
Abstract
Abstract
Background:
Surgical site infection (SSI) remains the most frequent complication after colorectal resection. The role of sutures coated with antimicrobial agents such as triclosan in reducing SSI is controversial.
Methods:
This was a multi-center randomized controlled trial with patients and outcome assessors blinded to treatment. The study was performed in four university referral hospitals. Patient candidates for elective colorectal resection were assigned randomly to abdominal incision closure with polyglactin 910 triclosan-coated sutures (triclosan group) or with polyglactin 910 without triclosan (control group). The primary outcome was the rate of SSI within 30 d after hospital discharge. The secondary outcomes were the overall rate of incision complications and length of hospital stay (LOS).
Results:
Two hundred eighty-one patients (triclosan group: 140; control group: 141) were analyzed after randomization. The rate of SSI was 12.9% (18/140) in the triclosan group versus 10.6% (15/141) in the control group (odds ratio: 1.24; 95% confidence interval: 0.60–2.57; p=0.564). Secondary outcome analysis showed an overall incision complication rate of 38.3% in the control group versus 45.7% in the triclosan group (odds ratio: 1.36; 95% confidence interval: 0.84–2.18; p=0.208). Median LOS was 11 d in both groups (p=0.55).
Conclusions:
Surgical sutures coated with triclosan do not appear to be effective in reducing the rate of SSI.
S
Patient-related risk factors and potential strategies to reduce the risk of development of SSIs are well known [2,6–9]. Among the innovative approaches to reduce the risk of incision infection is the ability to impregnate suture materials with anti-microbial substances. In fact, microbial adherence to the surface of sutures has been recognized as one of the reason for the development of incision infections [10–12]. To prevent microbial colonization of sutures, triclosan-coated materials have become available recently. Triclosan is an antiseptic that has been used in several pharmaceutical products over the past 30 years for its antiseptic properties and safety profile [13]. In vitro studies demonstrated that triclosan forms an inhibition zone around suture material and it is effective against the pathogens responsible most frequently for SSIs [14].
Clinical experience with this material is still limited. Two recent meta-analyses [15,16] on the effect of triclosan-impregnated sutures on SSI reported conflicting results. A potential limitation of both analyses was the heterogeneity of the studies incorporated ranging from clean to dirty operations and different types of surgery. Until now, only three randomized controlled trials (RCTs) addressing the effect of triclosan-coated sutures in colorectal operations have been published, with inconsistent outcome. A Hungarian multi-center trial [17] failed to demonstrate any advantage of impregnated sutures on the overall rate of SSIs. Two recent single-center studies [18,19] showed a significant reduction of incision infection in patients undergoing open colorectal resection treated with triclosan-coated sutures. We sought to evaluate the effect of a triclosan-coated sutures on the incidence of SSIs after elective colorectal operations.
Patients and Methods
Study design
The present study was a multi-center, randomized, controlled trial carried out in four university referral hospitals in Italy. The protocol was approved by the ethical committees of all four centers. Written informed consent was obtained from all participants before randomization. The study was registered at www.clinical-trial.gov with identifier number NCT01869257.
Study population
Patient enrollment took place between January 2010 and March 2013. Patients were eligible if they were candidates for elective colorectal resection with a clean-contaminated field. The exclusion criteria were younger than 18 y, pregnancy, emergency operations, ongoing infections, American Society of Anesthesiologists (ASA) score ≥3, any organ insufficiency, Karnofsky performance status <70, intra-operative evidence of gross contamination of the surgical field, and denied written consent. Necessity of re-operation for any reason during the post-operative course resulted in patient dropout from the trial with no replacement.
Random assignment and blinding
Patients were randomized during surgery after the colorectal resection was completed and just before beginning the closure of the abdominal wall. Treatment allocation was by means of a computerized randomization list with 1:1 ratio. Each center had an independent list. Assignment was done by sealed, opaque, numbered envelopes that were opened in sequence by a registered nurse not involved in the study.
This was an independent, unsponsored study and each hospital purchased the sutures. Therefore, it was impossible for the organizers of the trial to receive blind suture packages. As a result, operating surgeons were not blinded to the material used for incision closure. To minimize the risk of bias, patients and outcome assessors were blinded to the allocation for the full period of evaluation. The surgical staff members were not allowed to communicate information about treatment allocation to patients or other staff during the duration of the study.
