
Abstract
A 44

Cladophialophora bantiana—the puncture culture on the Sabouaraud soil.
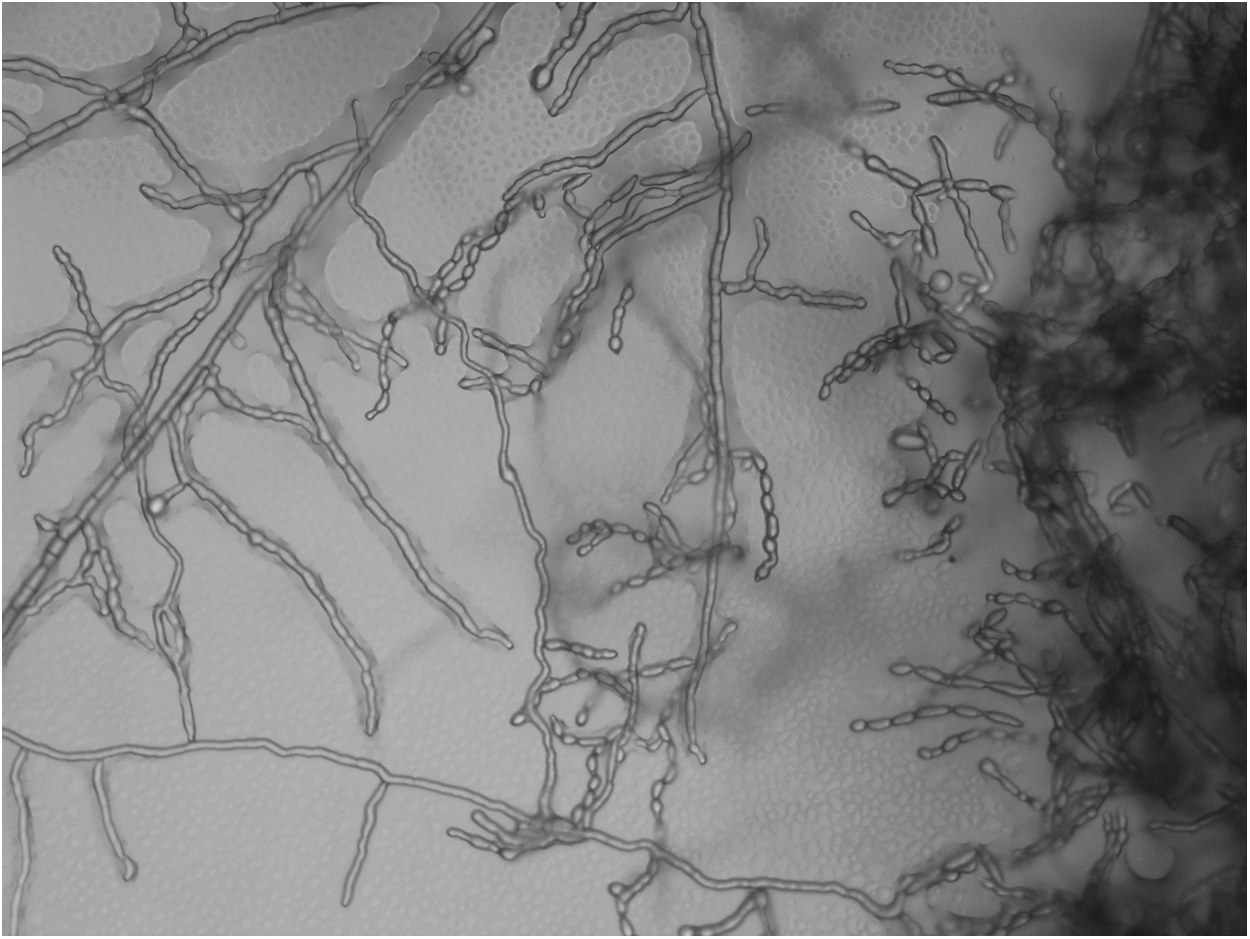
Cladophialophora bantiana—the native preparation, magnification 10×20.
Despite the established treatment, the abscess lesions progressed in both the lungs and the brain. Therefore, the antifungal therapy was changed after two months and combination therapy with amphotericin B (four weeks conventional followed by liposomal amphotericin B) and posaconazole was administered for the next two months. The patient's condition necessitated additional stereotactic puncture of the brain abscesses. Subsequent CT scans of the lungs demonstrated marked regression of the lung lesions and regression of lymphadenopathy. A MRI scan of the brain revealed regression of the lesion on the left side parietally and unchanged findings of other focal lesions in the brain. The liver graft function was good despite minimal immunosuppression and the antifungal therapy mentioned previously. After another month, the patient experienced a paroxysmal seizure with worsening of the right-sided hemiparesis, and progression of the abscess lesions in the brain was proved. Therefore, the third stereotactic puncture was performed with subsequent drainage of the brain abscesses and re-introduction of the combination antifungal therapy with amphotericin B and posaconazole. However, the patient's condition was complicated by fungal sepsis, of which the patient died 21 mo after the liver transplantation and eight months after the start of treatment of fungal infections. Autopsy confirmed progression of the fungal infection in the lungs and brain.
Treatment of brain abscesses caused by Cladophialophora bantiana includes surgical intervention and combination antifungal therapy. Levin et al. described a case of combination treatment with liposomal amphotericin B, voriconazole, and flucytosine with a fatal outcome after 45 d. In their article, they documented eight cases of brain abscess after organ transplantation since the year 1966: The cases involved two heart transplant recipients, four kidney transplant recipients, one liver transplant recipient, and one combined heart and lung transplant recipient. The mean age was 41 years, time from transplantation was from nine to 120 mo. In five cases, the therapy included a neurosurgical procedure. All but one patient were treated with amphotericin B, and three patients had combination treatment with itraconazole or voriconazole with flucytosine. The mortality rate was 71% [1]. Unfortunately, there are no tests to determine the risk of infection after organ transplantation. The risk of infection after organ transplantation changes over time, especially with the adjustment of immunosuppression. It is always necessary to assess the risk of infection and also the risk of rejection of the organ transplant [2]. Long-term prophylaxis is used to reduce the risk of serious complications, especially in the first half of the year after the transplant surgery. In our facility, we administer rifaximin in combination with a single oral ketoconazole dose for pre-operative prophylaxis to decolonize the intestine. For long-term prophylaxis, we administer cotrimoxazole per os and local co-trimoxazole in the oral cavity between meals for three months. A total of 459 transplants were carried out at the transplant center in Brno between February 2, 1983, and March 31, 2013. The authors found only one case of Cladophialophora bantiana in these patients.