
Abstract
Abstract
Background:
Current studies of post-operative Staphylococcus aureus disease focus primarily on surgical site infections and are often limited to infections caused by methicillin-resistant Staphylococcus aureus (MRSA). The objective of this retrospective cohort analysis was to describe the occurrence of and outcomes associated with post-operative MRSA and methicillin-sensitive S. aureus (MSSA) infections in patients undergoing elective surgical procedures.
Methods:
Data were extracted from Health Facts for inpatients aged 18 years or older with pre-defined International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure codes, meeting additional criteria indicating that the procedure was elective. Post-operative S. aureus infection was identified by one or more qualifying culture positive for MRSA or MSSA. Multivariable regression models compared patients with MRSA, MSSA, and no S. aureus infection.
Results:
Among 34,866 qualifying patients, the incidence of S. aureus infections was 0.9% during the index admission and 1.7% within 90 d after elective surgery, of which 36.6% and 38.4% were MRSA, respectively. The highest rates were observed among patients undergoing general surgery (2.2% during index admission, 3.2% within 90 d) and plastic surgery (1.8% during index admission, 3.1% within 90 d). Patients with MRSA and MSSA experienced poorer outcomes than uninfected patients, based on index admission length of stay (LOS; mean, 30.2, 22.7, and 5.7 d, respectively), hospital charges ($165,651, $134,313, and $52,077), and hospital mortality (odds ratios, 6.4 for MRSA, 4.8 for MSSA versus uninfected patients). Relative to MSSA infection, MRSA infection was associated with greater total hospital LOS and hospital charges but not with increased re-admission or mortality.
Conclusions:
The burden of post-operative S. aureus infection is shared among elective surgical procedures, however, rates and types of infections vary. Whereas MRSA infection results in substantially greater health care cost and LOS, mortality and re-admission rates are similar among patients with MRSA and MSSA. In elective surgery, infection control and surveillance for both MRSA and MSSA are warranted.
S
This study aimed to describe the characteristics of post-operative S. aureus infections after elective surgical procedures and to examine the impact on clinical outcomes and health care resource utilization associated with MRSA and MSSA infections by comparison with surgical patients without S. aureus infections. Our scope extended to a range of elective procedures and considered infections in multiple anatomic sites.
Patients and Methods
Study design and data source
This retrospective cohort study used the Health Facts electronic health record (EHR) database (Cerner Corporation, Kansas City, MO). As an EHR database, it consists of data collected during the course of usual clinical practice from U.S.-based hospitals and contains a comprehensive clinical record for each encounter, including pharmacy, clinical and microbiology laboratory, admission, and billing information from affiliated patient care locations. Data used for the study were Health Insurance Portability and Accountability Act compliant.
Population selection
Included patients were hospitalized between April 2005 and March 2010 and were 18 years of age or older. Patients were required to have at least one qualifying surgical procedure as identified by International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure codes. Each procedure was assigned to one of seven surgical subgroups: Cardiothoracic, general, gynecologic/genitourinary (GYN/GU), neurologic, orthopedic, plastic, or vascular. Procedures were classified as major (e.g., entering a body cavity, organ, or joint space via an open procedure) or minor (e.g., laparoscopic or minimally invasive). Procedures involving permanent implantation of a device were flagged. Patients with multiple procedures in different surgical subgroups were categorized by the procedure that occurred first or by that which was assigned as primary. A small number of patients were assigned manually to a surgical subgroup; two physicians reviewed these cases independently.
To ensure that only elective procedures were selected for analysis, we required that the primary procedure be performed within two days of admission. Patients with urgent or emergent admission status, transferred from the emergency department or another acute care facility, or with a discharge diagnosis consistent with surgical emergency or trauma were excluded. Patients could not have evidence of pre-existing or peri-operative S. aureus infection by positive culture or ICD-9-CM discharge diagnosis codes. For patients with multiple eligible encounters in Health Facts, only the first encounter was considered.
