
Abstract
Abstract
Background:
Deep sternal incisional surgical site infection is a serious and potentially life-threatening complication after open heart surgery. Although a rare post-operative complication, the rates of post-operative morbidity and mortality are greater in patients who develop a deep sternal incisional surgical site infection than in those who do not.
Methods:
We evaluated retrospectively the results of patients who developed a deep sternal incisional surgical site infection who were treated with either a pectoralis major flap or delayed primary closure after previous negative-pressure wound therapy (NWPT). From July 2007 to July 2012, 25 patients had a deep sternal incisional surgical site infection after open heart surgery in the Departments of Plastic Surgery and Cardiac Surgery of the Tri-Service General Hospital Medical Center. Sternal refixation was not performed in our patients.
Results:
In 15 patients, a unilateral or bilateral pectoralis major advancement flap with a myocutaneous or muscle flap was used. In seven patients, delayed primary closure was performed after NPWT. One patient received a rectus abdominis myocutaneous flap and another received a free anterior lateral thigh flap. One patient died after developing nosocomial pneumonia with severe sepsis after debridement.
Conclusions:
In our series, no patient required sternal re-fixation. Our findings suggest that delayed primary closure and use of a unilateral or bilateral pectoralis major flap following NPWT for a deep sternal incisional surgical site infection are simple and quick methods for managing such difficult surgical incisions even if the deep sternal surgical site infection is located in the lower one-third of the sternum.
S
Debridement and negative-pressure wound therapy (NPWT) are the first therapeutic choices of the cardiothoracic surgeon [4]. Various flaps can be used to close the wound; these include a pectoralis major (PM) muscle pedicled flap, rectus abdominis (RAM) flap, and latissimus dorsi flap. Alternatively, transposition of the greater omentum, with or without split-skin grafting [5], can be used. However, there is no consensus about the use of these different reconstruction techniques for individual patients who may have diverse clinical conditions. In addition, it is easier to treat a infection in the upper two-thirds of the sternum with a PM muscle flap than it is to treat a infection in the lower one-third of the sternum [6]. The purpose this study was to describe our practices for treating deep sternal surgical site infections.
Patients and Methods
We analyzed retrospectively the data for 25 patients who were treated at the Tri-Service General Hospital Medical Center in Taiwan between July 2007 and July 2012. The sternal surgical site infections were classified as infection type IVA or IVB using the El Oakley classification [7]; type IVA was defined as an infection presenting within 6 wks after the operation after one failed therapeutic trial, and type IVB was defined as an infection presenting within 6 wks after the operation after more than one failed therapeutic trial. The inclusion criteria were having a bacterial surgical site infection, having received NPWT, and having received treatment with a secondary flap closure of the sternal surgical site at our hospital.
The surgical site infections were debrided with resection of bony sequesters. After adequate debridement, we covered the site with polyurethane foam dressing and applied intermittent NPWT (Vacuum-assisted closure therapy®, KCI, San Antonio, TX); the negative pressure was limited to 125 mm Hg. Antibiotics were used individually according to the susceptibility of the bacteria identified.
No sternal refixation was performed in these patients. After achieving control of the infection and the well-vascularized incision base was found, we created the flap according to the site of the incision—upper two-thirds or lower one-third of the sternal surgical site. Fifteen patients received coverage with a unilateral or bilateral PM flap with a myocutaneous or muscle flap (Figs. 1 and 2). Seven patients received a delayed primary closure; one patient received a free anterior lateral thigh flap and one patient received an RAM flap.