Intervention
Patients were randomly allocated into two groups to receive either closure of the midline abdominal incision with triclosan-coated sutures (triclosan group) or a suture material without triclosan (control group). In the treated group the abdominal incision was sutured by a separate layer technique starting with the peritoneum with 0 Vicryl Plus® (triclosan-coated polyglactin 910; Ethicon Italia, Pratica di Mare, Italy), followed by the fascia with PDS Plus® (triclosan-coated polydioxanone; Ethicon), and then the skin with 3/0 Vicryl Plus®. The skin closure was by interrupted sutures, while the peritoneum and the fascia by a running suture. The identical technique was used in the control group using polyglactin (Vicryl®; Ethicon) or polydioxanone suture without triclosan (PDS II®; Ethicon). Suturing or not suturing the subcutaneous tissue layer was left to the preference of the operating surgeon. In cases of subcutaneous fat tissue closure, the technique was interrupted sutures with 3/0 Vicryl Plus or 3/0 Vicryl according to randomization. Bowel preparation with 3 L of an iso-osmotic solution was carried out only in patients who were candidates for rectal resection. Patients presenting with large bowel obstruction were treated with an endoscopic metallic stenting and operated on after a complete resumption of bowel function. Hair removal was performed the evening before operation or the morning of the operation with either an electric clipper or a razor blade. Skin disinfection before incision was done in all cases with a 10% povidone-iodine solution. Mechanical wound protectors were used only in case of laparoscopic resection during specimen extraction.
All patients received antibiotic prophylaxis. The type of drug was left to the preference of the operating surgeons but within the limited choice based on national guidelines [20]. A single pre-operative dose, 30 min before skin incision (single dose), or a pre-operative dose followed by three consecutive doses every 8 h after the operation (multiple doses) was based on surgeon prescription. A second dose of antibiotic during surgery was administered in cases in which the duration of the operation was longer than 4 h, intra-operative contamination, or bleeding more than 500 mL. Prevention of intra-operative hypothermia was carried out by means of warming blankets and infusion of heated fluids.
Data collection and follow-up
After the patients signed informed consent the following pre-operative baseline demographic characteristics and risk factors were recorded: Age, weight, height, body mass index [BMI], type of disease, ASA score, weight loss and its amount, smoking habit, diabetes mellitus, chemoradiation, steroid use, and laboratory parameters (blood glucose, albumin, pseudocholinesterase, lymphocyte count). During and after the operation the following data were recorded: Duration and type of surgery and technical details, use of peritoneal drainage, and blood transfusion.
Independent, blinded trained observers checked the patients during the post-operative course twice per day and the incision every other day until hospital discharge. The observers performed data collection using standard paper case report forms and electronic databases. Using the U.S. Centers for Disease Control and Prevention (CDC) criteria of 1999 [21], they recorded the occurrence of and defined SSI and any other incision event. Superficial incisional SSI and deep incisional SSI were considered in this trial whereas organ/space SSIs were not included because suture coating should not have a role in the occurrence of intra-peritoneal collection. Superficial incisional SSI was defined as an infection occurring within 30 d after the operation and involving only skin or subcutaneous tissue of the incision and at least one of the following: Purulent drainage from the incision, pain or tenderness, localized swelling, redness, or heat. Deep incisional SSI was defined as an infection occurring within 30 d after the operation and involving deep soft tissues (e.g., fascial and muscle layers) of the incision and at least one of the following: Purulent drainage from the incision but not from the organ/space component of the surgical site; spontaneous dehiscence or deliberate incision opening by the surgeon with fever (>38°C), localized pain or tenderness, or deep incisional abscess. In case of suspected SSI, microbiologic analysis and pus culture had to be performed.
The occurrence of complications was monitored for 30 d after discharge with regular weekly visits by the same personnel. In case of any incision complication the assessor was required to ask for a second opinion to confirm the event.
