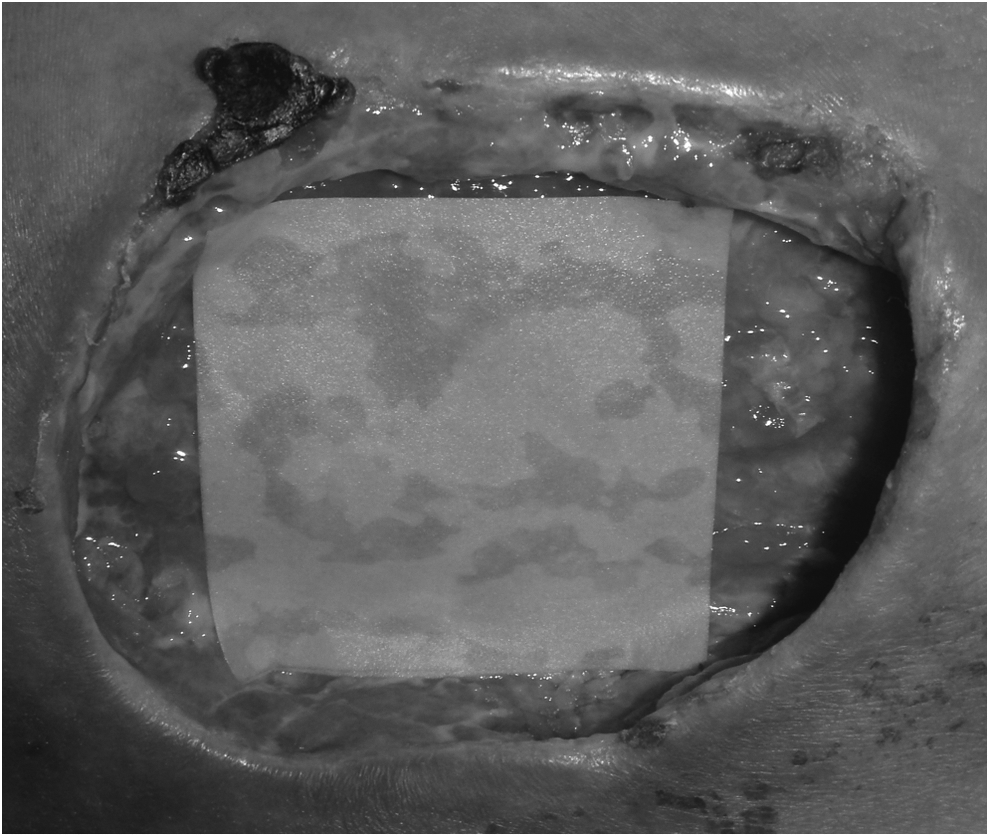
Step 2: The filter paper was left in the surgical site infection for 10 sec until it became wet.
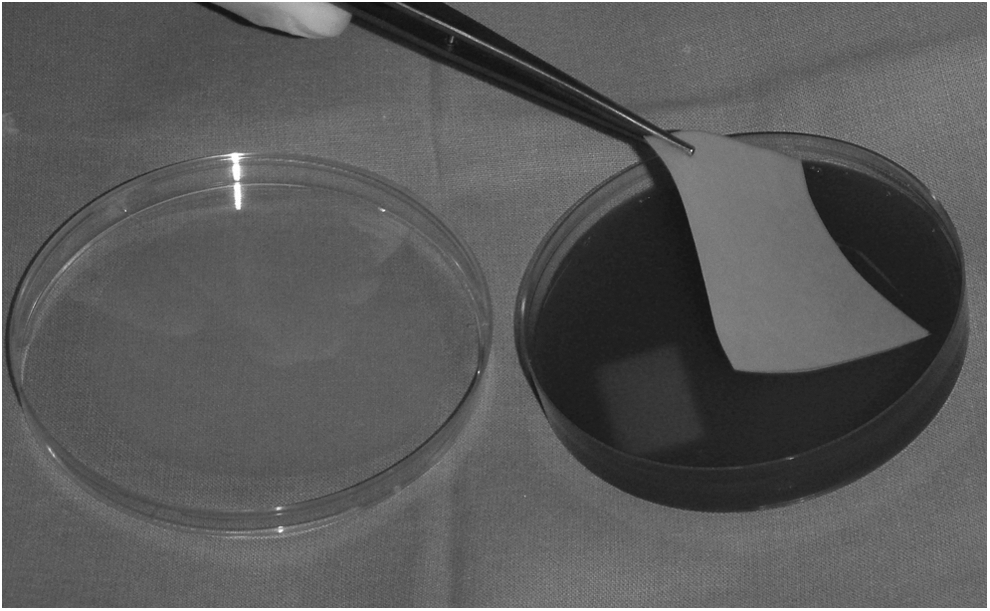
Step 3: The wet filter paper was removed from the surgical site infection to a Petri dish with blood agar, and transported to a microbiologic laboratory as soon as possible.
