
Abstract
Abstract
Background:
Chronic pancreatitis is a painful and often debilitating disease. Total pancreatectomy with intra-portal islet autotransplantation (TP-IAT) is a treatment option that allows for pain relief and preservation of beta-cell mass, thereby minimizing the complication of diabetes mellitus. Cultures of harvested islets are often positive for bacteria, possibly due to frequent procedures prior to TP-IAT, such as endoscopic retrograde cholangiopancreatography (ERCP), stenting, or other operative drainage procedures. It is unclear if these positive cultures contribute to post-operative infections.
Hypothesis:
We hypothesized that positive cultures of transplant solutions will not be associated with increased infection risk.
Methods:
We reviewed retrospectively the sterility cultures from both the pancreas preservation solution used to transport the pancreas and the final islet preparation for intra-portal infusion of patients who underwent TP-IAT between April 2006 and November 2012. Two hundred fifty-one patients underwent total, near-total, or completion pancreatectomy with IAT and had complete sterility cultures. All patients received prophylactic peri-operative antibiotics. Patients with positive pancreas preservation solution or islet sterility cultures received further antibiotics for 5–7 d. Patients' medical records were reviewed for post-operative infections and causative organisms.
Results:
Of the 251 patients included, 151 (61%) had one or more positive bacterial cultures from the pancreas preservation solution or final islet product. Seventy-three of the 251 patients (29%) had an infectious complication. Thirty-four of the 73 (22%) patients with a post-operative infectious complication also had positive cultures. Only seven of 151 patients with positive cultures (4.7%) had an infectious complication caused by the same organism as that isolated from their pancreas or islet cell preparation.
Conclusions:
In autologous islet preparations, isolation solutions frequently have positive cultures, but this finding is associated infrequently with clinical infection.
C
Sterility testing from the pancreas preservation solution or of harvested islets are often positive for bacteria, likely caused by frequent procedures prior to TP-IAT, such as endoscopic retrograde cholangiopancreatography (ERCP), stenting, or other operative drainage procedures. As the islet cells are infused directly into the portal venous system, there is concern that any bacteria present in the transplant may increase risk of infection. It is unclear if these positive cultures contribute to post-operative infections or affect surgical outcomes. We performed the following work with the goal of evaluating the effect of culture-positive islet preparations on outcomes after TP-IAT, with the hypothesis that infusion of culture-positive islets is safe.
Patients and Methods
After approval from our internal review board, we performed a retrospective review of patients who underwent TP-IAT between April 2006 and November 2012 at our institution. During that time, 251 patients underwent total, near-total, or completion pancreatectomy with islet autotransplant. Chart review was performed to collect patient demographics, previous pancreatic interventions, total, completion, or partial pancreatectomy performed with islet transplant, and islet cell yield. The microbiologic culture data from islet preparations from all 251 patients were collected. Two samples for sterility culture were obtained from each patient. The first sample was from the pancreas transport solution, which contains the pancreas after removal and prior to islet preparation or purification. The second sample was from the solution containing the final islet preparation (including the islets) to be transplanted into the patient. Medical chart review was completed for all patients for any documented post-operative infection or other post-operative complications within 30 d of the procedure, previous pancreatic procedures, and insulin requirement post-operatively.
The criteria for selection of patients with chronic pancreatitis for TP-IAT have evolved over the years. Table 1 lists current selection criteria [14]. Contraindications include active alcoholism, pancreatic cancer, illicit drug usage, and poorly controlled psychiatric illness with predictable inability to comply with the post-operative regimen. A multi-disciplinary group consisting of surgeons, a gastroenterologist, endocrinologists, and pain management physicians and nurse coordinators reviews all patients prior to the decision to perform TP-IAT. A patient is accepted for TP-IAT after the group reaches consensus.
ERCP=endoscopic retrograde cholangiopancreatography; EUS=endoscopic ultrasound; MRCP=magnetic resonance pancreaticocholangiography.
Surgical procedure
Informed consent is obtained from all patients prior to any procedure. The patient is prepared and draped in the usual sterile fashion and all patients received pre-operative ertapenem 1 g for prophylaxis. Ertapenem is used because in addition to covering for most of the usual organisms associated with surgical infections, this procedure is performed on patients with previous pancreatic instrumentation who therefore are at increased risk of Escherichia coli and Klebsiella infections, including extended-spectrum β-lactamase–producing species, but have a low risk for Pseudomonas infection. Total pancreatectomy is performed so that the blood supply to the pancreas is preserved until just before removal; the entire pancreas is mobilized and then the origin of the splenic artery and termination of the splenic vein are ligated. In this way, warm ischemic time to the islets is minimized. In cases in which head and duodenal mobilization were difficult, the body and tail were removed separately and sent to the islet processing laboratory before the proximal portion was removed. For those without an earlier Whipple procedure, all or part of the duodenum was resected, using a pylorus-sparing technique whenever possible. In all patients, a cholecystectomy and appendectomy were performed if not done previously.