End points
The primary outcome measure was the overall rate of incisional SSI (superficial and deep incisional SSI). Secondary end points were length of hospital stay and overall incision complication rate, including skin swelling and redness, hematomas, and seromas.
Statistics
When designing the study, the overall SSI rate was expected to be approximately 15%. This was based on the mean rate of SSI in the four participating centers in the years 2007–2008. A relative reduction of 50% was considered clinically significant. With the planned sample size of 140 patients per arm, the expected width of the two-sided 95% confidence interval for the difference in proportions was 0.17. A dropout rate of 7% for discontinuation of intervention was anticipated, therefore, the target was a total sample size of 300 patients. The primary outcome measure was evaluated by 95% confidence interval of the difference in the proportion of SSI and by the odds ratios (odds ratio, p value were obtained from χ2 test with 1 df). The secondary end points based on proportions were evaluated by odd ratio and 95% confidence interval.
To evaluate the influence of pre- and intra-operative variables on the incidence of SSI, the χ2 test or Fisher exact test when appropriate and t-test were applied for categorical and continuous variables, respectively. A multivariable logistic model was applied including the treatment variable and evaluating the most important risk factors emerging from the literature in a one-step model. From this model, the predicted probabilities of SSI were estimated for hypothetical patients with relevant combinations of risk factors.
Results
Three hundred eighty-seven patients were screened for eligibility for the study and 300 patients were enrolled. One hundred fifty subjects were allocated in the triclosan arm and 150 in the control arm. After randomization, 19 patients (9 in the control arm and 10 in the triclosan arm) underwent re-laparotomy with discontinuation of intervention. This left 141 patients in the control arm and 140 in the triclosan arm for the final analysis (Fig. 1). No patient was lost for follow-up. Table 1 describes the demographic and baseline characteristics, surgical details, and the risk factors for SSI of the two groups. The two groups were well balanced for all the variables considered.
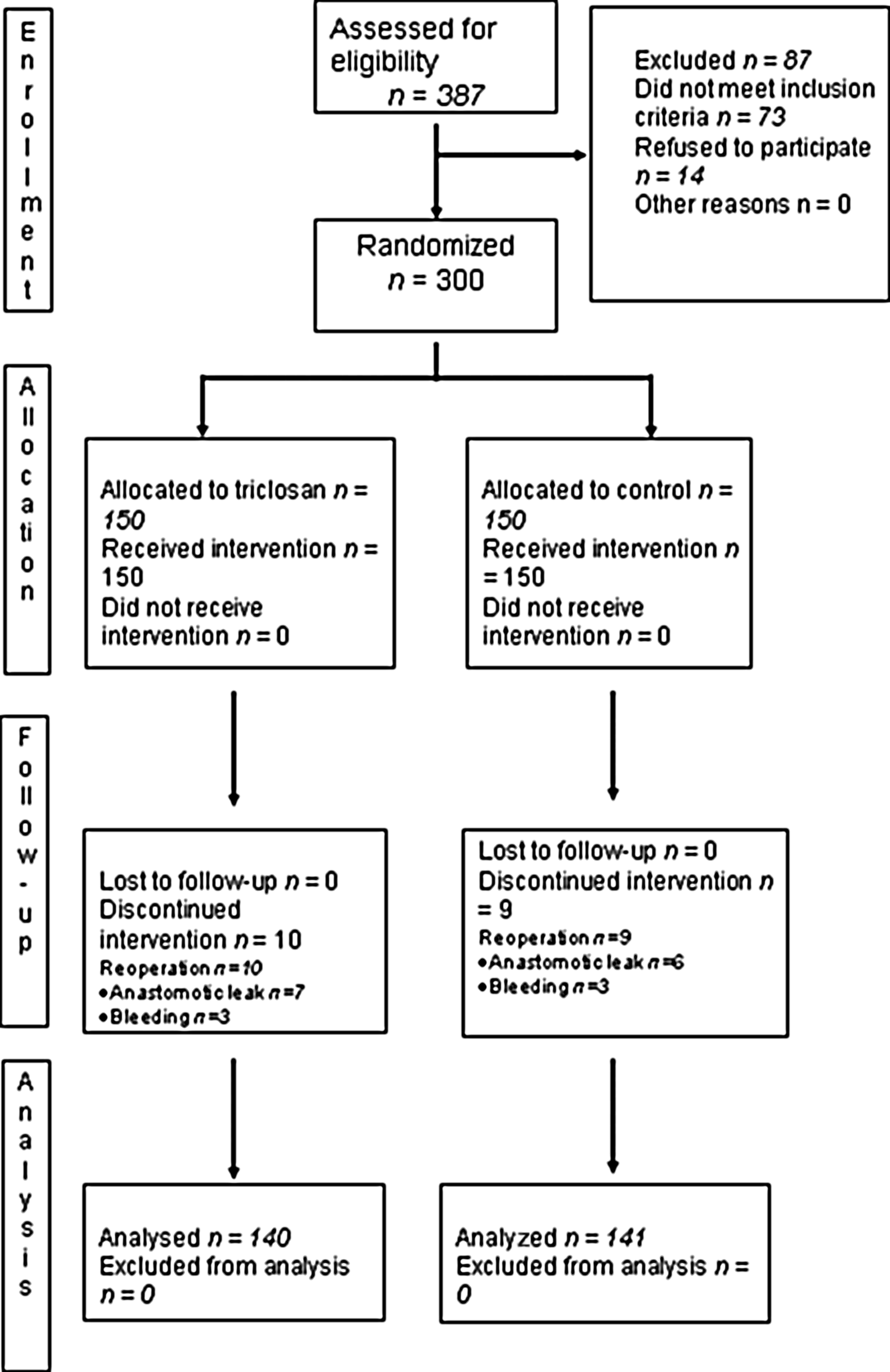
CONSORT diagram for the trial.
Values are median (interquartile range).
Values in parentheses are percentages unless indicated otherwise.
ASA=American Society of Anesthesiologists physical status classification system; PPBLI=penicillins plus β-lactamase inhibitors.