Post-operative S. aureus infection identification
Post-operative S. aureus infection was identified by one or more qualifying cultures, defined by site and source descriptions in the microbiology record. Site/source descriptions determined to carry a high risk of contamination or colonization (e.g., superficial swab, ulcer) were excluded. Infection types (i.e., blood, urine, respiratory, neurologic, orthopedic, other) were assigned based on the site/source information associated with the microbiologic specimen. “Other” infection types comprised site/source descriptions indicative of clinically significant infection (e.g., body fluid, tissue, abscess) that could not be categorized definitively based on anatomic site or organ system. Notably, SSIs were included in this category. Orthopedic infections comprised infections of bone and joint but may have included some SSIs. If methicillin resistance was reported in association with a qualifying culture, the infection was categorized as a MRSA infection; otherwise, infection was assumed to be MSSA. Patients with qualifying cultures positive for both MRSA and MSSA were assigned to the MRSA group.
Data elements and outcome measures
The characteristics of post-operative S. aureus infections were described by incidence, anatomic site, and timing. Incidence was calculated as percent of patients with a positive S. aureus culture; MRSA rate was defined as percent of S. aureus infections reported as methicillin resistant. These measures were assessed during the index admission, and within 30 and 90 post-operative days. Time to infection was defined as the number of days elapsed between the day of operation and the day of the first (index) S. aureus-positive culture. To assess time at risk of infection in patients without S. aureus infection, a pseudo-index culture was defined as the patient's last S. aureus-negative culture. Patients receiving an anti-S. aureus antibiotic between post-operative day three and discharge were flagged.
Impacts associated with post-operative S. aureus infections were assessed based on: (1) length of inpatient stay; (2) time from index/pseudo-index culture to discharge; (3) total hospital charge; (4) in-hospital mortality; (5) proportion of patients alive at discharge who went to skilled nursing facilities (SNF) or nursing homes; (6) all-cause re-admission within 30 and 90 post-operative days; (7) re-admission likely associated with S. aureus infection (i.e., re-admission during which a positive S. aureus culture was reported) within 30 and 90 post-operative days. Comparisons were made between patients with MRSA or MSSA infection and patients without S. aureus infection, and between patients with MRSA and MSSA infection.
Patient comorbidities of interest were derived from ICD-9-CM discharge diagnoses of encounters within the previous 12 mo, including the current encounter. Total hospital charges were reported by contributing institutions; approximately 70% of patients had charge data available. Charges were adjusted to 2009 U.S. dollars using the Consumer Price Index (Medical Care Services Factor).
Statistical analysis
Patient and encounter characteristics were compared among cohorts (MRSA/MSSA/no S. aureus) using χ2 tests for categorical variables and Wilcoxon two-sample rank-sum tests for continuous variables. For outcomes, the general linear model procedure was used to compare LOS, days from index/pseudo-index culture to discharge, and total hospital charges. A gamma distribution was assumed for hospital charges with a log link. Logistic regression was used for the outcomes of discharge to SNF/nursing home, mortality, and re-admission. The models compared among patients with MRSA, MSSA, and no S. aureus, while controlling for multiple variables as listed in Table 1. Variables were selected based on the medical literature and available data elements, considering their potential to impact both the outcomes we examined and the risk of S. aureus infection [13,16–18]. All variables were tested for association with S. aureus infection status. Only the variable describing the nature of the procedure as “major versus minor/minimally invasive” was not significantly different across the S. aureus infection cohorts. However, it was significant in most of the adjusted models, indicating its usefulness in explaining outcomes.
GYN/GU=gynecologic/genitourinary; MRSA=methicillin-resistant Staphylococcus aureus; MSSA=methicillin-sensitive S. aureus; SD=standard deviation; SNF=skilled nursing facility.
Longer LOS can be both a risk factor for and a result of hospital-acquired infection (HAI); thus, we aimed to compare patients with equivalent time at risk. We performed a sensitivity analysis using strata defined by (1) number of days from operation to index/pseudo-index culture and (2) propensity for S. aureus infection. Propensity scores were generated for each patient using a logistic regression model with S. aureus infection as the dependent variable, controlling for the variables included in the outcomes analysis. Missing days to pseudo-index culture was imputed by random sampling with replacement from the distribution of non-missing days to pseudo-index culture values among patients without S. aureus infection with the same or shorter LOS. Only patients with four or more days to index/pseudo-index culture were included in the sensitivity analysis; they were classified into eight strata based on two categories: (4–5, 6+ d) of days to index/pseudo-index culture, and four quartiles of propensity for S. aureus infection. All analyses were performed using Statistical Analysis System (SAS) software version 9.22 (SAS Institute Inc., Cary, NC).
