
Abstract
Abstract
Background:
Catheter-associated urinary tract infection (CAUTI) and ventilator-associated pneumonia (VAP) are considered performance measures. We analyzed the incidence, prevalence, and risk of CAUTI and VAP in trauma patients, as well as the demographic and injury factors related to these infections and their relative risks of negative outcomes (prolonged length of stay [LOS], sepsis, and death).
Methods:
Trauma registry data were analyzed (age >18 y; LOS >24 h) from January 1, 2007, to December 31, 2011. Demographics and injury location, severity, and type were analyzed relative to outcomes along with device-associated infection, as defined by the U.S. Centers for Disease Control and Prevention. The outcomes analyzed were intensive care unit (ICU) and hospital LOS, sepsis, and in-hospital death. Multivariable logistic regression was then used to identify the factors contributing to sepsis, including device-associated infections.
Results:
The included population (n=10,755) was 66.6% male and had a mean age of 45.1 y, with blunt trauma in 91.8% and a median Injury Severity Score (ISS) of 10 points. Patients developing CAUTI (n=324; 3.0%; p<0.005) were more likely to be female (59.4%), had a higher median ISS (20.5), and were older (56.7 years). Patients with VAP (n=161; 1.5%; p<0.005) had a higher median ISS (27). Patients with sepsis (n=149; 1.4%; p<0.005) had a higher median ISS (24.0) and were older (52.3 y). Sepsis was associated with prolonged LOS and death, as expected (p<0.005). In multivariable analysis, independent predictors of sepsis were CAUTI (odds ratio [OR] 16.15; p<0.001), VAP (OR 6.95; p<0.001), ISS (OR 1.05 per unit; p<0.001), age (OR 1.02 per year; p<0.001), and penetrating, abdominal, pelvic, or chest injury.
Conclusion:
Development of CAUTI and VAP are significantly associated with a higher risk of sepsis in trauma patients after adjustment for age and injury type, location, and severity. This study suggests the importance of device-associated infections as vectors for sepsis in trauma and highlights the importance of prevention initiatives.
S
The risks and prevalence of CAUTI, VAP, and associated sepsis in trauma patients are not well known, nor is it known how risk factors for CAUTI, VAP, and sepsis combine to change the odds of a negative outcome (prolonged length of stay [LOS], sepsis, and death). This project analyzed the incidence, prevalence, and risk of CAUTI and VAP in trauma patients and the relative risk of negative outcomes to identify the factors contributing to the incidence of CAUTI, VAP, and sepsis and to determine whether device-associated infections are an independent risk factor for sepsis. We hypothesized that CAUTI and VAP have identifiable risk factors and increase the risk of prolonged LOS, sepsis, and death. We did not have sufficient cases (n<5) of central line-associated blood stream infection (CLABSI) to make a statistical analysis.
Patients and Methods
Inclusion criteria were admission to the University of Kentucky (LOS >24 h) between January 1, 2007 and December 31, 2011 with a diagnosis of blunt or penetrating trauma and age 18 y or greater. The U.S. Centers for Disease Control and Prevention (CDC) limits the definition of CAUTI to a UTI (diagnosed clinically or by culture) that occurs at least two d after the placement of an indwelling catheter or within 1 d after discontinuation of a catheter [8]. Similarly, pneumonia (diagnosed clinically or by culture) must occur at least 2 d after initiation of mechanical ventilation or within one d after discontinuation of mechanical ventilation [9]. The diagnoses of CAUTI and VAP must have been made during the hospital stay. The exclusion criteria were burns or age less than 18 y. At discharge, trauma nursing staff entered all patient data in the University of Kentucky Trauma Registry and determined whether infections noted in the charts met the CDC criteria for VAP or CAUTI [8,9]. Data were collected retrospectively from this registry. The Institutional Review Board approved the study protocol and found it exempt from full review on the basis of the low risk to the research subjects of using data from the Trauma Registry.
