
Abstract

A 62-
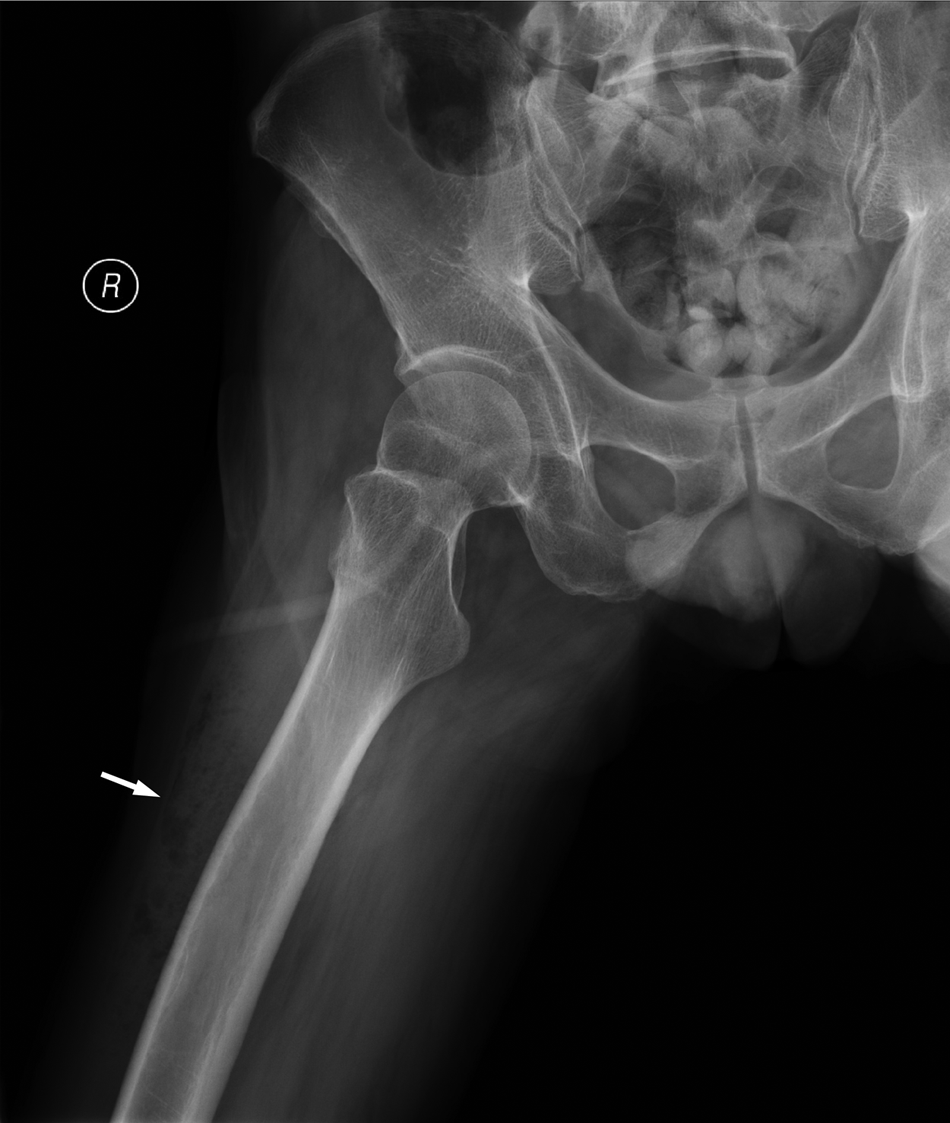
Plain radiography of the right hip revealing soft tissue gas in the right thigh (arrow).