Islet isolation
After the pancreas is removed, it is placed in University of Wisconsin (UW) solution and transported on ice. Islet isolation and purification is performed in the University of Minnesota Molecular and Cellular Therapeutics GMP facility. Although modifications have been introduced throughout the years, the basic method of islet preparation has been the same over time: Dispersion of the pancreas in a stepwise fashion, first by intra-ductal injection of collagenase solution under pressure to disrupt the exocrine pancreas (islets are spared) and then digestion at 37°C in (since 1991) a shaking chamber (Ricordi method) to facilitate dispersion mechanically and free the islets as much as possible [15–17]. At the University of Minnesota, several enzyme preparations have been used throughout the years. The current enzyme mixture consists of intact C1 collagenase (VitaCyte, Indianapolis, IN) and neutral protease (SERVA, Heidelberg, Germany).
After digestion, the islets can be purified or partially purified by a gradient separation method or can be transplanted as an unpurified preparation. Islet purification is performed using density gradients in the COBE 2991 cell processor (Teromo BOT, Lakewood, Co) [18]. The decision to purify depends mainly on the post-digest tissue volume and the desire to minimize the increase in portal pressure that occurs during islet embolization to the liver [19]. Gradient purification is avoided when possible, to avoid loss of islets. Currently, a post-digest tissue volume of >0.25 cm3/kg is an indication to at least purify partially [19]. The final islet tissue preparation is suspended in 500 mL CMRI culture medium (Mediatech, Inc., Holly Hill, FL).
Islet transplantation
The final islet preparation is generally returned to the operating room 3.5 to 6.5 h (mean, 4.5 h) after the pancreatectomy. After administration of heparin (70 mg/kg intravenously), the islets are infused during a 15- to 60-min period depending on tissue volume. The larger the tissue volume, the slower the islet infusion rate in order to minimize portal pressure elevation. Currently, if the portal venous pressure reaches 30 cm H2O, the infusion is stopped and any remaining tissue is discarded or placed in the peritoneal cavity. All patients received a heparin infusion or enoxaparin post-operatively to prevent portal venous thrombosis.
Microbiology
All patient samples of both the pancreas transport and transplant (final islet product) solutions are sent for aerobic, anaerobic, and fungal culture. If an islet solution was culture-positive, the patient received intravenous antibiotic treatment for 5–7 d, either piperacillin-tazobactam and ertapenem or vancomycin to provide broad-spectrum coverage. Once final culture results were available, the broad-spectrum antibiotics were narrowed to appropriate coverage for the specific pathogens identified. Urine culture results were considered infected clinically if bacterial counts were greater than 100,000 CFU/mL. Bacteremia was defined as any bacterial growth in blood cultures (for coagulase-negative Staphylococcus, if blood cultures were positive in all bottles this was considered a case of bacteremia). Any intra-abdominal fluid collection that had positive cultures was considered an infection. If no cultures were obtained but clinical data (i.e., elevated temperature, leukocytosis, improvement with appropriate treatment) supported the diagnosis of infection this was also noted as a post-operative infection. Pneumonia was defined as a new infiltrate on chest radiograph with associated clinical signs.
Statistics
Statistical Package for the Social Science (version 19, IBM, Armonk, NY) was used to perform statistical analysis. Categorical variables were evaluated with χ2 tests and continuous variables are reported as mean values with standard deviation and were evaluated with analysis of variance (ANOVA) or the Student t-test as appropriate. Logistic regression was used for multivariable analysis.
Results
Of the 251 patients included, 152 (61%) had one or more positive bacterial cultures of either the pancreas transport solution or final islet product. Seventy-one of the 152 positive cultures (47%) were positive in the pancreas transport solution only, and the final islet product solution to be infused into the portal vein was sterile. Four of the 152 positive cultures (3%) were positive in the islet transplant solution only and were suspected to represent contamination during islet processing. Including these four newly contaminated islet solutions, there were 81 patients with culture positive final islet preparations infused into patients, with 77 (51%) having positive sterility cultures of both the pancreas transport and islet transplant solutions (Fig. 1). Enterococcus, E. coli, and streptococcal species were the most common isolates identified in the islet solutions. Three islet solutions were positive for an extended-spectrum β-lactamase–producing organism. There were no cases of methicillin-resistant Staphylococcus or vancomycin-resistant Enterococcus (Fig. 2). There were five cases (3%) of fungal growth found in the islet solutions (Candida albicans, C. glabrata, C. dubliniensis, and yeast). Two of these were only identified in the pancreas transport solution with sterile final islet products, two had fungal growth in both solutions, and the final case was a new contaminant identified in the final transplant solution after the transport solution was sterile.