The patients were sorted into the following groups, which are not mutually exclusive: CAUTI (sepsis/no sepsis), VAP (sepsis/no sepsis), and no device-associated infection (sepsis/no sepsis). The patients' medical records were evaluated for the following data points: Demographics (age, gender), injury type (blunt or penetrating) Injury Severity Score (ISS), Abbreviated Injury Score (AIS), duration of device use, intensive care unit (ICU) and hospital LOS, and disposition (discharge to home or a rehabilitation center, or death). Each patient had a unique identifier once data were exported from the Research Electronic Data Capture (REDCap). This number, along with the study data, was collected and managed using REDCap tools hosted at the University of Kentucky. REDCap is a secure, Web-based application designed to support data capture for research studies, providing validated data entry, audit trails, data downloads, and data import from external sources [10].
The outcomes analyzed were ICU and hospital LOS, sepsis, and in-hospital death. We defined prolonged LOS as a stay in the top quartile (more than 8 d). We set the significance threshold at p<0.005 to allow multiple comparisons. Multivariable logistic regression was used to identify factors contributing to sepsis, including device-associated infections.
Results
The included population, defined in Table 1 (n=10,755), was 66.6% male, had a mean age of 45.1 y, was mostly blunt-injured (91.8%), and had a median ISS of 10 points. Overall, 3% had CAUTI, 1.5% had VAP, 1.4% had sepsis, 4.1% died, and 24.6% had an LOS >8 d (Table 2). The patients who developed CAUTI (n=324; 3.0%; p<0.005) were more likely to be female (59.4%) and older (56.7 y) and to have a higher overall median ISS (20.5 points). These patients had a higher (p<0.001) prevalence of VAP (13.9%), LOS >8 d (83.0%), sepsis (16%), and death (8.6%). The patients who developed a VAP (n=161; 1.5%; p<0.005) had a higher overall median ISS (27 points). These patients had a higher (p<0.001) prevalence of CAUTI (28.0%), LOS >8 d (100.0%), sepsis (14.9%), and death (5.6%).
Moderate=abbreviated injury score (AIS) 2.
Serious=AIS 3.
Severe plus=AIS ≥4.
p<0.005 for differences in groups with and without the outcome.
H, N, & F=head, neck, and face.
p<0.001 (Fisher exact test).
Patients who developed sepsis, regardless of etiology (n=149; 1.4%; p<0.005), had a higher median ISS (24.0 points) and were older (52.3 y). These factors were associated with a higher (p<0.001) prevalence of CAUTI (34.9%), VAP (16.1%), LOS >8 d (95.3%), and death (22.9%). Sepsis was associated with prolonged LOS and death, as expected (p<0.005). Patients with an LOS >8 d had a significantly higher (p<0.001) prevalence of CAUTI (10.2%), VAP (6.1%), and death (5.4%). Patients who died had a higher (p<0.001) prevalence of CAUTI (6.3%) and sepsis (7.6%).
By multivariable analysis, shown in Table 3 and Fig. 1, independent predictors of sepsis were CAUTI (odds ratios [OR] 16.15; p<0.001), VAP (OR 6.95; p<0.001), severe (AIS=3) and serious (AIS=4) abdominal injury (OR 2.60; p<0.001 and OR 3.00; p<0.001, respectively), penetrating injury (OR 2.54; p<0.005), severe chest injury (OR 2.00; p<0.05), serious pelvic/leg injury (OR 1.51; p<0.05), ISS (OR 1.05 per unit over 10 points; p<0.001), age (OR 1.02 per year over 45.1; p<0.001), CAUTI and VAP together (OR 0.10; p<0.001), and female gender (OR 0.51; p<0.001).