Results
S. aureus infection by surgical subgroup
A total of 34,866 patients with a qualifying elective surgical procedure were identified from among 80 geographically dispersed U.S. hospitals. Characteristics of S. aureus infection in the study population are presented by surgical subgroup in Table 2. The most common surgical category was orthopedic (n=11,786, 33.8%). General (n=6,928, 19.9%), cardiothoracic (n=6,208, 17.8%), and GYN/GU (n=5,441, 15.6%) operations comprised most of the remaining patients, with neurologic, vascular, and plastic procedures being less common.
Includes 1 patient with S. aureus infection who stayed in hospital longer than 30 post-operative days during the index admission; therefore, S. aureus infection rate was higher than rate within 30 post-operative days.
Not mutually exclusive because positive S. aureus culture could occur in multiple sites.
Denominator=all patients in surgical subgroup.
Denominator=all patients with S. aureus-positive culture during index admission.
Denominator=all patients with S. aureus-positive culture within 90 post-operative days.
GYN/GU=gynecologic/genitourinary; MRSA=methicillin-resistant S. aureus; MSSA=methicillin-sensitive S. aureus; SD=standard deviation.
The overall incidence of post-operative S. aureus infection was 0.9% during the index admission, 1.1% at 30 d, and 1.7% at 90 d after the index procedure. Infection rate varied by surgical subgroup, with highest rates reported among general surgery (2.2%, 2.3%, and 3.2%, respectively) and plastic surgery (1.8%, 1.6%, and 3.1% respectively) patients and lowest rates among GYN/GU patients (0.3%, 0.4%, and 0.6%, respectively). Among all patients, lung was the most common infection site (0.8% at 90 d), followed by blood (0.3%) and other sites (0.5%). At 90 d after index procedures, the proportions of S. aureus infections caused by MRSA varied by surgical subgroup from 29.4% among plastic surgery patients to 51.4% among GYN/GU surgery patients. First S. aureus-positive culture occurred on average at post-operative day 26; two-thirds of infections occurred within 30 post-operative days. More than 40% of S. aureus infections occurred after discharge, although this fraction was much greater among orthopedic (77.7%) and neurosurgical (63.4%) subgroups.