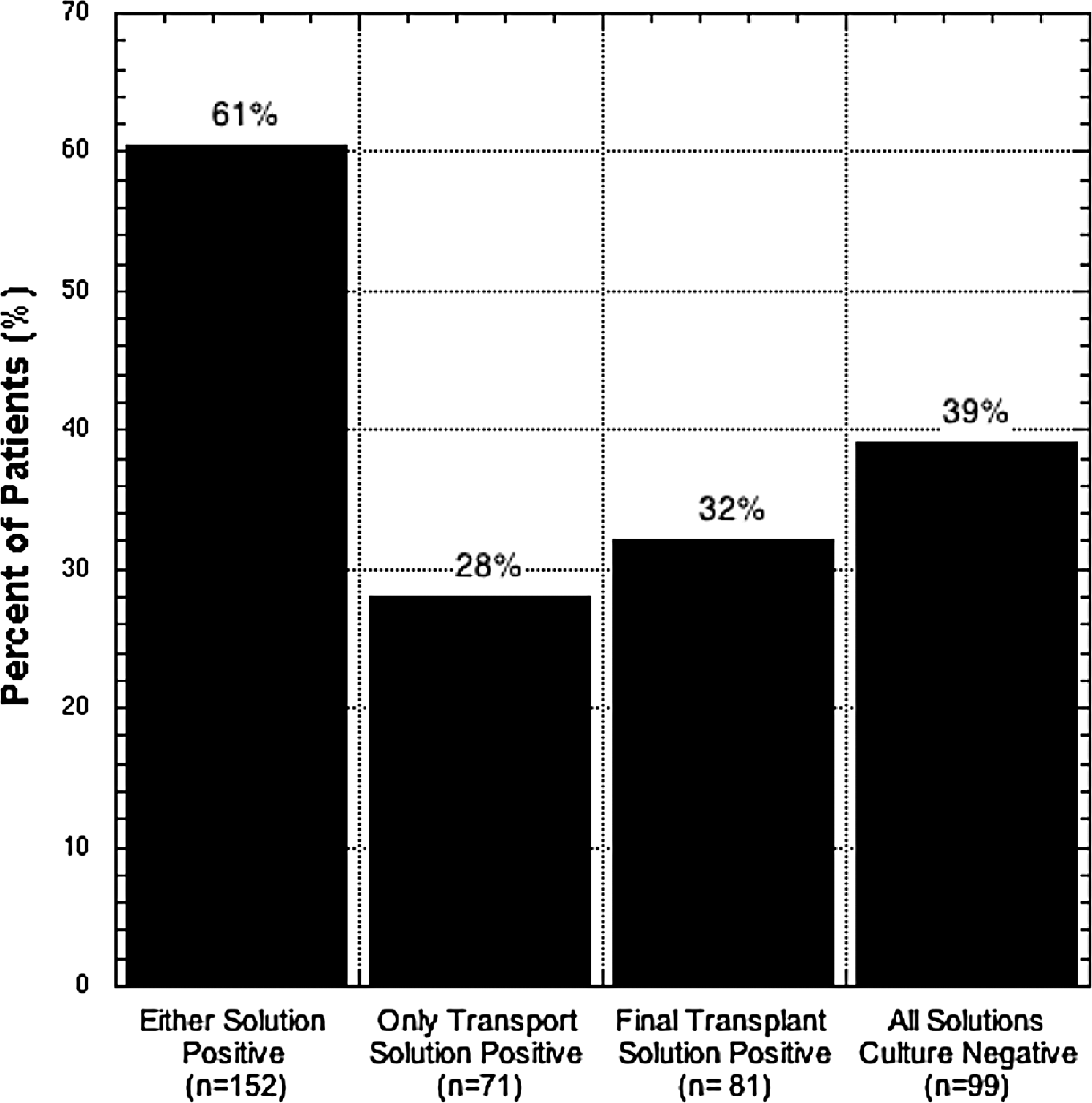
Islet solution culture results. The majority of patients had one or more positive cultures, 32% had culture-positive transplant islet solution infused into the portal vein.