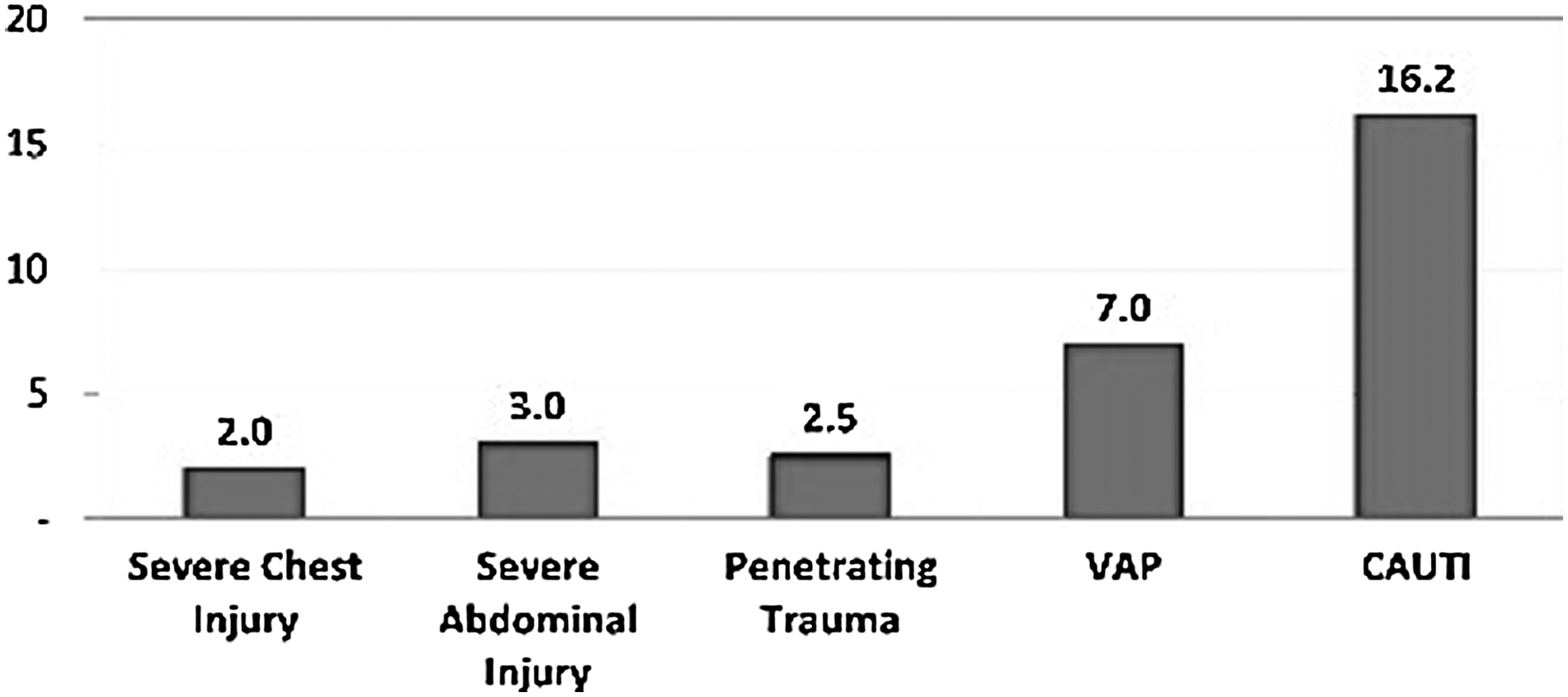
Odds ratios for risk factors for sepsis in patients with trauma adjusted for age, gender, and total Injury Severity Score. p<0.05 for all.
CAUTI=catheter-associated urinary tract infection; CI=confidence interval; ISS=Injury Severity Score; VAP=ventilator – associated pneumonia.
Discussion
The chances of a typical trauma patient developing a CAUTI or VAP are 3% and 1.5%, respectively. This confers a baseline 1.4% chance of developing sepsis and a 4.1% chance of death for the typical trauma patient. Factors that increase a person's chance of developing a CAUTI include being female, having a higher ISS, and being of greater age. Injuries with a strong associated risk for CAUTI are moderate head, neck, and face injury and abdominal injury. Traumatic brain injuries and spinal cord injuries have been reported to increase the odds of CAUTI [11]. A higher ISS (particularly with an abdominal injury) increases a person's risk of VAP. Pulmonary complications in trauma patients are reported to increase with advancing age, traumatic brain injury, and chest injury that requires a thoracic intervention such as thoracotomy, chest tube placement, or mechanical ventilation [12].