Microbiologic laboratory
The filter paper was removed from the Petri dish by sterile forceps (Fig. 6), applied onto a new blood agar for 10 sec (Fig. 7), then onto the UriSelect 4 medium, and afterward onto sodium chloride blood agar. The cultivation was in the atmosphere with 10% CO2 and a temperature of 37°C. The final reading of the Petri dishes was done after 48 h. The inoculation line of Staphylococcus aureus CCM 6198 was made on blood agar for a better isolation of some other microbes.

In the microbiology laboratory: Using sterile forceps the filter paper was moved from the blood agar to the UriSelect medium.
In the microbiology laboratory: The filter paper was applied onto the NaCl blood agar.
We evaluated colony-forming units per cm2 (CFU/cm2), the type of microbe, and the antibiogram. Samples obtained by swabbing provided information about the type of microorganisms; the result was qualitative compared with samples collected by imprint, which provided information about the type and density of the microorganisms and were semi-quantitative.
The colony-forming unit is an estimate of viable bacteria, whereas direct microscopy counts all cells, dead and living. The appearance of a visible colony requires growth of the initial cells plated; at the time of counting the colonies it is not possible to determine whether the colony arose from one cell or 1,000 cells. Figures 8 and 9 are examples of cultivation results.

Result of cultivation: Pseudomonas aeruginosa, Escherichia coli, Streptococcus agalactiae, Enterococcus faecalis; from left to right, on blood agar, UriSelect 4, and NaCl-blood agar.

Result of cultivation: Turquoise blue: Streptococcus agalactiae 10–100 CFU/25 cm2; pink: Escherichia coli 10,000 CFU/25 cm2; dark blue: Enterococcus faecalis 100–1,000 CFU/25 cm2; colorless to crystal clear: Pseudomonas aeruginosa 10,000 CFU/25 cm2.
Statistical analyses
All statistical calculations were done using Statistica 9.0 (StatSoft CR s.r.o., Prag, Czeck Republic) by using contingency tables and the McNemar test. The p values for each analysis were considered significant at ≤0.05.
Sterile (negative) cultivation results were designated with “−” and positive cultivation results were designated with “+”. The samples without cultured microorganisms (sterile) from swabbing and imprinting were identified as “both negative”; in statistical processing the sign “−” was given to both the swab and the imprint. In total, 46 samples were evaluated in this way. The samples with identical cultured microorganisms from swabbing and imprinting were identified as “both positive”; in statistical processing the “+” sign was given to both the swab and the imprint. In this way 68 samples were evaluated.
If the samples from the swab contained fewer microbial species than the imprint, or if the swab was sterile and the imprint was positive, the swab sample was denoted “−” and the imprint sample “+”, “swab negative and imprint positive.” In total, 48 samples were evaluated in this way.
The last option designated as “swab-positive and imprint negative” was identified with those samples where the swab contained more microbial species than the imprint, or the swab was positive and the imprint sterile, designated as swab “+” and imprint “−”. In total, 15 samples were evaluated in this way.
Results
In our study, 27 types of bacteria were cultivated by both the above-mentioned methods: Swabbing and indirect imprinting. The most frequent finding for swabbing was a sterile finding in 62 cases as opposed to 50 cases by imprinting.
At the outset of the study, only the cultivation of Staphylococcus spp., coagulase-negative, showed a higher sensitivity for imprinting compared with swabbing, but later a higher precision of imprint was confirmed in cultured strains of E. coli, E. faecalis, and S. aureus.