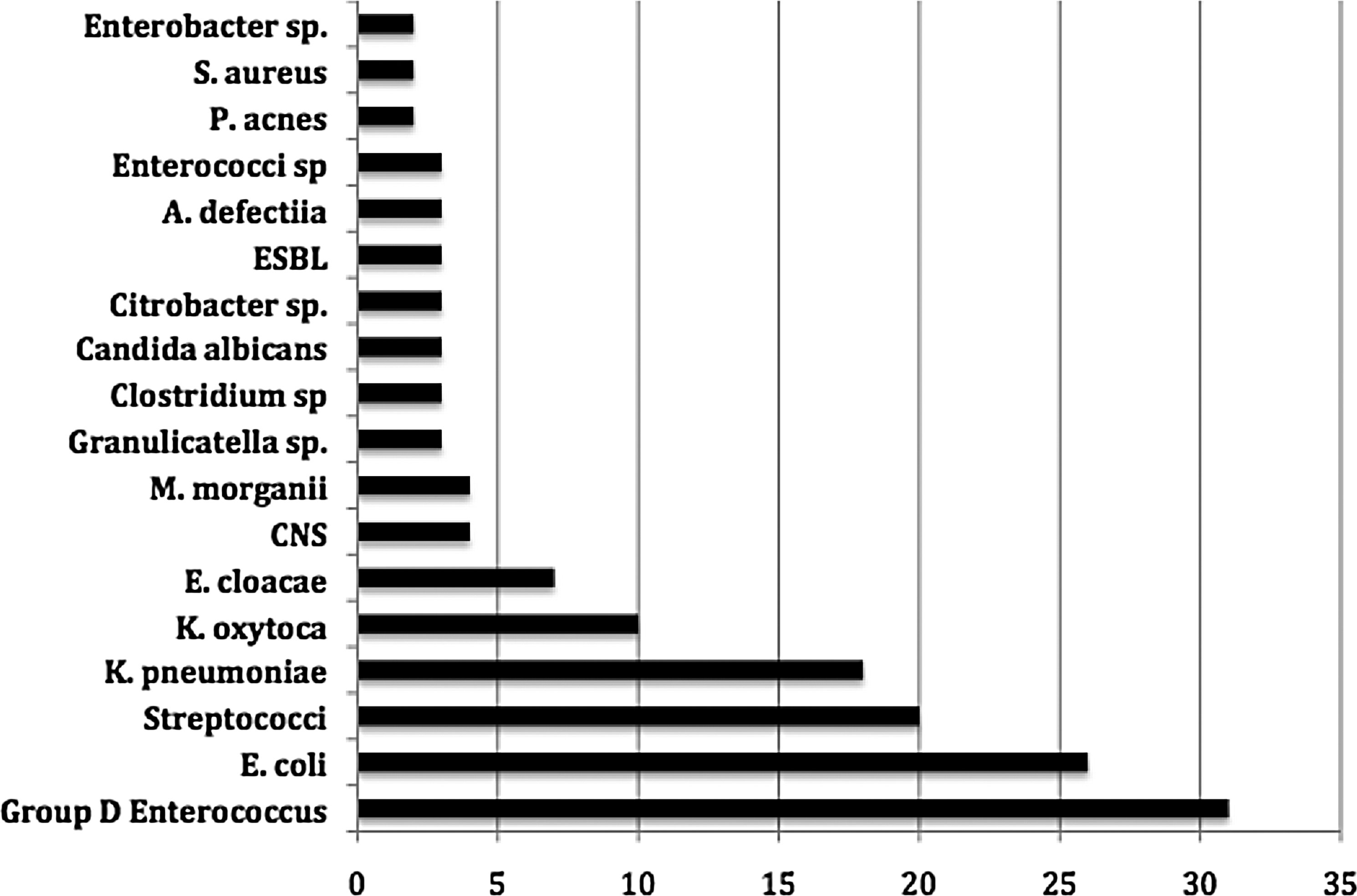
Microbiologic surveillance results of islet media solutions. CNS=coagulase-negative Staphylococcus; ESBL=extended-spectrum beta-lactamase.