The overall incidence of SSI was 11.7% (33/281), lower than what was expected. The evaluation of the primary end point showed that there was no statistically significant difference in the overall rate of SSI between treated and control groups (difference: 2.2; 95% CI (−5.3–9.7); odds ratio: 1.24; 95% CI: 0.60–2.57; p=0.56). Similar results were obtained when SSI were divided between superficial and deep (Table 2). Among the 33 SSIs, 11 (33.3%) appeared after hospital discharge (4 in the triclosan group and 7 in the control group).
Values in parentheses are percentages unless indicated otherwise.
SSI=surgical site infection; OR=odds ratio; CI=confidence interval.
Secondary outcome analysis showed that the overall wound complication rate was 45.7% in the triclosan group versus 38.3% in control group (odds ratio: 1.36; 95% CI: 0.84–2.18; p=0.21; Table 3). The patients treated with triclosan-coated sutures had significantly more wound hematomas than the control group (9.3% vs. 2.1% respectively; odds ratio: 4.71; 95% CI: 1.31–16.91; p=0.02), while no significant differences were observed for skin swelling, redness, or wound seroma. Duration of hospitalization was similar between groups (p=0.546).
Values in parentheses are percentages unless indicated otherwise.
OR=odds ratio; CI=confidence interval; SD=standard deviation.
Table 4 shows the results of the univariate analysis of single risk factors on the occurrence of SSI. Antibiotic prophylaxis with a single dose was the only parameter that was associated with a significant reduction of SSI compared with multiple doses. Other variables such as BMI <30, the use of penicillins plus β-lactamase inhibitors (PPBLI) for prophylaxis, and not suturing the subcutaneous fat tissue did not reach statistical significance.
Values in parentheses are percentages unless indicated otherwise.
SSI=surgical site infection; BMI=body mass index; ASA=American Society of Anesthesiologists physical status classification system; PPBLI=penicillins plus β-lactamase inhibitors;
The multivariable logistic regression analysis (Table 5) provided an estimate of the treatment effect (OR: 1.26, 95% CI: 0.59; 2.69). Regarding risk factors, results showed that giving multiple antibiotic doses was significantly associated with a fourfold increased risk of SSI compared with single dose (p=0.01), after adjusting for type of antibiotics, BMI, and whether the patients had or did not have a subcutaneous tissue suture. Moreover, compared with PPBLI, other antibiotics were related to a sixfold increase in the odds of developing an SSI, although this did not reach statistical significance (p=0.098).