The microbe cultured most frequently gram-negative bacillus was Pseudomonas aeruginosa in 22 cases (swabbing) compared with E. coli in 31 cases (imprinting). The most common gram-positive bacterium cultured using a swab was methicillin-resistant S. aureus (MRSA) in 16 cases compared with the finding by imprint of E. faecalis in 22 cases. Other common cultured bacteria included S. aureus, Staphylococcus spp., coagulase-negative, and Proteus mirabilis.
The largest differences of cultivation results between the two methods was observed in sterile culture in 12 cases, followed by cultivation of E. faecalis in 11 cases and E. coli in 10 cases (Table 1).
First column, type of microorganism; second column, total count sampling by swab; third column, numerical order swab sampling; fourth column,, total count sampling by imprint; fifth column, numerical order by imprint; sixth column, difference between comparing methods.
Identical results by both culture methods were obtained in 114 samples and different results in 63 samples. The most frequent result for swabbing was a sterile result, obtained in 62 cases, whereas imprinting was sterile in 50 cases. Imprinting and the swabbing were both negative in 46 cases and both positive in 68 cases; imprinting was negative and swabbing positive in 15 cases; and imprinting was positive and swabbing negative in 48 cases (Table 2).
First column of the first row, identical positive result of both culture methods; second column of the second row, identical negative result of both culture methods; second column of the first row, swab negative and imprint positive; first column of the second row, swab positive and imprint negative.
Results of the McNemar test for a case-control study
In this study, there were 63 discordant pairs (indirect imprinting and swabbing had different results). There were 15 (23.81%) pairs in which the swab was positive against 48 (76.29%) pairs in which the imprint was positive but the swab was not.
The statistical p value of the samples after operation on the thoracic cavity–chest site infection was 0.3865; after operation on the abdominal cavity combined with the gastrointestinal tract–open abdomen, 0.0012; after other post-operative site infections, 0.0014; and after non-postoperative infections, 0.5791.
The statistical p value of all the samples treated was 0.0001; by conventional criteria, this difference is considered to be statistically significant. The hypothesis suggesting swabbing to be a more accurate diagnostic method than imprinting was not confirmed.
Result of κ indice to evaluate the concordance between the two techniques
The number of observed agreements was 114 (64.41% of the observations) and the number of agreements expected by chance was 86.8 (49.03% of the observations). κ=0.302 and standard error of κ=0.066, 95% confidence interval was from 0.172 to 0.431. The strength of agreement was considered as fair.
Of the 177 samples there were 53 samples simultaneously sterile by swabbing and positive by imprinting. Colony-forming units were not counted in three samples; 22 samples were within the limit of 0–25×101 CFU/cm2, 20 samples within the limit of 25×101–25×102 CFU/cm2, five within the limit of 25×102–25×103 CFU/cm2, and three of more than 25×104 CFU/cm2.
Discussion
In 1980 Craythorne et al. [9] published a study comparing different types of imprint techniques. The author compared the results of microbial culture from artificially infected surface by S. aureus and E. coli sampled by the Rhodac technique, the velvet pad imprint technique, the velveteen pad imprint technique, the velvet pad rinse technique, the imprint technique using filter paper pad, and tissue biopsy. The most accurate sampling method was indirect imprint technique with filter paper pad.
In 2012, Gjødsbøl et al. [10] presented the results of a study comparing the filter paper pad imprint technique with swabbing and tissue biopsy. They compared 46 samples from chronic varicose ulcers. No differences among the three sampling techniques was found with respect to the bacteria species detected.
Rusanen et al. [11] compared the imprint technique using filter paper with swabbing in the sampling of oral mucosa. Samples were taken from 14 volunteers. In this study the imprint technique captured more colonies than swabbing.
In the Czech Republic the indirect imprint technique was developed by Toršová from the Antibiotics Centre of The Health Institute in Ostrava and has now been routinely used at the burns clinics and departments of both the Czech and Slovak Republics for bacterial screening.