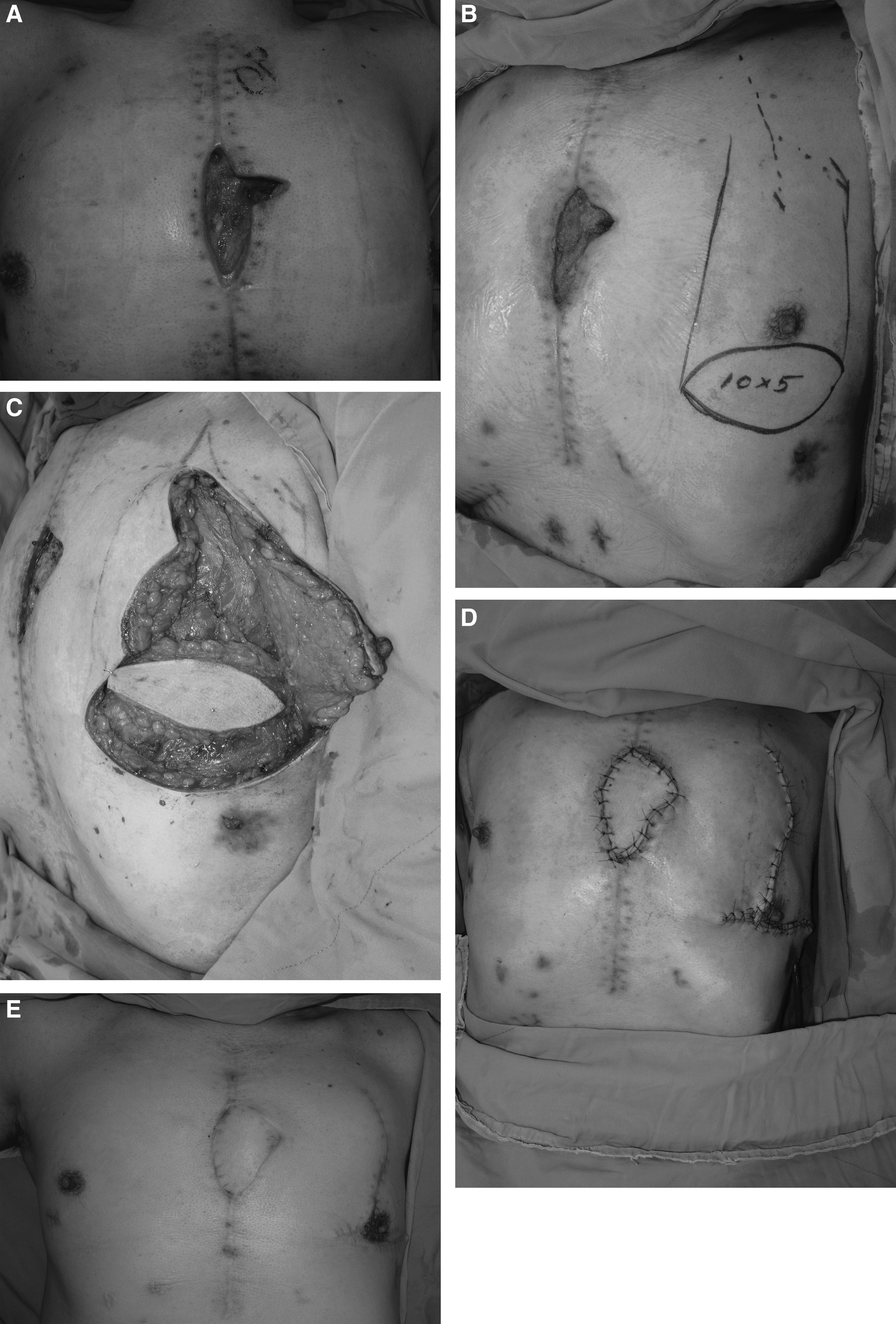
Sample of the sternal defect and coverage with a unilateral pectoralis major (PM) myocutaneous flap.
