
Abstract
Abstract
Background:
There are several studies regarding risk factors affecting surgical site infections (SSIs); nevertheless, there are an insufficient number of studies focusing on risk factors for SSI in hepatobiliary (HPB) surgery. In this study, we aimed to determine risk factors related to HPB surgery.
Methods:
A total of 1,418 patients were included in this study, all of whom underwent hepatobiliary system surgery in a five-year period between January 2005 and December 2009. Demographic data, patient- and surgery-related risk factors, and laboratory parameters were analyzed retrospectively from a database maintained prospectively.
Results:
The overall incidence of SSI was 3.94% for HPB surgery. In multivariable analysis, blood transfusion (OR: 20.9), the presence of surgical drains (OR: 10.7), a pre-operative hospital stay of more than eight days (OR: 8.1), diabetes mellitus (OR: 6.2), chronic obstructive pulmonary disease (OR: 6.127), inappropriate antimicrobial prophylaxis (OR: 6), obesity (OR: 3.2), the presence of an external-internal biliary drainage catheter (OR: 2), and a direct bilirubin concentrations more than 15 mg/dL (OR: 1.4) were determined as independent risk factors related to SSI. E.coli and Enterococcus spp. were the pathogens isolated most commonly in SSIs.
Conclusions:
Most of the independent risk factors for hepatobiliary system surgery are similar to those for other general abdominal surgical procedures. The presence of an external-internal biliary drainage catheter and direct bilirubin concentrations higher than 15 mg/dL were found to be specific risk factors for HPB surgery.
B
Development of SSI after a surgical intervention is associated with the characteristics of the microorganism, perioperative factors and patient-related factors [1,4]. Most of the isolated pathogens related to SSI are endogenous flora bacteria. However, in recent years, the role of causative bacteria in SSI seems to be shifting. Some recently published reports have shown that E.coli and Enterococcus spp. are the agents isolated most commonly in SSIs [5,6]. We observed similar findings in a surveillance study of our clinic over six years (unpublished data).
Bile prevents bacterial overgrowth in the intestinal lumen by its detergent effect. Bile has trophic effects for the intestinal mucosa, the main source of secretory Ig A. It is normally sterile, but it can be colonized by bacteria when there is a gallstone or obstruction to bile flow [7]. In the case of biliary obstruction, increasing bile duct pressure causes bile reflux into the venous and lymphatic systems [8]. This may lead to the development of systemic sepsis. Although jaundice can be treated with external or internal biliary drainage, it has been shown that biliary drainage may cause bactibilia and fungal colonization, consequently increasing post-operative sepsis and SSI rates as well as length of hospital stay. The agents isolated most commonly in bile cultures are gram-negative aerobic bacteria in patients treated with biliary drainage (in particular, E.coli and Klebsiella spp.) [9,10].
Several previous studies have determined risk factors for SSI for colorectal and cardiovascular surgery. By contrast, there is a limited number of studies investigating risk factors affecting incidence of SSI after hepatobiliary system surgery, including cholecystectomy and hepatectomy procedures. In this study, determined risk factors for SSI after hepatobiliary system (HPB) surgery.
Patients and Methods
A total of 1,418 patients who underwent one or more surgical interventions for HPB system diseases between January 2005 and December 2009 were included in this study. Patient data were analyzed retrospectively using a prospectively maintained database. We also used data, obtained from a SSI surveillance study, which has been collected continuously in our clinic starting in 2003. The Institutional Review Board of Uludag University School of Medicine approved this study (decision no: 2009-5/18, date: 17.03.2009).
Recorded data for each patient included age, gender, surgical procedure, length of preoperative hospital stay (PHS), hair removal technique, inappropriate anti-microbial prophylaxis (AMP), malnutrition, American Society of Anesthesiologists (ASA) score, emergent or elective admission, steroid usage, obesity, malignant disease, chronic obstructive pulmonary disease (COPD), diabetes mellitus (DM), incision type (subcostal, median, laparoscopy), wound class (clean, clean-contaminated, contaminated, dirty–infected), surgeon's experience (junior resident, senior resident, attending surgeon), duration of operation, placement of drains, type of skin suture material (stapler, polypropylene), use of blood transfusion, hemoglobin level, total and direct bilirubin, aspartate amino transferase and alanine amino transferase concentrations, albumin concentration, percutaneous biliary drainage catheter (external, external/internal) placement, and development of SSI. In our clinic, we use cefazolin–sodium for AMP in hepatobiliary operations, administered concurrently with anesthesia induction. We administer additional doses if the operation time is over four hours. Inappropriate AMP definition includes improper antimicrobial drug selection, administration time, and dosage (non-compliance with U.S. Centers for Disease Control and Prevention (CDC) recommendations).