Analysis of rates of S. aureus-positive cultures by year revealed that the proportion of patients in our study with S. aureus-positive cultures during the index admission peaked in 2007 and declined after that (Fig. 1; p value for linear trend, 0.0146). A similar trend was observed for MRSA (p=0.0023). In contrast, the decline after 2007 was less pronounced for MSSA, with no significant linear trend.
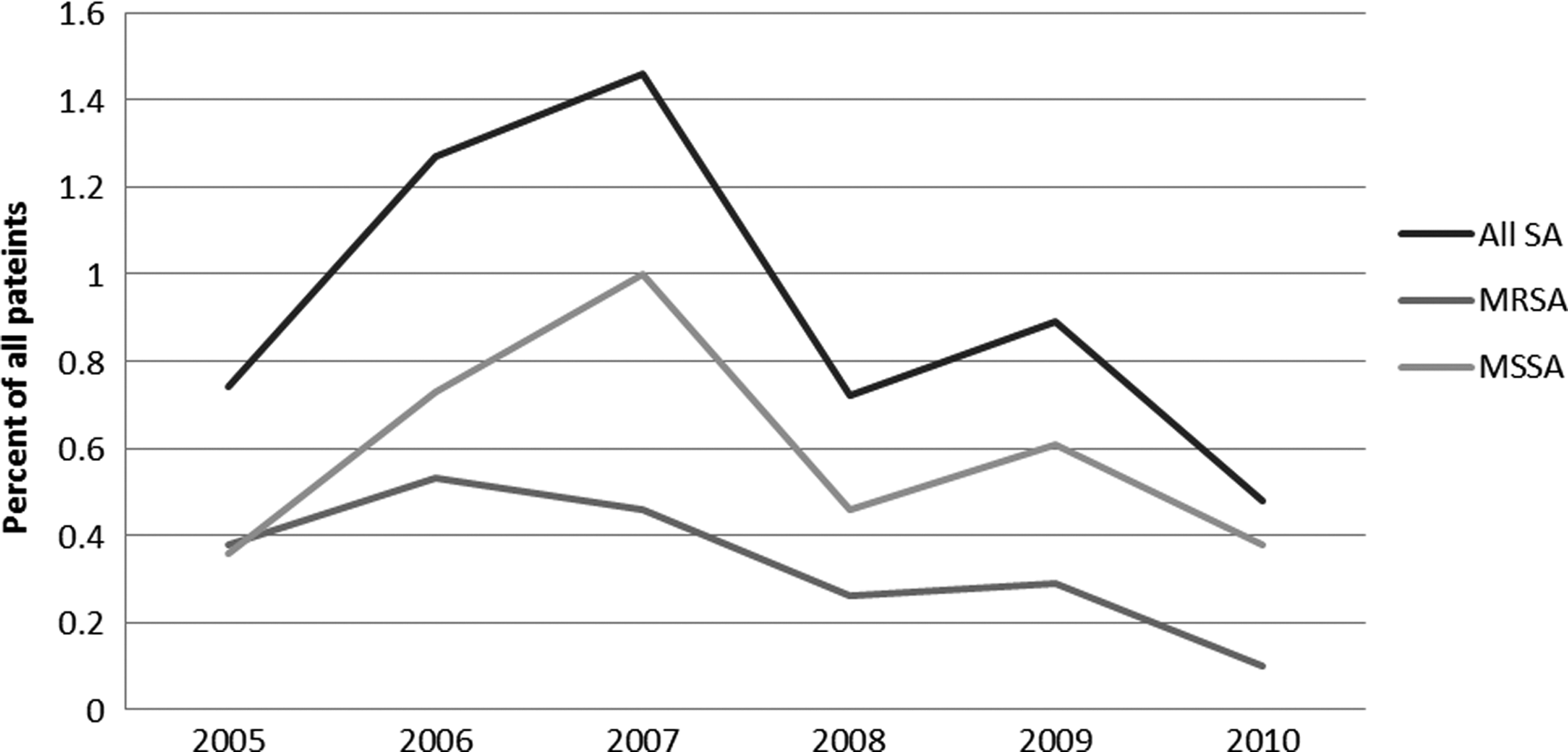
Percent of patients with Staphylococcus aureus (SA) by year. MRSA=methicillin-resistant S. aureus; MSSA=methicillin-sensitive S. aureus.
Patient and clinical characteristics
Differences in demographic and encounter characteristics were evident between infected and uninfected patients (Table 1). Patients with either MRSA or MSSA were significantly older than those without S. aureus infection. Infected patients were more likely to have undergone general or cardiothoracic procedures, while those without infection were more likely to have undergone orthopedic and GYN/GU procedures. Ninety percent of procedures were classified as major, with no significant difference between S. aureus and uninfected cohorts. Patients with MRSA and MSSA had more chronic comorbidities than those without infection, as evidenced by a greater likelihood of having a Charlson Comorbidity Index score ≥2, and by significantly greater rates of cardiac disease, chronic kidney disease, cancer, and chronic respiratory disease but not diabetes mellitus. Nearly three-quarters of patients with S. aureus during the index admission received an anti-staphylococcal antibiotic, versus 27% of patients without S. aureus.
In the sensitivity analysis, cohorts (stratified by time from surgery to index/pseudo-index culture and propensity for S. aureus infection) comprised 270 patients with infection (102 MRSA, 168 MSSA) and 10,493 patients without S. aureus infection. There were fewer statistically significant differences between the S. aureus and uninfected groups (Table 1). Patients with S. aureus were still more likely to be in the general surgery subgroup and less likely either to be in the orthopedic subgroup or to have had a permanently implanted device. The significantly greater rate of cardiovascular disease persisted among MSSA versus comparators, as did the greater occurrence of diabetes mellitus in non-S. aureus versus MSSA patients.