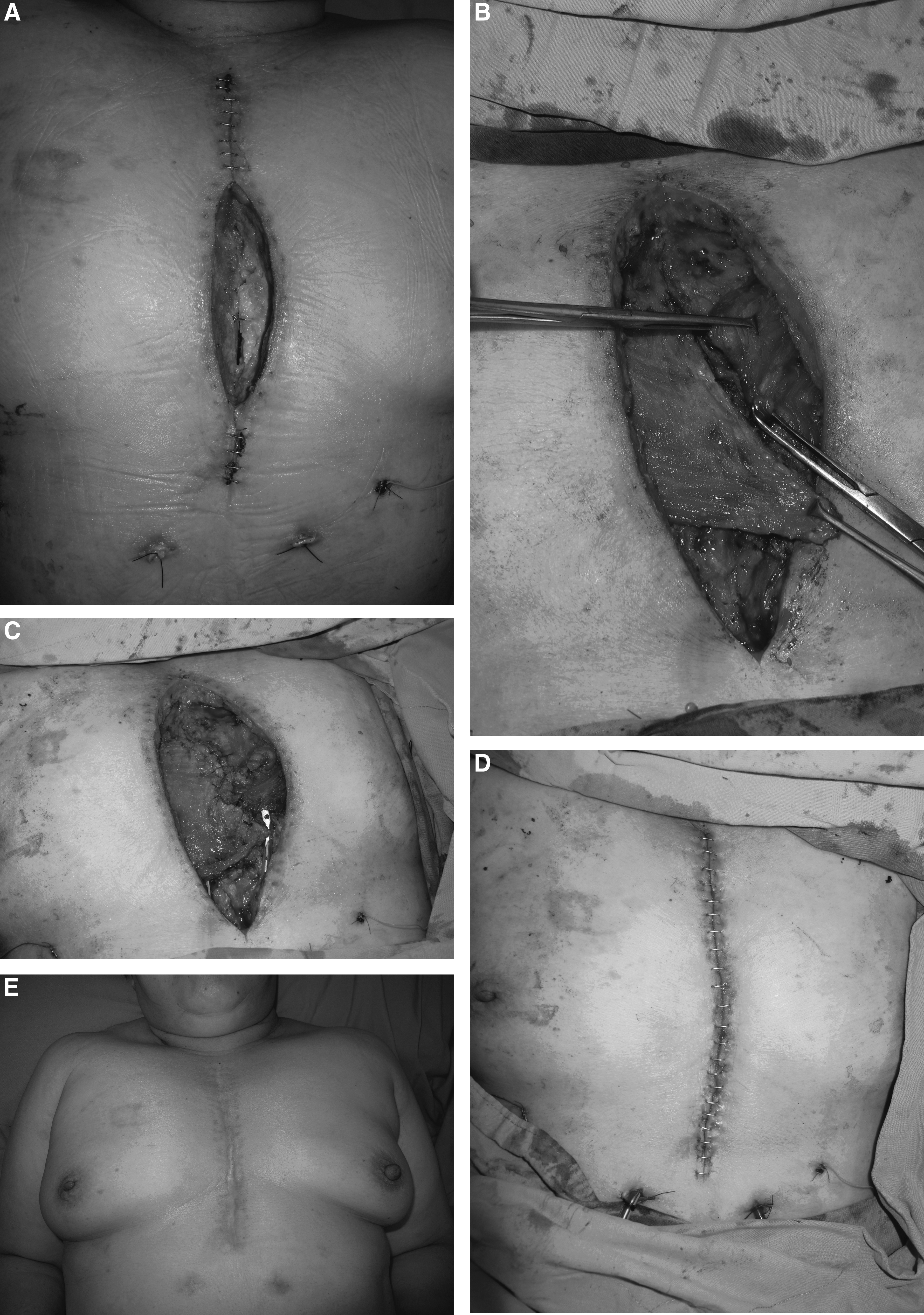
Sample of the sternal defect and coverage with a bilateral pectoralis major (PM) muscle flap.
Results
Twenty-five patients were included in this study: 20 males and 5 females, whose mean age was 66.5 y at the time of flap closure (Table 1). The patients had developed deep sternal surgical site infection after a procedure such as open heart surgery for coronary artery bypass graft, valve replacement, heart transplantation, or reconstruction of the aorta. Negative pressure wound therapy was used in all patients before closure of the sternal incision; the average duration of treatment was 18.7 days.
BMI=body mass index; NWPT=negative-pressure wound therapy.
Antibiotics were vancomycin empirically and then according to the susceptibilities of bacteria detected in the incision for each patient and average duration of antibiotics was 41 d. The pathogen detected most frequently in this study (68% of patients) was methicillin-resistant Staphylococcus aureus (MRSA; Table 2), which was treated with vancomycin. The other pathogen was Pseudomonas aeruginosa, which was treated with ceftazidime and the average duration of antimicrobial treatment was 48 d.
