
Abstract
Abstract
Background:
Daptomycin is used increasingly to treat prosthetic joint infection (PJI). A possible side effect of this drug is eosinophilic pneumonia. We describe two patients with PJI treated with daptomycin who had this side effect with different clinical presentations.
Methods:
Case reports and review of the literature.
Results:
The first case was a 64-year-old male who received daptomycin as a part of the treatment for PJI caused by methicillin-resistant Staphylococcus epidermidis (MRSE). He developed fever without other symptoms; bronchoalveolar lavage (BAL) revealed eosinophils. The second was a 61-year-old male who also used daptomycin as part of the treatment of PJI caused by MRSE and developed severe lung symptoms. Bronchoalveolar lavage and pleural fluid showed an increased number of eosinophils.
Conclusion:
Daptomycin-induced pneumonia can present with a wide range of symptoms, from fever alone to severe lung symptoms. Surgeons should be aware of this possible side effect when prescribing daptomycin.
D
Case Reports
Case 1
A 64-year-old male with a body mass of 88 kg was hospitalized for treatment of chronic infection of his left total hip prosthesis implanted five years earlier. The medical history was not notable except for sinus bradycardia and bilateral implantation of hip prostheses. In particular, there was no history of lung or rheumatic disease, and he had never smoked tobacco. To treat the chronic PJI, a two-stage left prosthesis exchange was performed. At the first stage, the prosthesis was removed, and an articulating spacer impregnated with 4 g of gentamicin and 2 g of vancomycin in 40 g of cement was implanted. Empiric treatment with amoxicillin–clavulanic acid (2.2 g intravenously [IV] q 8 h) was started after first-stage surgery. This treatment was switched two days later to daptomycin (10 mg/kg IV q 24 h) after the culture results showed a rifampin-susceptible and methicillin-resistant Staphylococcus epidermidis (MRSE) in the periprosthetic tissue and sonication fluid [2] of the extracted prosthesis. Daptomycin was administrated because of a presumed previous allergic reaction to vancomycin and was planned to be used for six weeks until re-implantation. Four weeks into treatment, fever of 38.5° C developed, and the general health of the patient was reduced considerably. Fever persisted for the following seven days, and the physical examination did not identify the infectious focus. Laboratory tests revealed the following: White blood cell [WBC] count 14,600 mcL (normal 4–10,000,000 mcL) with 5% eosinophils (normal 1%–4%), C-reactive protein (CRP) concentration 262 mg/L (normal <10 mg/L), creatinine 83 mcmol/L (normal 62–106 mcmol/L), and creatine phosphokinase 68 U/L (normal 25–190 U/L). Prior to the start of daptomycin, the WBC count was 10,800/mcL with 3% eosinophils. A chest radiograph showed a lesion in the right upper lung (Fig. 1). Therefore, a computed tomography (CT) scan was performed that revealed diffuse bilateral patchy ground-glass opacities, predominantly in the upper part of the lungs (Fig. 2). Bronchoscopy was performed, and the bronchoalveolar lavage (BAL) fluid yielded 47% eosinophils (normal <1%). Cultures remained negative. Daptomycin-induced eosinophilic pneumonia was suspected, so daptomycin was replaced by vancomycin (1 g q 12 h IV). Fever disappeared within 24 h after the discontinuation of daptomycin, and the patient recovered completely without systemic corticosteroid treatment. The planned re-implantation (the second stage) of a left hip prosthesis was performed one week after discontinuation of daptomycin (i.e., six weeks after explantation). At followup three months later, the patient had no respiratory or other symptoms and had a functional prosthesis.

Chest radiograph of first patient shows lesion in right upper lung.