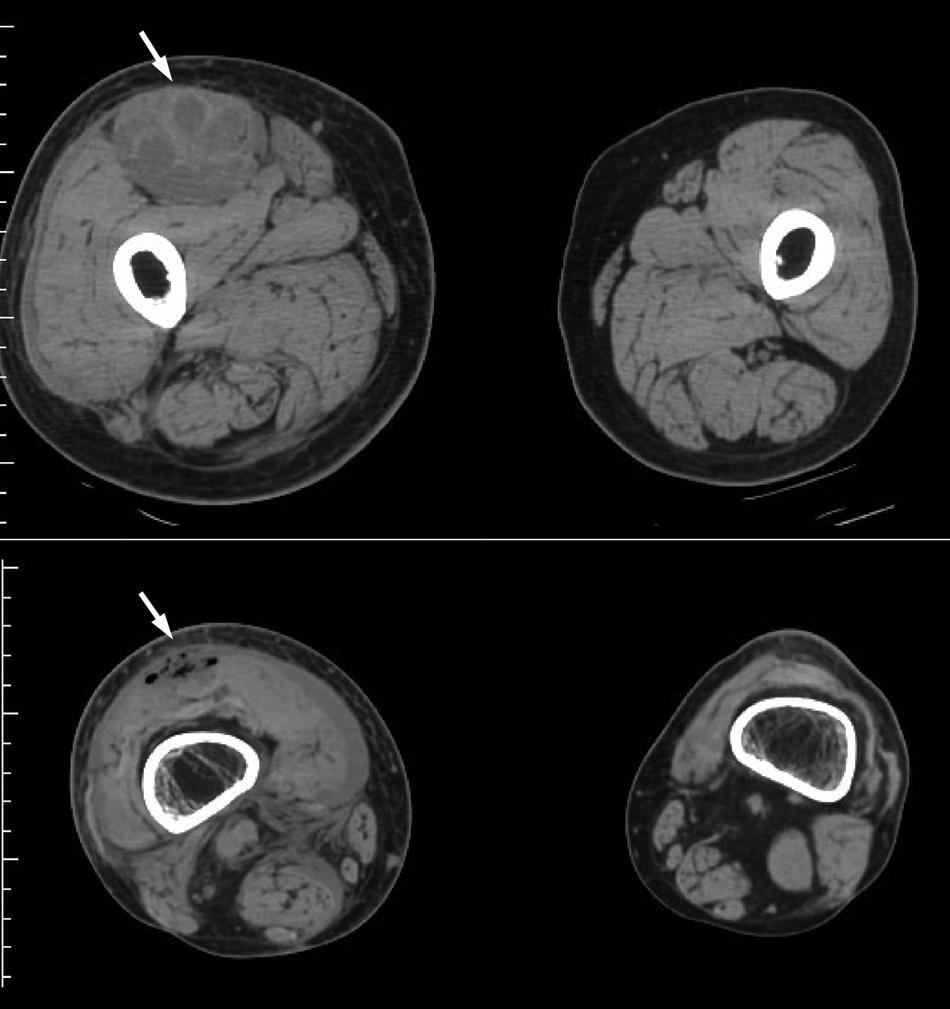
Non-contrast computed tomography of bilateral thighs showing a swollen right rectus femoris muscle with areas of low attenuation and gas formation (arrows), and atrophy of left thigh muscles.
Pyomyositis, a rare clinical entity, is a bacterial infection of skeletal muscle and the primary form is believed to be a complication of transient bacteremia [1]. Staphylococcus aureus is the most common causative pathogen, followed by streptococci; by contrast, gram-negative bacilli are relatively uncommon [1,2]. The most frequent site of infection is the quadriceps muscle, followed by the gluteal and iliopsoas muscles [1]. The reported mortality of primary pyomyositis ranges from 1 to 8%, depending on the baseline comorbidities; furthermore, patients in a later stage who present with sepsis, hemodynamic compromise or organ dysfunction have a higher mortality rate [2,3]. The standard treatment of pyomyositis includes antibiotic therapy and immediate drainage of the purulent material, especially in patients presenting with sepsis [1]. For this reason, early diagnosis is of considerable importance and a high index of suspicion is required because there may be a lack of change on overlying skin [2]. Screening plain radiograph might show soft tissue gas but its utility is limited by the low sensitivity [1]. On the other hand, CT and magnetic resonance imaging (MRI) would provide a better illustration, and the diagnostic performance of CT is non-inferior to MRI [4]. The CT findings of pyomyositis are characterized by fascial air, muscle enlargement with heterogeneous attenuation, focal fluid collection, and ring enhancement after injection of contrast medium [4,5]. In our case, contrast medium was avoided because of impaired kidney function and the changes in CT attenuation were relatively faint but identifiable. To summarize, early recognition by CT imaging and aggressive surgical debridement are crucial for pyomyositis. Although the majority of cases are caused by gram-positive bacteria, broad-spectrum antibiotics are necessary pending final culture reports.