The type of SSI (superficial incisional, deep incisional, organ/space), time and place of post-operative diagnosis of SSI, treatment (open wound dressing, open wound dressing and antibiotics, drainage and open wound dressing), treatment length, mortality, and morbidity rates were analyzed for patients who developed SSI. The follow up time for SSI diagnosis was 30 d after hospital discharge. The relation between SSI and risk factors was also analyzed statistically. The type of bacteria isolated from the wound culture was also determined.
Statistical Analysis
Statistical analyses were performed using SPSS 15.0 (Statistical Package for Social Sciences, Chicago, IL) package for Windows. Demographic data and risk factors were compared using the Chi-square and Fisher exact tests for categorical variables and the sample t-test for quantitative variables. To test the independence of the risk factors, the significant variables (p<0.05) in the univariate analysis were assessed using a multivariable logistic regression model with a likelihood ratio of p<0.05 (Confidence Interval 95%, Odds Ratio). Causative agents for SSI, SSI treatment type and length and the relationship between SSI and mortality and morbidity rates were documented.
Results
A SSI was detected in 56 (3.94%) of the 1,418 HPB patients (731 male, 687 female). The majority of patients with SSI were in the 45–64 years' age group (41.1%) and 51.8% were male. However, there was not a statistically significant relationship between SSI and age or gender. The frequency of operations and development of SSI in the study patients are shown in Figure 1. A SSI was most commonly detected after biliary diversion procedures at a frequency of 8.8% in these patients (p<0.001).
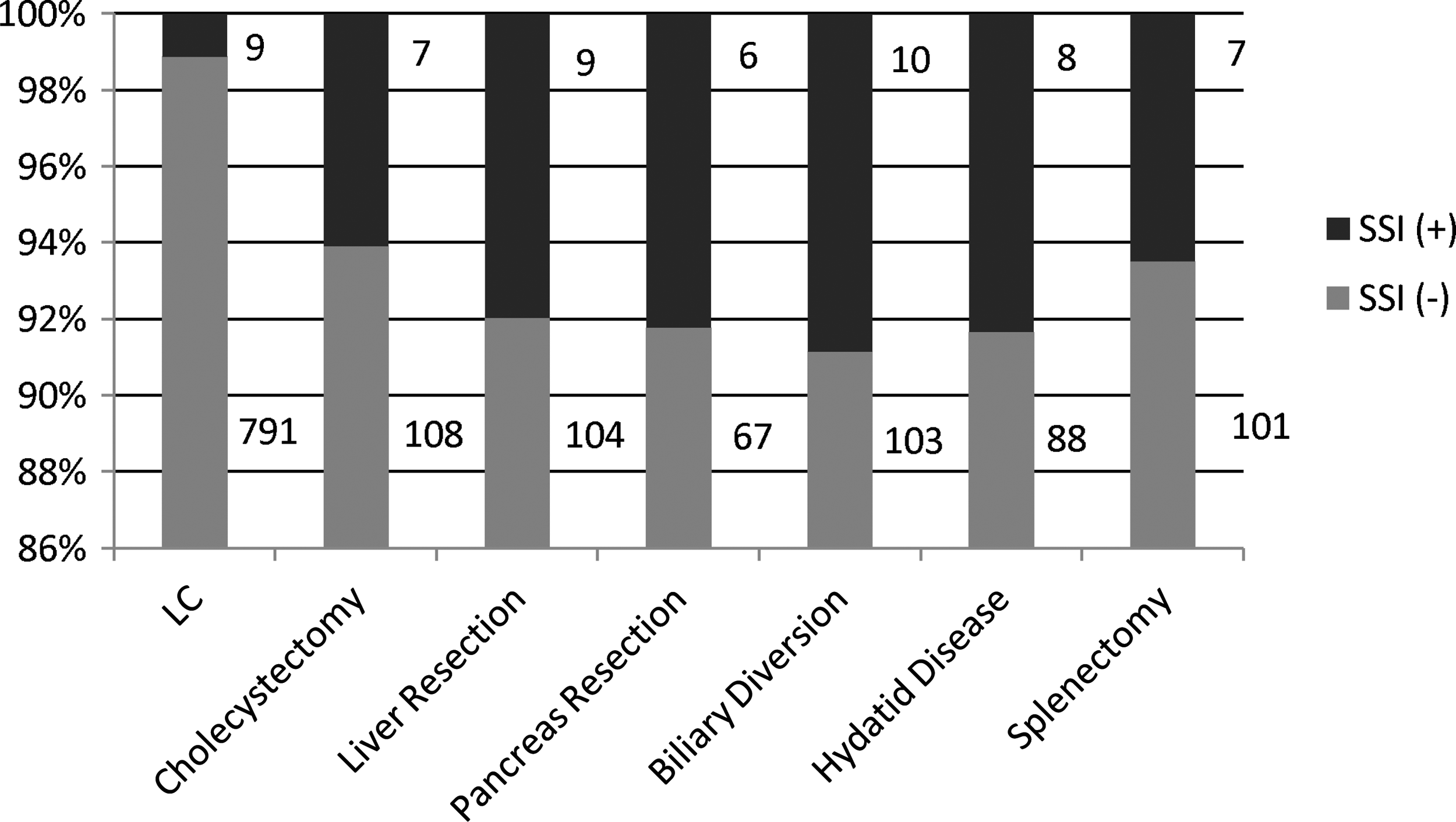
Procedure-specific SSI rates. LC=laparoscopic choleccystectomy.