Clinical outcomes and resource utilization
Post-operative MRSA and MSSA infection were each associated with poorer clinical outcomes and increased resource utilization, after adjustment for demographic characteristics, chronic comorbid conditions, surgical aspects, and hospital factors (Table 3). Odds of in-hospital mortality at index admission and within 90 post-operative days were significantly greater for both MRSA (odds ratio [OR] 6.4 and 5.7, respectively, p<0.0001 for both) and MSSA (OR 4.8 and 4.5, respectively, p<0.0001 for both). Discharge to a SNF or nursing home, among survivors, was three to six times more likely among patients with S. aureus infection. Patients with MRSA and MSSA each had greater odds of all-cause re-admission within 30 and 90 post-operative days (among survivors). Methicillin-sensistive S. aureus was associated with significantly greater re-admission relative to absence of S. aureus infection. Total LOS was four to five times longer among the patients with S. aureus infection. Length of stay after index/pseudo-index culture was also substantially (11–17 d) longer. Total hospital charges at index admission and within 90 post-operative days were greater for patients with MRSA and MSSA (all p<0.0001). Compared with patients with MSSA, both LOS and charges for the index admission were significantly greater for patients with MRSA but no other differences were observed.
p<0.0001, bp<0.01, cp<0.05 adjusted for age group; gender; race; insurance type; Charlson Comorbidity Index; the presence of chronic cardiac disease, kidney disease, cancer, respiratory disease, liver disease, and diabetes; procedure year; surgery subgroup; major procedure; procedure with a permanent device; time to index/pseudo-index culture; and hospital indicators for region, teaching hospital, and number of beds.
MRSA vs. no S. aureus.
MSSA vs. no S. aureus.
MRSA vs. MSSA.
Positive S. aureus culture occurred during the re-admission.
LOS=length of stay; MRSA=methicillin-resistant S. aureus; MSSA=methicillin-sensitive S. aureus; SD=standard deviation; SNF=skilled nursing facility.
The sensitivity analysis was intended to adjust for time at risk for infection (time to index/pseudo-index culture). Differences in outcomes persisted when comparing the MRSA and MSSA cohorts with uninfected patients. The effect of S. aureus infection on hospital mortality and likelihood of discharge to a SNF/nursing home was somewhat attenuated but remained statistically significant. The impact on total hospital LOS was consistent with the primary analysis: LOS was increased by 2 wks for patients with either MRSA or MSSA (p<0.0001 for both). Total hospital charges were again significantly greater among patients with either MRSA or MSSA. All-cause and S. aureus-associated re-admission rates among survivors were similar to those of the main analysis. All outcomes were similar between MRSA and MSSA patients.
Discussion
To our knowledge, this is the first study to evaluate MRSA and MSSA infection incidence, clinical outcomes, and resource utilization across the spectrum of elective surgical procedures. Much of the existing literature focuses on SSI, whereas we considered a range of post-operative S. aureus infections based on anatomic site. Whereas there are few studies specific to elective surgery with which to relate our findings directly, our estimates are comparable to the work of Anderson et al. [16] (overall incidence, 0.47%; comprising SSI, 0.33%; and blood stream infection, 0.19%). The median time to infection in our analysis was 18 post-operative days, which is also similar to the work of Anderson et al. [16] (20 d). In our study, 38% of infections contracted by post-operative day 90 were caused by MRSA, versus 51% as reported by Anderson et al. [16]. Differences in S. aureus infection rates by surgical subgroup were evident: General and plastic surgery procedures accounted for the highest rates of infection, whereas the study by Anderson et al. [16] reported more infections among neurosurgical patients (0.62%) and fewer in plastic surgery (0.32%). Comparisons across studies should be made cautiously, given the heterogeneity in qualifying procedures, definition and time frame of infections, and participating hospitals.