Some types of injuries appear to be associated with higher risks of sepsis, and these injury groups might therefore be targets of focused prevention efforts. Injuries with a strong associated risk for sepsis were severe chest injury (OR 2.0), severe abdominal injury (OR 3.0), and penetrating injury (OR 2.5). A higher ISS increases the odds of developing sepsis by 1.05 per point over 10 points. Certain injuries increase the odds of developing sepsis, such as serious pelvic/leg injury (1.51-fold), severe chest injury (2.00-fold), and abdominal injury (2.60-fold). Abdominal injury is linked to a higher risk of sepsis [13]. If the injury is penetrating, it increases the odds of sepsis 2.54-fold.
Both CAUTI and VAP are more potent than any other risk factor for sepsis. The presence of VAP increases the odds of sepsis 6.95-fold, and CAUTI increases the odds by 16.10. Increasing age over 45.1 y raises the odds of developing sepsis 1.02-fold per year. One study found that the odds of sepsis increase above 46 rather than 45 years of age [14]. Female gender reduces risk of sepsis in trauma victims by one-half. Published research on female gender and the risk of sepsis support this finding. The possibility of a protective effect of female hormones [15] vs. the harmful effect of male hormones [16] is being investigated.
Developing CAUTI and VAP together is not associated with a higher risk of sepsis above the baseline risks and may in fact be statistically protective. The reason for this paradox is unclear. A possible explanation is that having multiple antibiotics treating both infections is synergistic and thus more protective.
This study did not explore the timing and causal relations of events, merely associations. Thus, the exact causality of a device-associated infection and sepsis is unclear, and the sepsis may be from another source but coincident with device-associated infection. For instance, a patient who develops sepsis secondary to a penetrating chest injury may need to be ventilated mechanically and may subsequently develop VAP. However, the profound magnitudes of the odds ratios for CAUTI and VAP are not likely to be explained by this alone. Although it would be ideal to have culture data to draw conclusive connections between events, this was not feasible in this retrospective study. First, many CAUTI and VAP episodes were diagnosed clinically without positive cultures. However, the CDC does not require a positive culture for a diagnosis of CAUTI or VAP. Therefore, these cases were included in this study. Second, for those with a positive culture, the diversity of organisms reported makes it statistically difficult to draw any meaningful conclusions. Third, the majority of cases of sepsis were diagnosed clinically without documented bacteremia. Furthermore, even if different pathogens were identified as causing a device-associated infection and the episode of sepsis, it is possible that the treatment of the primary infection led to a super-infection [17,18].
Culture data in one study showed that pathogens causing VAP in trauma patients are more likely to be non-resistant strains of bacteria, leading to a lower mortality rate among trauma patients [19]. This may explain why VAP has a lower sepsis risk than CAUTI. The most common pathogens causing CAUTIs are Providencia stuartti and Proteus mirabilis [20] instead of the Escherichia coli commonly associated with community-acquired UTI [21]. Proteus mirabilis [22] and P. stuartti [23] are particularly virulent and may increase the mortality rate when associated with sepsis. More focused prospective research may confirm this hypothesis.
Conclusion
Device-associated infections increase the risk of sepsis and death after trauma. However, the incidence of device-associated infections is associated with greater injury severity and age. Thoracic injury, in particular, increases the risk of VAP, CAUTI, prolonged LOS, and sepsis. Once a patient has one device-associated infection, getting a second infection does not greatly increase the risk of sepsis. This study demonstrates the devastating effects of device-associated infections in trauma and highlights the importance of prevention initiatives, particularly given that key risk factors often are present on arrival and may not be modifiable.
Author Disclosure Statement
No competing financial interests exist.