The preoperative mean total bilirubin concentration was 1.4, and the mean direct bilirubin level was 0.9. Direct bilirubin concentration more than 4.8 mg/dL were associated with an increased SSI rate (p<0.001). There were 82 patients who underwent percutaneous biliary drainage (PBD), but no patients underwent endoscopic biliary drainage. SSI rates were found to be 3.2% for patients without biliary drainage, 6.3% for patients who underwent external percutaneous biliary drainage, and 47.3% for patients who underwent external-internal percutaneous biliary drainage. Of the patients with an external–internal biliary drainage catheter, enteric bacteria were determined to be the causative pathogen in seven cases (77.7%).
All risk factors except age, gender, steroid usage, smoking, and albumin concentration were found to be statistically significant risk factors for SSI by univariate analysis (Table 1). Increased SSI risk was associated with receiving perioperative blood transfusion (OR: 20.9), drain placement (OR: 10.7), pre-operative length of hospital stay more than eight days (OR: 8.1), DM (OR: 6.2), COPD (OR: 6.1), inappropriate AMP (OR: 6), obesity (OR: 3.2), external–internal biliary drainage catheter placement (OR: 2), and pre-operative direct bilirubin level over 15 mg/dl (OR: 1.4) by multivariable analysis (Table 2).
PHS=Pre-operative hospital stay; AMP=antimicrobial prophylaxis; COPD=chronic obstructive pulmonary disease; DM=diabetes mellitus; PBD=pre-operative percutaneous biliary drainage.
(*)=Standard reference; OR=Odds ratio; CI=Confidence interval.
The cases of SSI were distributed as 55.4% superficial incisional, 35.7% deep incisional and 8.9% organ/space; SSI was detected most frequently (85.7%) during the third through seventh post-operative days. However, in one patient, SSI was detected after post-operative day 14. The overall mortality rate was 2.7% (n=39), and the mortality rate among patients who developed SSI was 17.85% (n=10). The overall morbidity rate was 17% (n=240). The morbidity rate was 46.4% for patients with SSI and 15.7% for patients without SSI. The rate of SSI was significantly higher among patients who developed morbidity and mortality than among those who did not (p<0.0001).
For treatment of SSI, five patients required percutaneous drainage, antibiotic drugs were given to 30 patients, and 21 patients were treated with only open wound dressing. Forty-two (75%) patients were hospitalized for treatment of SSI. The treatment period lasted a median of seven days (range 5–16 days). We obtained wound cultures from all patients; in 11 patients, the culture was negative. Isolated pathogens are shown in Table 3.
Discussion
As an important cause of mortality and morbidity, SSI is responsible for 77% of deaths in patients undergoing surgical operations [11]. Previously reported SSI rates range from 8.8 to 34% in our country [3,12,13]. We detected an SSI rate of 7.5% in the first year and 4.1% in the last year of the SSI surveillance study administered in our clinic between 2003 and 2009. The lower SSI rate (3.94%) found in this study is due to, in our opinion, the impact of the SSI surveillance study (unpublished data) and our specialized hepatobiliary surgery team.
A strong risk factor for SSI was a prolonged length of pre-operative hospital stay, causing colonization by pathogens and increasing nosocomial SSI rates. In the study completed by Garcia et. al [14], which included 2,237 cases, the SSI rate increased 1.1 times for every three-day-long prolongation of hospital stay length. In our study, we detected that the SSI rate increased 8.1 times if the hospital stay length exceeded eight days.
It has been reported that SSI rates decrease from 10.8% to 2.8% over a one-year period with the initiation of pre-incision antibiotic prophylaxis in patients undergoing caesarean section [15]. Another study suggests that reduction of inadequate perioperative antibiotic prophylaxis would reduce the observed SSI rate [16]. In our study, we detected that inappropriate AMP administration increased the rate of SSI. We believe that this finding is convincing evidence for the importance of appropriate dosage and administration time for antimicrobial prophylaxis.
It has been reported that both a body weight exceeding 20% over ideal weight and subcutaneous fat tissue thickness are correlated with increased SSI rates [17]. In our study, obesity was found to be an independent risk factor for SSI, increasing SSI rates 3.2-fold. However, we did not find obesity to be a risk factor for SSI in a previous study from our department [18].