No patient received sternal re-fixation and all received 3–5 debridements before closure of the incision. If granulation tissue formation after NPWT and incisions were free of microorganisms, we would perform the reconstruction with flap or delayed primary closure. Fifteen patients received PM flap coverage, and two patients developed the complication of wound dehiscence but no flap loss. Two of the seven patients with delayed primary closure also had incision dehiscence. There were four patients with incision dehiscence and incisions were all free of microorganisms. One of these patients received free anterior lateral thigh flap coverage and had the complication of partial necrosis due to infection. The other patient received an RAM flap and had no complications. One patient died from nosocomial pneumonia complicated by sepsis after one debridement of the sternal incision. The sternal incision healing time for all patients was 50 to 105 days.
Discussion
Deep sternal incisional surgical site infection is a potentially life-threatening complication after sternotomy for cardiac surgery and can cause instability of the chest, chronic osteomyelitis, and incision dehiscence [7]. Therefore, the initial treatment is crucial, and sternal refixation for incision closure after Negative pressure wound therapy has been recommended by Daya and Barnes [8]. NPWT can reduce bacterial colonization and increase dermal perfusion and granulation tissue formation [9–11], and is the first treatment considered for deep sternal incisional surgical site infection, mortality and reinfection rates and a hospital stay are favorable compared with conventional treatment [12]. In our study, no patient required sternal refixation and all were treated with NPWT and antibiotics. The initial treatment in our patients included early adequate debridement, NPWT, and broad-spectrum antibiotics for MRSA before closure of the sternum.
Methicillin-resistant S. aureus was associated with a high risk for incision dehiscence in other studies [13,14]. Gram-negative bacteria also cause incision dehiscence but are found rarely, and surgical site infections by these microorganisms may be caused by skin contamination, transfer into the bone via intravenous drug use, or contamination [13,15]. In our series, MRSA was the pathogen frequently found most in our patients (68%), followed by P. aeruginosa, which was found in 12% of patients. In the initial treatment in our hospital, we consider empiric use of antibiotics, such as vancomycin and ceftazidime, for these pathogens.
After adequate debridement including removal of all infected, devitalized tissue, and obliteration of dead space [16], the surgeon may choose from several reconstruction methods including the PM muscle pedicled flap, RAM flap, latissimus dorsi flap, or greater omental flap [17]. The PM flap is a dependable pedicled flap the advantages of which include the ease of harvest and overall reliability in terms of flap survival [18]. Because of its anatomic proximity, the PM muscle pedicled flap is the first choice for reconstruction of a deep sternal surgical site infection [19], but the flap is not suitable for patients who have received previous axillary radiation therapy or have low muscle density [20]. It is easier to repair an incision in the upper two-thirds of the sternum with the PM muscle or other flaps than an incision in the lower one-third of the sternum [6]. In our patients, a simple flow chart showing our principles for treating deep sternal incisional surgical site infections is given in Figure 3. After adequate debridement and NPWT, we close the sternal incision a primarily and with a PM muscle pedicled flap because it is a quick and simple method to manage a patient with complications such as a deep sternal incisional surgical site infection. In five patients, we used a PM muscle pedicled flap to close the incision in the lower one-third of the sternum, possibly because of granulation tissue formation after NPWT. One of the patients with a incision in the lower one-third received a free anterior lateral thigh flap but developed partial necrosis. We note that this flap is used rarely in the reconstruction of sternal incisions because of the long operation time and poor general condition of these patients [6], suggesting that this flap may be not suitable for such patients. The other patient with an incision in the lower one-third of the sternum was treated with an RAM flap for coverage; this type of flap is another option for reconstruction of incisions in the lower one-third of the sternum.