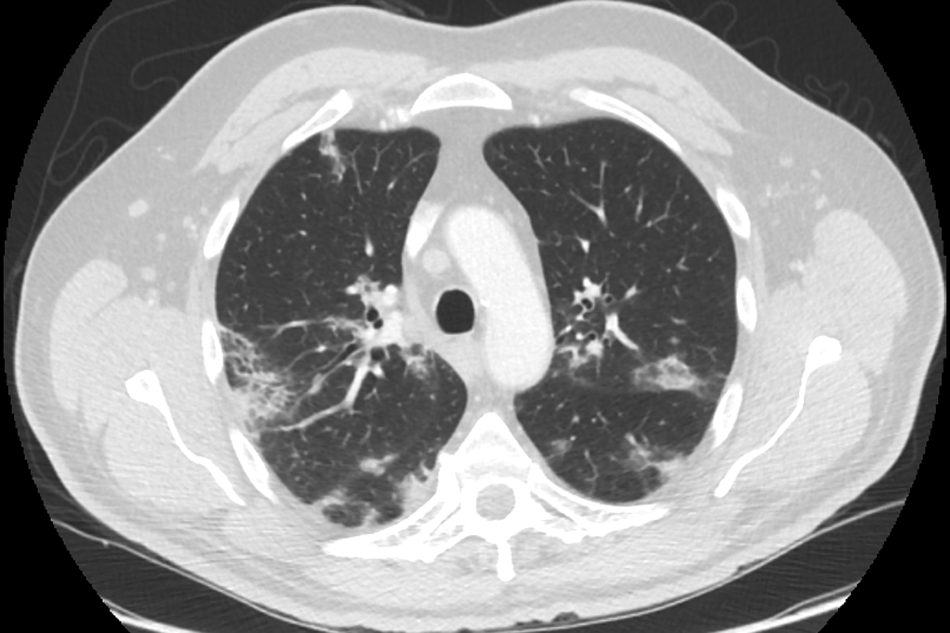
Representative computed tomography scan of chest of first patient shows diffuse bilateral densities with peripheral predominance.
Case 2
A 61-year-old male with a body mass 110 kg was admitted because of recurrent PJI of the right knee. His medical history included arterial hypertension and recurrent erysipelas. He had no history of asthma but had smoked until 10 years ago. To treat the chronic PJI, a two-stage prosthesis exchange with a short (2-wk) interval was performed with insertion of a cement spacer (articulating spacer impregnated with 4 g of gentamicin and 2 g of vancomycin in 40 g of cement). After explantation (the first stage), amoxicillin–clavulanic acid (2.2 g q 8 h IV) was started and changed one week later to daptomycin (10 mg/kg q 24 h IV) because MRSE grew from the sonication fluid of the removed prosthesis. Two weeks into daptomycin therapy (one week after the second stage where a new prosthesis was implanted), dyspnea and fever (37.7° C) developed. The WBC count was normal (8,200 mcL), C-reactive protein was increased (308 mg/L), and creatinine (79 mcmol/L) and creatine phosphokinase (52 U/L) were within normal limits. Chest radiography revealed bilateral lung opacities (Fig. 3). A bilateral ground-glass consolidation with bilateral pleural effusion was seen on CT scan (Fig. 4). A healthcare-acquired pneumonia was suspected. Cefepime (2 g q 8 h IV) and clarithromycin (500 mg q 12 h orally) were started, together with systemic corticosteroids. However, his general condition deteriorated further, with a decrease in the oxygen saturation to 62%, requiring endotracheal intubation and mechanical ventilation. Serum CRP concentration increased further, as did the WBC count. The BAL revealed 3% eosinophils and negative cultures. Peripheral blood eosinophilia (15%) was noticed, as well as 16% eosinophils in aspirated pleural fluid. Daptomycin was switched to vancomycin. The patient recovered within 24 h. At followup six months later, he had no respiratory symptoms and had normal laboratory values. There were no signs of infection of the right knee.