We did not detect a significant association between smoking and SSI in our study. However, we did detect a statistically significant relationship between COPD and SSI, and COPD was shown to be an independent risk in multivariate analysis. Additionally, DM was reported as an independent risk factor in previous studies [11]. In our study, we determined DM to be an independent risk factor in accordance with the literature.
Foreign materials used in operations provide a suitable environment for microorganisms. It has been reported that drain placement via the incision site increases SSI rates, though closed negative-pressure drains were associated with lower SSI rates [11]. Although we did not place drains through the incision, drains may allow for a two-way flow to the surgical site. In the study of Pessaux et al. [19], the presence of drains was shown to be an independent risk factor for SSI, which is consistent with our findings.
Perioperative blood transfusion is related to an immunosuppressive effect, and it is suggested that perioperative transfusion increases SSI rates five to six times [20]. We determined that perioperative transfusion significantly increased the SSI rate, and it was found to be an independent risk factor for SSI. The relationship between perioperative transfusion and SSI is an important consideration for prevention of SSI.
A serum total bilirubin concentration more than 1 mg/dL and an albumin level lower than 3.5 gr/dL were shown to be independent risk factors for SSI in the study conducted by Neumayer et al. [21]. In our study, a direct bilirubin concentration more than 15 g/dL was determined to be an independent risk factor, increasing the SSI rate 1.4 times in our study. In patients with obstructive jaundice, bile can be colonized easily by microorganisms as enterocytes cannot utilize the trophic effects of bile. Percutaneous biliary drainage (PBD) is performed frequently for patients with obstructive jaundice and cholangitis. It has been reported that pre-operative biliary drainage is associated with increased post-operative sepsis risk, development of SSI and prolonged length of hospital stay [10]. In a review, it was reported that SSI rates are increased in patients with PBD catheter because of positive bile cultures [22]. In our study, we determined external–internal PBD catheter placement is an independent risk factor for SSI, increasing SSI rates by two times. We believe that the increased SSI risk associated with external–internal PBD catheter, similarly to endoscopic drainage, is related to the ascending translocation of enteric microorganisms into the bile. Additionally, the isolated pathogenic microorganisms in these patients were mostly enteric bacteria.
The pathogenic microorganisms isolated from the surgical site wound cultures were 20% S. aureus, 17.8% E. coli and other enteric bacteria consecutively in a study conducted by Kaya et al. [3], and no microorganisms were isolated in 17.8% of samples. In our study, isolated pathogens were mostly enteric microorganisms as E. coli (14.3%), Enterococcus spp. (14.3%) and coagulase-negative staphylococci. (12.5%). In 19.6% of samples, we could not isolate a pathogenic microorganism. Our clinic is a referral center for our region; therefore, many patients are admitted to our department from other hospitals. We believe that this is the cause of the dominance of gram-negative pathogens in the hospital flora and of the antibiotic resistance of these pathogens.
The major limitation of this study is its retrospective nature. Although prospective patient data from our departmental SSI surveillance study were also included, patients' charts were reviewed to identify additional laboratory and clinical information. Another limitation may be that most of the study cohort consists of laparoscopic cholecystectomy patients. It is accepted widely that a laparoscopic approach is associated with low SSI rates, and including those patients may cause a selection bias by reducing the overall SSI rate. However, we preferred to include those patients in the study because laparoscopic cholecystectomy is a common hepatobiliary procedure. National Healthcare Safety Network (NHSN) risk index is a simple scoring system predicting SSI risk, and it includes three dichotomous variables: ASA score (3,4, and 5), wound class (contaminated, dirty–infected), procedure duration in minutes (>75th percentile). Each risk factor represents one point, and NHSN risk index varies from zero (lowest risk) to three (greatest risk) [23]. Unfortunately, operating time data were documented categorically in this study. We were unable to calculate NHSN risk score; that would certainly have strengthened the clinical value of this research.
We investigated many risk factors in our study, only external–internal PBD catheter and a direct bilirubin concentration more than 15 mg/dL were determined to be hepatobiliary surgery specific risk factors for development of SSI. We conclude, PBD catheter placement is not recommended for patients with obstructive jaundice unless the patient has an anticipated prolonged waiting time to operation. However, the SSI rate can also be decreased by the placement of biliary drainage catheters only for appropriate indications and by waiting until sufficient time has passed for bile to flow into the intestinal lumen and for correction of serum bilirubin concentrations. If PBD catheter placement is desired for a short time period, utilizing external biliary drainage should result in lower SSI rates. Major surgical procedures are frequently performed in patients with obstructive jaundice undergoing hepatobiliary surgery, and these patients often have multiple risk factors for SSI. Nevertheless, further studies are needed to evaluate the relationship between SSI and pre-operative biliary drainage types, as we detected a hepatobiliary surgery-specific risk factor in our study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.