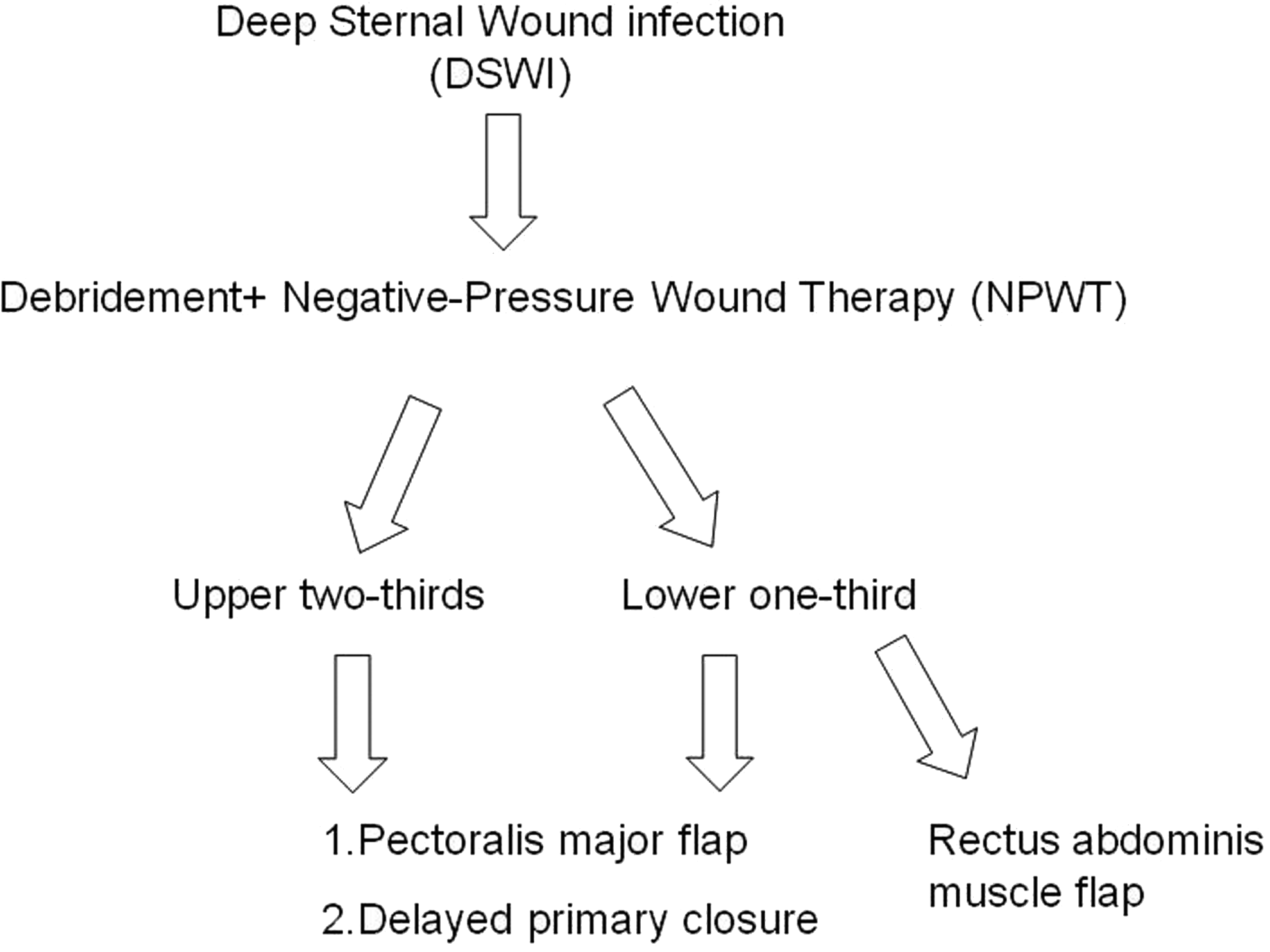
Flow chart: A simple protocol for reconstruction of deep sternal surgical site infection.
Conclusions
In our experience, when treating patients who develop a deep sternal surgical site infection after open heart surgery, our initial principle is to provide immediate adequate debridement, NPWT, and broad-spectrum antibiotics for coverage of possible pathogens. Our preference is for no sternal refixation and a simple method to close these incisions using a PM flap or RAM flap for incisions in the lower one-third of the sternum. Even a primary closure after NPWT may be a good choice for reconstructing a difficult surgical site infection in this type of critical patient.
Footnotes
Author Disclosure Statement
No competing financial interests exist.