OR=odds ratio; CI=confidence interval; BMI=body mass index; PPBLI=penicillins plus β-lactamase inhibitors.
By constructing a statistical model we evaluated the potential combinations of factors increasing the likelihood of developing SSI in patients with certain characteristics (Fig. 2). Obese patients receiving multiple prophylactic antibiotic doses with drugs other than PPBLI and having subcutaneous tissue sutured had a probability of SSI of 34.1% in the triclosan group and 29.1% in the control group. These probabilities decreased to 18.9% and 15.5%, respectively, in non-obese patients with the same characteristics. In contrast, when none of the above variables were present, the chance of an SSI was 1.3% in the triclosan group and 1.1% in the control group.

Predicted probabilities of SSI and 95% confidence intervals estimated from the multivariate model for hypothetical patients with relevant combinations of risk factors (dots and continuous lines). Dashed line reports the overall incidence of SSI. SSI=surgical site infection; C=control group; T=triclosan group; Y=yes; N=no.
Table 6 presents the details of the bacteria isolated from the incisions in the patients who developed infections. The results show that in the vast majority of patients, gram-negative Enterobacteriaceae were the most frequent isolates, followed Pseudomonas aeruginosa. Only occasionally were gram-positive such as enterococci and Staphylococcus aureus identified. No difference was observed between groups.
ND=not determined.
Discussion
There is justification for assuming that the use of sutures impregnated with triclosan may reduce the risk of SSI. Triclosan has demonstrated antiseptic properties primarily against gram-positive pathogens [22,23], but its effect against various E. coli strains was also proved in orthopedic operations [24,25]. Moreover, the coating provides prolonged protection against colonization of the tissue around the sutures because its effects last for approximately 1 mo [14,26]. This makes the use of triclosan-coated sutures even more attractive because of the considerable proportion of SSI presenting late after surgery [27]. Preliminary clinical results from a large retrospective analysis [28] were quite promising on the ability of triclosan-coated materials to prevent the occurrence of SSI but most of the subsequent RCTs [15], even if conducted in heterogeneous cohorts, failed to demonstrate clear benefits on incision infection and complication rates. Colorectal surgery may represent a favorable clinical model to evaluate the effect of sutures impregnated with triclosan because of the high incidence of SSI and thus limiting the trial sample size and the polymicrobial origin of SSI allowing an in vivo appraisal of the antimicrobial spectrum of triclosan.
The results of the present RCT do not support the hypothesis that triclosan-coated sutures decrease the rate of post-operative SSI. Our findings are consistent with the results of Baracs et al. [17], who showed in a similar population of 385 patients undergoing comparable surgical procedures an overall rate of incision infection of 12.5% with no significant difference between the group treated with triclosan-coated sutures (12.2%) and uncoated sutures (12.2%). As in our study, they used a running triclosan-coated polydioxanone to close the abdominal fascia; peritoneum and subcutaneous layer closure was optional and the rate of implementation was not reported.
Our data are in contrast to those reported in a single-center RCT conducted in Japan [19]. The authors found that suturing the abdominal wall with triclosan-coated polyglactin 910 was significantly effective in reducing the incidence of incision infection in patients undergoing colorectal resection. The incidence of SSI in their study group was 4.3% (9/206), and 9.3% (19/204) in the control group (p=0.047). This difference was mainly because of infections occurring in patients who underwent open surgery. The potential differences in the study design, such as type of suture, interrupted sutures, single-layer abdominal closure, and skin closure may partially explain the conflicting results. Probably more important in interpreting the discrepancies of results among trials is the composition of the colonic microbiota that differs substantially in different populations mainly according to alimentary habits and environmental conditions [29–31]. Because the main source of SSI after colorectal resection is the intestinal flora, different bacterial strains harboring the gut and their susceptibility to the antimicrobial properties of triclosan may account for the inconsistent results among trials conducted in different countries. In fact, in the study by Nakamura et al. [19], enterococci were by far the most frequent isolates (54%), and the second most common infections was caused by Bacteroides species (36%). In our series, enterococci was present in fewer than 20% of the cases and gram-negative enterobacteriaceae (Escherichia, Klebsiella, Proteus, Enterobacter, Citrobacter, Morganella) and Pseudomonas aeruginosa were the most common isolates accounting for more than 80% of the infections. This partially confirms the limited in vivo efficacy of triclosan on several species of gram-negative bacteria [32]. However, in our series 42% of the incision infections were not confirmed by microbiologic and culture analysis. These data might be explained by the fact that one-third of the infections were evident after hospital discharge. Our health care system does not provide reimbursement for outpatient laboratory tests; the cost of the analysis was to be paid entirely by the patient, who declined it.
