
Abstract
Abstract
Background:
Prosthetic mesh is employed routinely in the treatment of ventral and parastomal hernias, but its use can lead to major complications, including infection, extrusion, and fistula. Bacterial biofilms have been posited to play a role in mesh-related infection, but although bacteria have been noted to form biofilms on mesh surfaces in vitro, they have never been visualized directly in biofilms on mesh recovered from patients experiencing infectious complications.
Methods:
Five patients who developed complications after ventral hernia repair with prosthetic mesh were operated on again. Explanted mesh was examined for biofilm with confocal laser scanning microscopy (CLSM) and fluorescence in situ hybridization (FISH). In two cases, a novel molecular assay (the Ibis T5000) was used to characterize the biofilm-forming bacteria.
Results:
The CLSM examination demonstrated adherent biofilms on mesh surfaces in all five patients. Biofilms also were noted on investing fibrous tissue. The FISH study was able to discriminate between bacterial species in polymicrobial biofilms. In two patients the Ibis T5000 detected more species of constituent biofilm bacteria than did standard culture. Removal of the mesh and reconstruction with autologous tissues or biologic materials resolved the presenting complaints in all cases.
Conclusion:
Bacterial biofilms should be considered an important contributor to the pathology and complications associated with prosthetic mesh implanted in the abdominal wall. If biofilms are present, complete removal of the mesh and repair of the resulting defect without alloplastic materials is an effective intervention.
V
Complications are common after prosthetic mesh placement and can conclude failure (recurrent hernia), adhesion, pain, infection, enterocutaneous fistula, and so on. Infection of mesh requiring explantation has become an increasingly recognized problem, and a dedicated Current Procedural Terminology (CPT) code has been added for cases that require mesh explantation, namely 11008: “Removal of prosthetic material or mesh, abdominal wall for infection (e.g., for chronic or recurrent mesh infection or necrotizing soft tissue infection).” Some studies have found a mesh-infection rate as high as 8% [3,4], itself a substantial additional healthcare burden, given the high-volume use of prosthetic mesh.
As a permanent implanted foreign body, prosthetic mesh may be vulnerable to colonization by microorganisms and to the formation of bacterial biofilms. Biofilms are organized communities of microbes typically attached to a surface (either native or abiotic) that display markedly different physiology from free-floating planktonic bacteria: They are vastly more resistant to antibiotics, they are shielded from host defense mechanisms, and they are recalcitrant to ordinary microbiologic culture [5]. Biofilm-based infections are now believed to account for the majority of human infectious diseases, including such well-characterized examples as prosthetic joint infection, otitis media, cystic fibrosis, and endocarditis [6]. Biofilms are especially important in chronic infections but also can serve as the nidus from which acute infectious episodes arise as a result of “showering” of planktonic bacteria that detach from the biofilm complex.
Several studies have documented in vitro that multiple species of bacteria can attach to prosthetic mesh surfaces and form biofilms [7,8]. Reśliński et al. [9] inferred that biofilm was implicated in a recurring surgical site infection associated with mesh by recovering bacterial DNA from the mesh and using formazan metabolic stain to infer bacterial metabolic activity on the mesh surface. We have used confocal microscopy to identify bacterial biofilms on chronically infected sutures [10,11]; however, there has as yet been no reported direct observation of bacteria in a biofilm configuration on surgical mesh recovered from patients experiencing infectious complications. Using confocal microscopy and fluorescence in situ hybridization (FISH), we determined if bacterial biofilms were present on explanted surgical meshes from patients undergoing re-operative surgery for complications after ventral herniorrhaphy. In two instances, we employed a novel multiprimer polymerase chain reaction (PCR)–mass spectrometric technology (the Ibis T5000; Abbott Molecular Diagnostics, DePlaines, IL) to obtain a molecular profile of the resident micro-organisms.
Patients and Methods
Five patients presenting with complaints after ventral herniorrhaphy requiring re-operation were included in this study (Table 1). In each case, the prosthetic mesh was explanted, and the re-created hernia defect was repaired without the use of alloplastic materials (in one case, an acellular dermal graft was used). Pieces of explanted mesh, as well as surrounding fibrous tissue, were gathered aseptically as described previously [10,11]. Specimens were examined by confocal laser scanning microscopy (CLSM) and bacterial FISH as described below. In two cases, total nucleic acids were extracted from samples and analyzed with the Ibis T5000 device. Clinical characteristics of the patients' courses were tabulated. These studies were conducted in accordance with the ethical standards of the Helsinki Declaration of 1975 and with Institutional Review Board approval.
Abx=antibiotics; ADM=acellular dermal matrix graft; APR=abdominoperineal resection; F/U=followup; I+D=incision and drainage; KUGEL™ Hernia Patch, Davol, Warwick, RI; Para=parastomal; Polyprop=polypropylene; RYGB=Roux-en-Y gastric bypass; SBO=small bowel obstruction; Sep=separation; Sepra=Seprafilm™ (Sanofi-Aventis U.S., LLC, Bridgewater, NJ); VH=ventral hernia; X-lap=exploratory laparotomy.