For the 152 patients who had positive cultures of either the transport or the final islet solutions, age, gender, or the year of the procedure was performed were not associated with positive cultures (Table 2). Length of stay was not increased for patients with either positive pancreas transport or final islet product cultures. Most patients (91%) had undergone some pancreatic intervention (ERCP, pancreatic drainage procedure, Whipple procedure, or partial pancreatectomy) prior to total pancreatectomy. Of the patients with previous pancreatic intervention, 63% had positive cultures, compared with 27% of patients who underwent no previous intervention (odds ratio [OR] 3.21; 95% confidence interval [95% CI] 1.3–7.9; p=0.008). We then analyzed each group, those who had undergone no prior procedures, those who underwent only ERCP, and those who underwent a pancreas drainage procedure, and found that there was a significantly increased risk of having positive islet sterility islet solution cultures in those undergoing either previous drainage procedure or ERCP (Table 3). The mean islet yield was lower in patients with any positive cultures (3,458 islet equivalents per kilogram [standard deviation {SD} 2,275) versus 4,621 [SD 2,215] in those with negative cultures, p<0.001), however, this difference appears to be entirely due to the greater frequency of prior pancreatic surgery in the group with positive sterility cultures (Fig. 3). The islet yield was significantly decreased by having a prior pancreatic procedure compared with having had either no procedures or a prior ERCP (p<0.001 for both; Table 3). Positive cultures for either pancreas transport solution or final islet product did not affect the proportion of patients achieving insulin independence at follow-up. Twenty percent with positive cultures were insulin-independent at 1 y and 34.5% were independent at 2 y, compared with 19% with negative cultures at 6 mo and 35% at 1 y (p value>0.05 for both time periods).
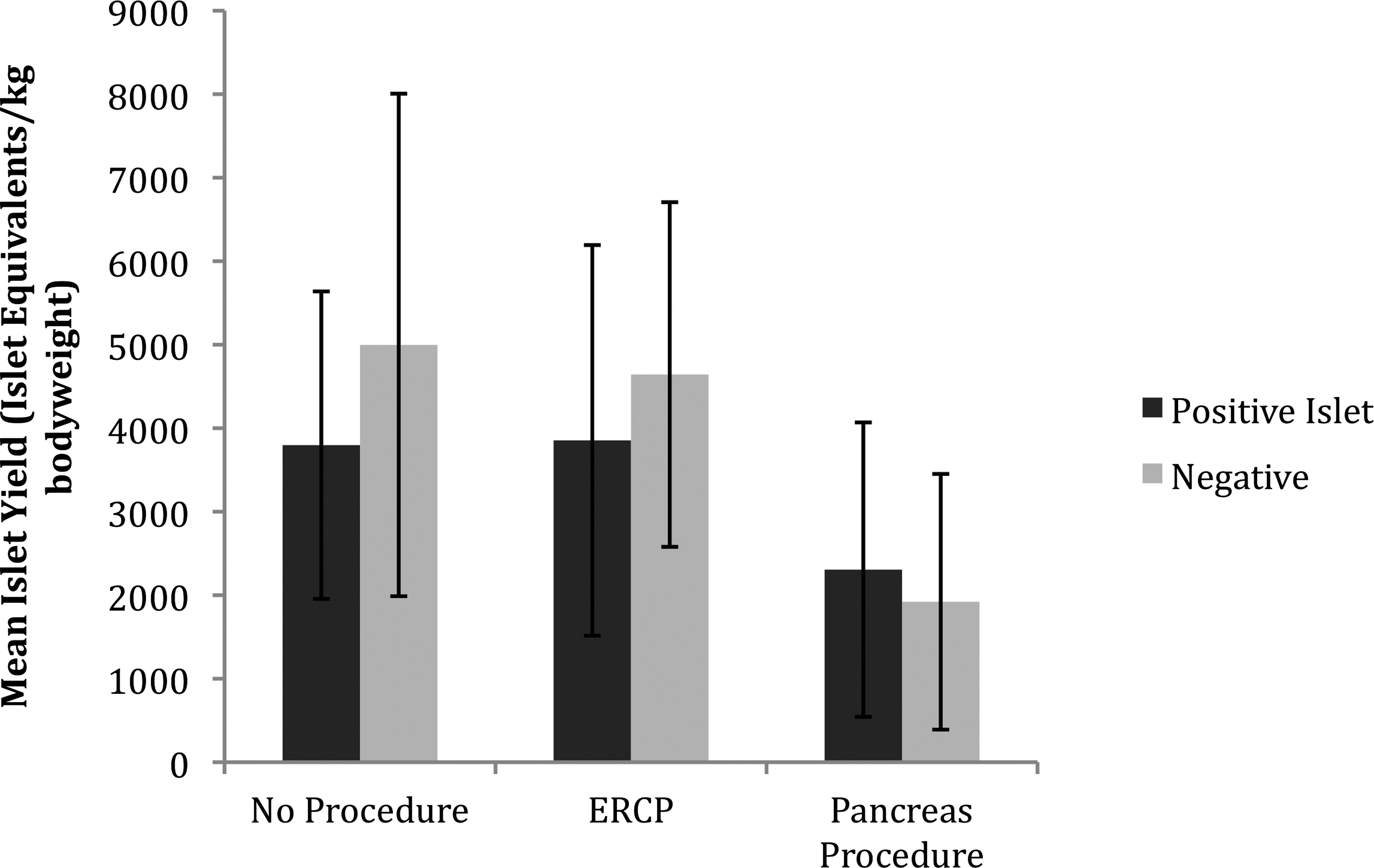
Islet yield by prior procedure and culture results. There was no difference in islet yield by culture result within each procedure. However, patients who underwent prior pancreas drainage procedure (i.e., Whipple, partial pancreatectomy, Frey procedure, or Puestow procedure) had significantly lower islet yield than the other patients (p<0.001). ERCP=endoscopic retrograde cholangiopancreatography.