In an elective (versus urgent/emergent) procedure, providers have more opportunity to take preventive measures to minimize the risk and reduce the burden of post-operative S. aureus infection. However, the present results demonstrate that the toll remains high. Our findings on outcomes associated with S. aureus infection among surgical patients extend those of previous work [12,13,19,20], although these studies are largely limited to evaluation of SSI. Among elderly patients, additional LOS of 12 post-operative days and charges of $41,117 have been attributed previously to deep or organ/space S. aureus SSI [12]. Deep incisional or organ/space SSI caused by MRSA was found to be an independent predictor of poor outcomes (re-admission, death, increased hospitalization, and hospital charges during 90 post-operative days) versus uninfected patients [13]. Our study adds to the growing body of literature on the clinical importance of MSSA as well as MRSA infections in a patient population not well documented previously. We demonstrated that MSSA is also associated with worse clinical outcomes and increased resource utilization. Moreover, post-operative MSSA and MRSA were similarly detrimental, with few differences in most of the outcomes we measured. In studies of surgical patients (limited to deep incisional or organ/space SSI), the incremental effect of methicillin resistance varied by outcome [5,13]. Engemann et al. [5] reported that resistance was associated independently with increased mortality and hospital charges but not hospital LOS [5]. In general patient populations, findings are mixed regarding the incremental burden of methicillin resistance [6,21–23]. Furthermore, the results of the trend analysis showing an attenuated decline in MSSA strengthen the case that MSSA remains a concern. Our data suggest that although infection control measures may be effective for MRSA, the impact on MSSA is less clear.
This large patient sample was identified from geographically diverse U.S. hospitals, thus, the results may be more generalizable than smaller, single-center studies. We leveraged multiple criteria available within the EHR to ensure capture of an elective surgical population, and used time-stamped culture data to exclude patients with pre-existing S. aureus infection. Our matching methodology was intended to create case and control groups with equivalent time at risk; patients without S. aureus infection were hospitalized for a similar length of time as those with infection, prior to first positive index culture. Including all patients and adjusting for demographics and comorbidities may not be sufficient. Patients without infection may likely have shorter LOS, potentially resulting in overestimation of the difference in LOS. Graves et al. [18] discuss these sources of bias in detail in their report on the effect of health care acquired on LOS and cost.
Our study has some limitations. The nature of the database and our inclusion/exclusion criteria selected against minor procedures, including percutaneous placement of devices. This bias may explain the observed lower rate of implanted devices among uninfected patients. Whereas we identified patients with cultures negative for S. aureus, we did not control for infections caused by other organisms. Some positive cultures may represent contamination or colonization rather than clinically significant infection, although we reviewed microbiologic site/source data to limit this risk. This distinction is more challenging in the context of respiratory cultures, which may in part account for the larger portion of infection sources attributed to lung. Tracheal colonization may occur in the intensive care unit, but this in itself has clinical implications [24]. Conversely, some excluded cultures may have represented clinically significant infection. Confounding factors may affect results in ways we cannot measure. The finding that diabetes mellitus was less common among infected versus uninfected patients was unexpected; there may be infection control practices (e.g., more aggressive antibiotic prophylaxis, bowel preparation) in the population with diabetes mellitus that could not be adjusted fully statistically.
Patients undergoing elective surgery are often discharged prior to onset of surgery-related health care acquired infections. Because data are not available for patients seen by a provider outside the Health Facts-contributing institution, infection rates up to 90 post-operative days may have been underestimated. Patients may have been included in the study if data representing pre-existing S. aureus infection were missing, which could result in an overestimation of post-operative infection rates. Infections occurring beyond 90 post-operative days were not included in this analysis.
Conclusions
Across the spectrum of elective surgical procedures, patients who contract post-operative S. aureus infection are at risk for increased mortality and hospital LOS, with greater resource utilization and health care cost. The risk of poor outcomes is not limited to MRSA; MSSA poses an equivalent hazard. Post-surgical surveillance and infection control measures should encompass MSSA as well as MRSA. The substantial percentage of S. aureus infections occurring after hospital discharge, particularly among orthopedic and neurosurgical cases, supports that infection control measures are appropriate throughout the continuum of care.
Footnotes
Acknowledgments
This study was supported by Pfizer, Inc. The authors gratefully acknowledge assistance from Jeffrey Binkley, PharmD, for project management support, Harlen D. Hays, MPH, for statistical input, and K. Suzanne Fiske, MS, and Jing Yi, MA, for data management.
Portions of this work were previously presented in abstract and poster form at: the 33rd Annual Meeting of the Surgical Infection Society, April 2013, Las Vegas, Nevada, IDWeek™, October 2012, San Diego, California, and the 52nd International Conference on Antimicrobial Agents and Infectious Diseases, September 2012, San Francisco, California.
Author Disclosure Statement
No competing financial interests exist.