The most frequently isolated microorganisms from surgery site infection include S. aureus, coagulase-negative staphylococci, specifically S. epidermidis, Enterococcus spp., E. coli, Enterobacter spp., and P. aeruginosa [12]. The result of cultivation depends on the cultivation methods chosen [13]. Methicillin-resistant S. aureus (MRSA) is one of the most feared pathogens in both acute and chronic wounds [14]. Of course, there exist other pathogens causing surgical site infection, for example β-hemolytic streptococci in S. pyogenes in the lead, gram-negative bacteria, in addition to other pseudomonads, P. aeruginosa, Acinetobacter spp., which are now becoming multi-drug-resistant [15], as well as other intestinal bacilli (Enterobacteriaceae), particularly members of the genera Klebsiella and Proteus.
Different types of microorganisms are specific to a certain type of infection. For example, in a study on non-healing pressure ulcers, P. aeruginosa, Proteus spp., and Bacteroides spp. were isolated most frequently in 71% [16].
Staphylococcus aureus is the most frequently found pathogen in infections, perhaps because it is so easy to cultivate. By using new detection methods its frequency decreases somewhat, but the connection between its presence and clinical infections remains important. Also, β-hemolytic streptococci are still often associated with acute soft tissue infections [17].
The role of anaerobes should also be considered. Recent studies using modern methods for strain isolation captured Finegoldia magna, Peptoniphilus spp., Anaerococcus spp., Bacteroides spp., and Prevotella spp. in almost all chronic wounds [18].
Quantitative analysis of superficial tissue may also play a role in predicting the risk of surgical site infection [19–20]. In 1964 Bendy et al. [21] described that the clinical import of the microbial load in delaying wound healing was <106 CFU/mL of wound fluid. Robson and Heggers [22] believed that acute or chronic wound infection starts when the microbial load is >105 CFU/g of tissue. Breidenbach and Trager [23] demonstrated that the crucial level of bacteria is ≥104 CFU/g of tissue. Raahave et al. [20], using the velvet pad surface imprint technique, reported that the median infective dose of mixed aerobes and anaerobes in post-surgical infections was 4.6×105 CFU/cm2 and Majewski et al. [19], using the surface swab method, demonstrated that skin grafting was more successful in patients with an incision contamination of <5×104 CFU/cm2. In our study, 50 samples were simultaneously sterile (negative culture) by swabbing and positive by imprinting. Twenty-two samples were within a range of 0–25×101 CFU/cm2, 20 samples within a range of 25×101–25×102 CFU/cm2, five within a range of 25×102–25×103 CFU/cm2, and three more than 25×104 CFU/cm2. If we use <5×104 CFU/cm2 as the level between critical colonization and infection, only three wounds were infected and the others were colonized. We did not compare the local signs of surgical site infection with microbial density because the importance of microbial density, especially its validity, was not part of this research.
Today it no longer holds that if some potential pathogens were cultured from the wound, we have to treat the patient with an antibiotic automatically. The decision to use antibiotics to treat patients depends on many factors such as the clinical condition of the patient, associated illnesses, and total and mostly local signs of inflammation. In this case, the importance of the microbial load is not one of the main factors for using antibiotics but rather helps us to change the local antiseptic therapy. This information is valuable when a re-suture of a per secundum healing infection is needed. If the load of the microorganisms is more than 101 CFU/cm2, the planned re-suture is delayed until the imprint was sterile. The value of density information is shown in the opportunity to see the dynamics of the microbial population in the infected surgical site, whereas swabbing provides information only about the presence and absence of the pathogen against the imprint, which enables us to monitor the microbial population in the wound in real time.
According to statistical calculations, the statistical p value is less than the significance level (in our study p=0.0001). The hypothesis that swabbing provides more accurate results than imprinting was not confirmed. The indirect imprint technique using filter paper as the transmission medium is a more accurate sampling method than swabbing. The κ statistic to evaluate the concordance between the two techniques was 0.302; the strength of agreement was considered to be fair.
The disadvantages of the indirect imprint technique using filter paper include a shorter exposure time, the need to prepare Petri dishes with filter paper the day before use, the need to refrigerate for storage, and, use sterile forceps for sampling. However, imprinting is more accurate compared with swabbing and provides information about the microbial density in the surgical site infection in real time. Despite all the drawbacks associated with the imprint technique, we recommend it for use in surgical practice.
Footnotes
Author Disclosure Statement
No competing financial interests exist.