ERCP=endoscopic retrograde cholangiopancreatogram
We also performed a review of the 81 patients who specifically had positive sterility cultures of the final islet product, excluding those who had only positive pancreas transport solutions with subsequent sterile islet product cultures after processing. The patients with positive cultures of the final islet product were significantly younger than those with a sterile islet product (31 y [SD 15.9] v. 36 y; [SD 12.8] p=0.007). The rate of positive transplant cultures did not differ significantly with gender or year procedure was performed. Length of stay was not increased for patients with positive cultures (16 d [SD 6] for positive cultures versus 18 d [SD 12] in negative; p=0.135). Mean islet yield per kilogram was again found to be significantly lower in patients with positive transplant cultures (2,812 islet equivalents/kg [SD 2,073] versus 3,923 islet equivalents/kg [SD 2,194]; p<0.001).
Infectious complications
Seventy-three of the 251 patients (29%) developed a post-operative infectious complication (Fig. 4). Patients who developed post-operative infections were more likely to be older (median age 39 y v. 32 y; range, 4–72 y v. 5–66 y; p=0.018). The risk of infection was not affected by gender, type of procedure, or year of procedure. Patients with infection had a longer length of stay (Table 4). Thirty-three of the patients (22%) with positive cultures in either the transport solution or final islet product developed an infection, whereas 117 patients (78%) with positive cultures in either solution did not experience any infections complication (Fig. 4). Only 12 of the 81 (15%) patients with positive cultures of the final islet product developed a post-operative infection. Having a positive culture from the islet product did not increase the risk of post-operative infection compared with those patients with negative islet cultures (OR 0.443; 95% CI 0.254–0.772; p=0.004). None of the patients with extended-spectrum β-lactamases isolated from their islet solutions developed any infection. There were 12 cases of fungal infections (six intra-abdominal abscesses, two pneumonias, two cases of bactermia, and two superficial surgical site infections). None of the fungal infections developed in patients with fungal growth in their islet solutions.

The infection rate for this procedure was 29%. Patients with positive islet solution cultures did not have a higher infection rate, in fact, the infection rate was significantly less than patients with negative islet solution cultures (p=0.004).