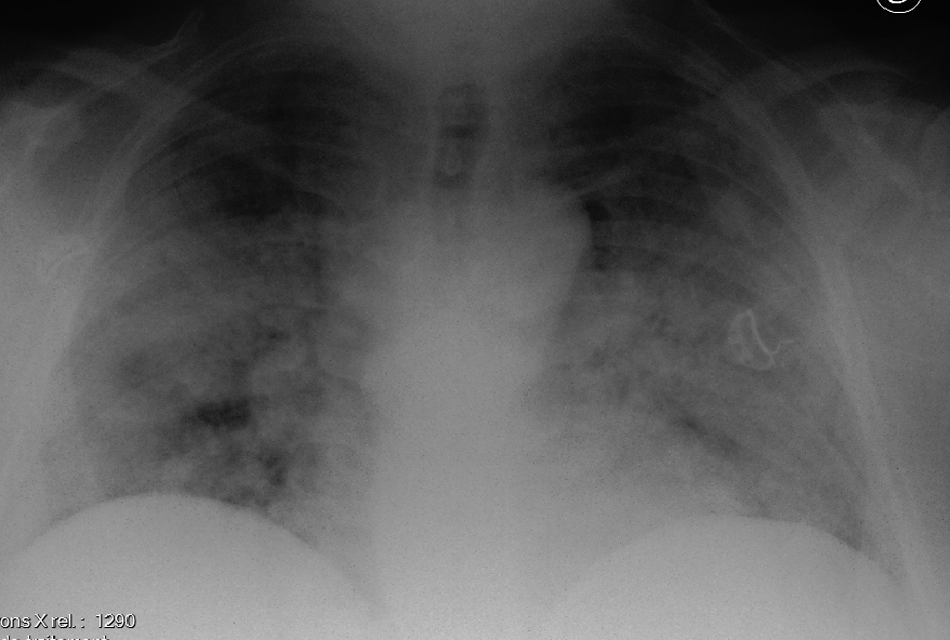
Chest radiograph of second patient reveals bilateral lung opacities.
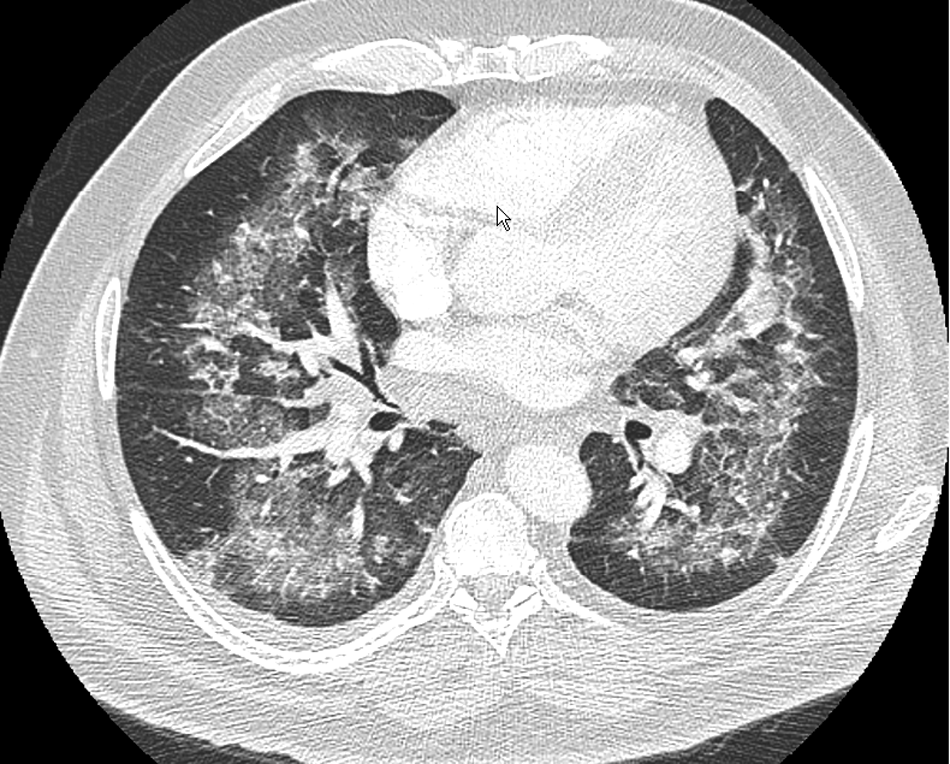
Representative computed tomography scan of chest of second patient shows diffuse bilateral densities.
Discussion
Daptomycin is an attractive antibiotic to treat infections caused by gram-positive bacteria because it is effective against many drug-resistant organisms such as methicillin-resistant S. aureus (MRSA) and because it has a low potential for resistance development [1,3]. It kills bacteria rapidly by binding to the cell membrane of gram-positive bacteria. This binding leads to the formation of potassium channels causing potassium efflux [4]. In our academic hospital, the reasons to use daptomycin in treating PJI were renal insufficiency that did not allow antibiotics such as vancomycin to be used, allergy to antibiotics such as penicillin, outpatient status ruling out IV drugs, and reduced bacterial susceptibility to vancomycin.