Safety studies on triclosan have been performed in the past, mainly focusing on systemic toxicity and local adverse reactions. Overall, these studies showed that systemic concentrations of triclosan are low when applied topically [13]. Although triclosan is relatively non-toxic in classic toxicologic terms, negative effects such as dermatitis, skin irritation, and allergic reactions have been described [33]. The safety of use in suture materials has been proved repeatedly although a recent study by Deliaert et al. [34] reported a negative effect on incision healing after breast reduction surgery. Our results showed that in patients treated with triclosan-coated sutures there was an increase of wound hematomas. Such local side effects were not reported previously. The reason is unknown and difficult to explain on the basis of the identified safety reports. It can be speculated that the release of triclosan in the incision may interfere with some local coagulation pathways or platelet function. This minor side effect might be attributed to the broad use of triclosan-coated sutures in our study. In fact, we utilized four sutures to close peritoneum, fascia, subcutaneous fat tissue, and skin while previous similar trials used only one or two sutures.
Using a multiple logistic regression analysis we investigated four key variables for SSI. The use of PPBLI for antibiotic prophylaxis and a single dose of antibiotics were the most protective factors against the development of SSI but also BMI <30 and not suturing the subcutaneous tissues were related to a lesser risk. Taken singularly these elements have not been identified commonly as relevant variables for the occurrence of postoperative infections. Obesity is a well-recognized risk factor [35], whereas the role of PPBLI versus other drugs as prophylactic agent [36], a single dose versus repeated antibiotic doses [37], and suturing versus not suturing of the subcutaneous layer [38] have been reported as comparable for the risk of SSI. The description of the SSI risk according to different combinations of the these variables showed that when all risk factors were present (obesity, suture of subcutaneous tissue, multiple antibiotic doses, and not using PPBLI) the risk was approximately 30% and only when obesity was not present was the risk reduced by 50% regardless the type of suture used. On the contrary, when all these variables were absent the risk of SSI almost disappeared (∼1%). These results may have clinical relevance because the use of subcutaneous tissue sutures may increase infection risk in obese patients, perhaps by adding foreign material.
Our trial has several methodologic limitations. The operating surgeon was not blinded to the intervention despite random assignment being done after the colorectal resection was completed and both patients and assessors being unaware of the randomization arm. Moreover, the randomization was not balanced for important and known patient and operative risk factors for SSIs.
Despite prevention of intra-operative hypothermia being performed routinely, body temperature was not recorded in the database. Therefore, we could not assess the role of hypothermia on the occurrence of SSI. In our study there was no predefined prophylactic antibiotic regimen and dosing, and 40% of the reported SSI was not confirmed by positive culture although a second assessor had to confirm the event. Our univariate and multivariable analyses may have suffered from the small number of events potentially leading to variability in treatment effects due to a type II error. Furthermore, a multi-center trial may introduce bias linked to the heterogeneity of surgical techniques, sanitary behaviors of the personnel, and judgment practices among centers.
Conclusions
The present trial failed to demonstrate a protective effect of triclosan-coated sutures on the occurrence of SSI. Our data suggest that the extensive use of such sutures have some local side effects. Given the conflicting results in the literature on the benefit and harm of triclosan-impregnated materials on incision healing, further large RCTs are needed before introducing it in a routine clinical use.
Footnotes
Acknowledgment
This trial was funded by a research grant of the University of Milano-Bicocca.
Author Disclosure Statement
No competing financial interests exist.