Fisher exact test used as sample size <5 cases, all other p values report the Pearson value for χ2.
The most common post-operative infections were intra-abdominal abscess, superficial incisional surgical site infection, and pneumonia (Fig. 5). No patient with a positive islet product culture developed an intra-hepatic abscess. Although all patients with positive sterility cultures received 5–7 d of post-operative antibiotics, we did not observe an increased rate of Clostridium difficile infections (2.6% with positive cultures v. 2.0% with negative cultures; relative risk 1.10 [95% CI 0.62–1.96] p=0.556)
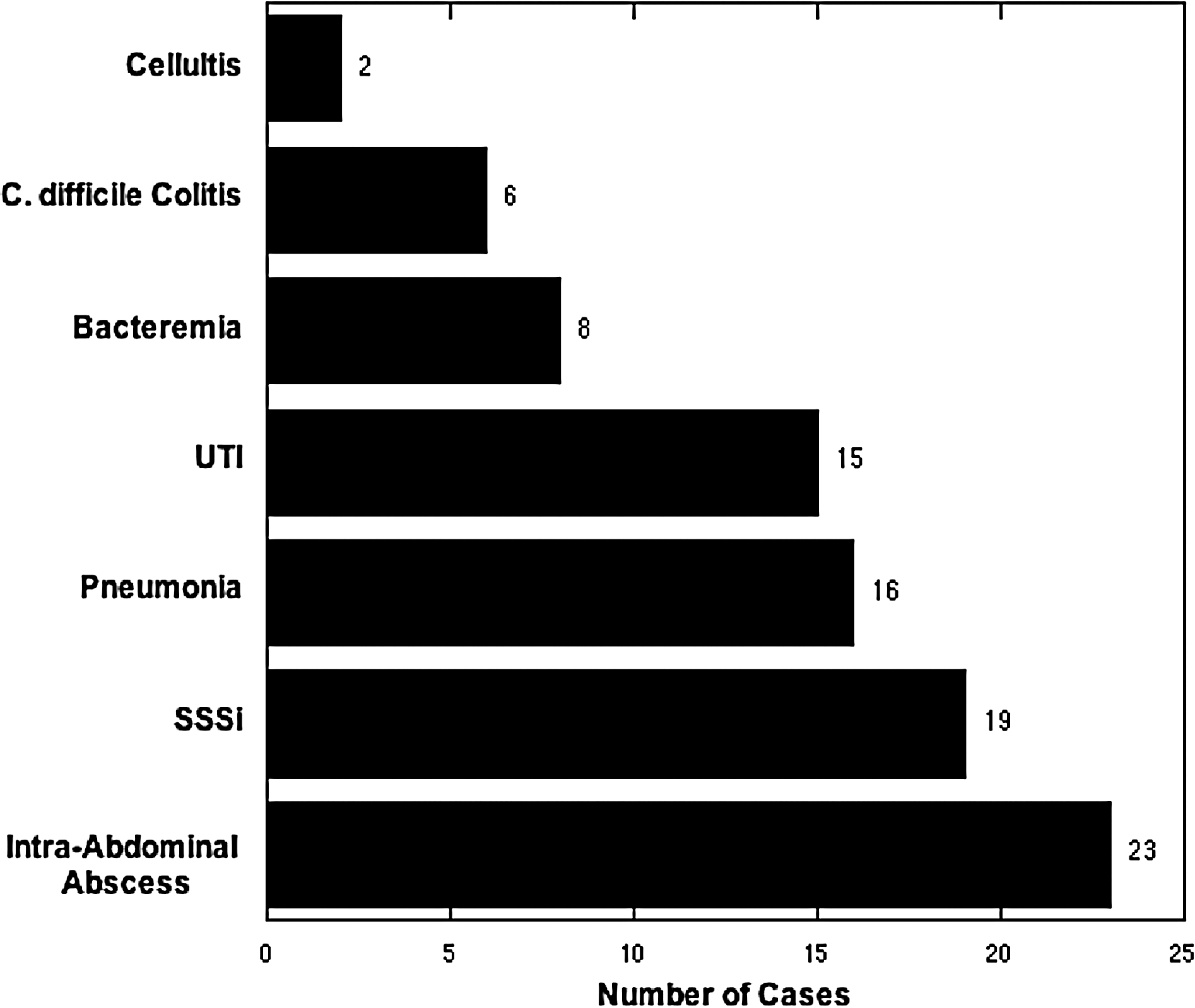
Types of post-operative infections developed after total pancreatectomy with intra-portal islet autotransplantation (TP-IAT).
Only seven patients (4.7%) had an infectious complication with concordant organisms isolated from both the pancreas transport or islet product preparations and the infectious source. These included three intra-abdominal abscesses, two bacteremias, one superficial incisional surgical site infection, and one pneumonia. Notably, three of these patients had positive cultures in the transport solution only, with the final islet solution infused into the portal vein being sterile.
Discussion
Although total pancreatectomy and islet autotransplant is an important surgical option to relieve pain for patients with severe chronic pancreatitis, post-operative infection is a frequent complication. Patients with pancreatitis are at high risk for bacterial contamination of their pancreas, particularly if multiple endoscopic interventions and lesser surgical procedures were used previously. This raises the question as to whether infusing a potentially contaminated islet product could increase the risk of serious bacterial infection in this patient population. To address this, we evaluated the incidence of microbial contamination of the pancreas and islet products and the associated risk of post-surgical infection in more than 250 TP-IAT recipients at a single center. Almost two-thirds of our TP-IAT patients had one or more positive bacterial cultures of the pancreas preservation solution or final islet product, although infectious sequelae directly related to these preparations were notably rare. Our results suggest that with proper antibiotic coverage and monitoring, infectious complications resulting from the islet autotransplant portion of the procedure are few.