The primary adverse effect of daptomycin in preclinical studies was skeletal myopathy [5]. Therefore, monitoring of serum creatine phosphokinase is advised when the drug is in clinical use. Other reported adverse effects were constipation, injection site reactions, headache, and rash [6]. Here, we present two cases of novel adverse effects of daptomycin in patients with PJI. Eosinophilic pneumonia can be idiopathic or be caused by drugs, toxins, or radiation [7]. It is characterized by infiltration of the lung parenchyma with eosinophils with or without peripheral eosinophilia.
Patients with eosinophilic pneumonia usually present with fever and shortness of breath [7]. However, the first patient in this case report had only fever without any pulmonary symptoms. Perhaps eosinophilic pneumonia was detected before the lung infiltrates caused symptoms. A presumptive diagnosis of eosinophilic pneumonia can be made on the basis of increased peripheral blood eosinophils in the presence of pulmonary infiltrates [7]. In our opinion, because eosinophilic pneumonia might present without pulmonary symptoms, patients receiving daptomycin should undergo blood eosinophil counts before and several times during the course of treatment. A rise above the normal value might raise the suspicion of daptomycin-induced eosinophilic pneumonia. However, whether a rise in eosinophil count above the normal range should prompt discontinuation of the drug when the patient is asymptomatic is a matter of discussion, and the decision should be made based on individual assessment of the patient.
To make the diagnosis, eosinophils should be shown in the BAL fluid in the presence of parenchymal infiltrates. The differential diagnosis of eosinophils in the BAL fluid includes allergic bronchopulmonary aspergillosis, vasculitides, infectious diseases, and pulmonary Langerhans cell histiocytosis [8]. The medication history should prompt the diagnosis of daptomycin-induced eosinophilic pneumonia. Other causes can be excluded using laboratory tests (e.g., anti-neutrophil cytoplasmic antibodies for vasculitides) and microbiology examination (e.g., culture of the BAL fluid) [9].
The most important treatment of eosinophilic pneumonia is withdrawal of daptomycin [7]. In both of our patients, the symptoms improved within 24 h after cessation of daptomycin. In eosinophilic pneumonia, corticosteroids also can be given because they can induce apoptosis of eosinophils [10].
How daptomycin leads to this complication has not been elucidated. One hypothesis is that interaction between daptomycin and surfactant, as shown in vitro [10], might lead to a cascade that causes eosinophil accumulation in the lungs.
The incidence of daptomycin-induced eosinophilic pneumonia probably is low. In a Phase III study of daptomycin to treat complicated skin and soft tissue infection, about 2% of the patients reported respiratory symptoms such as dyspnea [6]. However, it was not known how many of those had eosinophilic pneumonia. In our surgery unit, among 72 patients treated with daptomycin (>6 mg/kg/d) between November 2009 and May 2012, two developed eosinophilic pneumonia. Several other authors have described this lung condition associated with daptomycin use [11–18]. In those studies, the majority of the patients were male. They were between 54 [18] and 87 [15] y old. The symptoms started between one [11] and five [16] weeks after initiating daptomycin treatment. The eosinophil counts in the BAL fluid ranged from 3% (our study) to 81% [16] but usually are around 3% [12,15,16] or 30% [13,14,17]. Excess peripheral blood eosinophils were found in all but two cases [14,17].
In conclusion, because daptomycin is used increasingly in treating PJI, it can be expected that more side effects will be encountered by orthopedic surgeons and other surgical specialists. Awareness of daptomycin-associated eosinophilic pneumonia is needed, especially because the clinical presentations may differ, from persisting fever to severe lung symptoms. This diagnosis should be considered in every patient receiving daptomycin who has fever or pulmonary symptoms. If this adverse effect is not recognized and daptomycin is not discontinued, serious clinical problems may occur. In contrast, if the complication is recognized, daptomycin is stopped, and the patient is treated early, as in these cases and several others [11–18], full recovery is usually obtained.
Footnotes
Author Disclosure Statement
No competing financial interests exist.