This is the largest series to date evaluating microbial contamination in autologous islet transplant preparations. The only prior series evaluating microbial contamination in islet autotransplantation for patients with chronic pancreatitis similarly demonstrated a high rate of culture-positive islet solutions, 89% in a case series of 28 patients [20]. Islet allotransplantation from cadaveric donors without chronic pancreatitis has also been reported to have bacteria present in their initial pancreas transport solutions, between 19% and 68% [21–25]. However, within the alloislet transplant population, islet processing decreases the rate of microbial contamination in the final transplant solution to zero to 16% [21–24,26]. With islet processing or autologous preparations, Wray et al. [20] reported a decrease from 89% culture positivity in the pancreas transplant solution to 64% in their final islet autotransplant products. We demonstrated a similar decrease after islet processing, with rates decreasing from 60% to 32%. Although the steps of islet manufacturing may serve to eliminate some microbial contamination, the likelihood of having a culture-positive final islet product infused back into the patient is much greater with autologous islet transplant. The higher rates of contaminated pancreata and islet products in islet autotransplants is likely because these patients have chronic pancreatitis, and underwent prior pancreatic interventions such as ERCP and other drainage procedures previously. Those factors are not present with cadaveric donors.
Most importantly, this study demonstrated no increase in the infection rate with positive cultures. The overall infection rate was 29%. This is similar to the post-operative infection rates (20%–39%) reported in other series of TP-IAT [20,27–30]. The infection rate is likely related to the complex nature of the operation and the often poor nutritional status of patients prior to the procedure. The presence of bacteria in islet solutions did not increase the rate of infection; rather, we found that the rate of post-operative infection was significantly decreased in patients with positive cultures. This may be due to the longer duration of antibiotics administered in this subgroup of patients; all patients with positive islet solution cultures received 5–7 d of antibiotics, starting with either empiric piperacillin-tazobactam or ertapenem plus vancomycin based on physician preference and initial gram stain. Antimicrobial treatment is then narrowed based on subsequent culture results. Infusion of bacterial-contaminated transplant islet solution did not increase the rate of infection, suggesting these products are safe. Our results correlate with previous results reported in TP-IAT [20] and in allogenic islet transplants [21–23,31].
We found only seven cases of post-operative infections in which congruent organisms were cultured from the islet solutions and the subsequent infection. Of these cases, three patients (one pneumonia and two intra-abdominal abscesses) had bacteria present only in the transport solution. These cases may represent colonized abdominal flora in these patients, with infection resulting from disturbing anatomy in a chronically colonized field (e.g., the manipulated pancreatic duct), rather than the infusion of the islet solution. It is also possible that these are coincidental findings; we did not have any serotype data available to confirm that the same serotype caused both infections. Other congruent cases may have been missed, as we did have cases of surgical site infections, pneumonias, and cellulitis with no culture data available.
There was significant correlation between the prior procures (ERCPs and pancreatic procedures) and greater rates of bacterial contamination. This relationship has also been reported in other studies [32,33]. This contamination of the normally sterile pancreatic duct and tissue has been hypothesized to be due to loss of the biliary sphincter, the mechanical barrier to bacterial invasion from the duodenum, or through colonization of the stents often placed [20,32–35]. Operative pancreatic drainage procedures connect the pancreatic duct directly to the duodenum losing any barrier between the gut and the pancreas leading to contamination. In addition, previous surgical pancreas drainage procedures were associated with significantly decreased islet yield. Given these findings, we strongly recommend that TP-IAT be preformed prior to these drainage procedures, as we have recommended for years.
As noted above, we continue to treat all patients with positive islet solution cultures with 5- to 7-d course of antibiotics. Although we did not find an increased rate of C. difficile infections, treating with unnecessary antibiotics leads to many undesired consequences. In a smaller series, Wray et al. [20] reported the use of 24 h of post-operative antibiotics only without prolonging antibiotics for positive islet cultures with similar infection rates to our series. As the infection rate in our work was not increased in patients with positive cultures, we believe that the appropriate next step may be to shorten antibiotic duration in the setting of positive islet preparation cultures.
These results should be interpreted within the limitations of this study. The data were reviewed retrospectively and we lack serotyping to prove conclusively the congruency infectious organisms. There was no prospective study to evaluate the impact of antibiotic prophylaxis and treatment, type, or duration of antibiotics on infection risk, and it is unclear if shortening the duration of antibiotic therapy in culture-positive patients could be safely done.
In conclusion, the majority of patients undergoing TP-IAT will have bacteria present either in the pancreas transport solution, the final islet product, or both, particularly if there is a preceding history of endoscopic or surgical therapy, however, these positive cultures do not appear to increase the risk of post-operative infections, at least in the context of appropriate antimicrobial coverage. Islet autotransplantation does not significantly increase the risk of infectious complications for patients undergoing total pancreatectomy for the management of severe chronic pancreatitis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.