Confocal microscopy and detection of biofilm
In addition to standard microbiologic culture, specimens from surgery (both mesh and investing tissue) were examined with CLSM for the presence and viability of bacteria and biofilms, and FISH was used to identify specific targeted bacteria as described previously [12]. Specimens were examined or fixed either the day of surgery or the following morning.
To identify live bacteria, we used the BacLight Live/Dead kit (Invitrogen, Carlsbad, CA). The BacLight kit consists of the nucleic acid stains Syto9 (green) and propidium iodide (red). Both live and dead bacteria take up Syto9, but only bacteria with permeable cell walls (presumed to be dead or damaged) take up the propidium iodide, which displaces the Syto9 and gives a red color. In some cases, bacteria retain both stains and appear yellow in confocal overlays; these cells have been interpreted as living but damaged. Human nuclei also take up both stains, but virtually all cells take up propidium iodide rapidly and turn red regardless of viability. Human cells are readily distinguishable from bacterial cells by morphology and size. The mesh substance itself was imaged using either the natural autofluorescence of the material or reflected 488-nm light. Our technique for fresh specimens using a water immersion microscope objective ensures that the samples were never dehydrated and that we observed only firmly attached bacteria (unattached planktonic cells were removed by rinsing).
Fluorescence in situ hybridization
We used FISH to identify Staphylococcus aureus or Enterococcus spp. Mesh and associated tissue was mounted in 35-mm petri plates as previously described and fixed in 4% paraformaldehyde (PFA; Electron Microscopy Sciences, Hatfield, PA) in 3× phosphate-buffered saline (PBS) for 12 h at 4°C to preserve structure and permeabilize the bacteria, allowing uptake of the FISH probe [13]. The tissue was washed three times with PBS. The buffer was removed, and the tissue was submerged in 50% PBS/50% ethanol solution and stored at −20°C until staining. To permeabilize the bacteria further, specimens were treated with 0.5 mg/mL lysozyme (Sigma-Aldrich, St Louis, MO) in 0.1M Tris HCl (Sigma-Aldrich) to pH 8.0 and 0.05M disodium ethylenediaminetetraacetic acid (Sigma-Aldrich) for 3 h at 37°C and washed with ultrapure water. The sample was dehydrated in a graded series of ethanol (50%, 80%, and 100%) for 3 min at each concentration. The FISH was performed using either the S. aureus-specific 16S ribosomal probe Sau 5′-GAAGCAAGCTTCTCGTCCG-3′ [13] or the Str 5′-CACTCTCCCCTTCTGCAC-3′ Streptococcus spp. probe [14]. The Str genus FISH probe hybridized with the isolated strain Enterococcus faecalis (data not shown). This was not surprising, as Enterococcus is closely related to Streptococcus, and indeed, E. faecalis was classified formerly as a Group D streptococcus. As a negative control, the Str probe did not hybridize with the S. aureus isolate (data not shown). The FISH probes were labeled with either the green fluorescent probe Cy3 or 6-carboxy-fluorescine (FAM) (Integrated DNA Technologies Inc., Coralville, Iowa). The eubacterial probe Eub338 5′-GCTGCCTCCCGTAGGAGT-3′ conjugated with Cy5 (red) was used as a general bacterial stain [15]. We also used propidium iodide or Syto9 (Molecular Probes) as non-specific bacterial stains, and these probes also stain the nuclei of host cells red or green, respectively, but these cells are readily distinguishable from bacteria by morphology and size. The specimens were imaged after submersion in Hank's Balanced Salt Solution with a 63× water immersion objective.
Ibis T5000
In two cases, specimens were assayed for microbial content with the Ibis T5000, a novel technology that uses 16 primer sets designed to canvass more than 3,000 known eubacterial organisms and Candida to amplify any template DNA (or mix of DNAs) blindly. The resulting amplimers are then subjected to electrospray ionization mass spectrometry to resolve their molecular weights, and the results are compared with the Ibis reference library. The assay is rapid (∼6 h from the time DNA is presented to it) and capable of delivering data down to the species level. It is semi-quantitative, yielding estimates of the number of genome copies per well, and can detect the genes responsible for major patterns of antibiotic resistance. It features additional internal primers to control for false-negative results and provides an algorithmical “confidence value” to itself gauge the likely accuracy of its results. The Ibis system is now approved by regulatory agencies for use in clinical diagnostics; we have used it to investigate clinical samples from multiple sources.
In patient four, a single sample was tested; in patient five, separate samples from two discontinuous areas of mesh were examined. Extraction of total nucleic acid from the specimens was performed as described previously [16,17]. The Ibis results were considered positive only if at least two distinct primer sets corroborated the result, if the confidence value of the call exceeded 0.70, and if no corresponding result was detected in the control “no template added” runs.
Results
There was no uniformity in the initial surgical episode that created the hernia for which mesh was placed, nor in the types of mesh used or their positioning. The presenting complaints also showed a wide range, from chronic pain alone, to non-healing incisions and recurrent hernia, to frank infection and enterocutaneous fistula formation. In two patients, an earlier operation had already removed the implanted mesh, in one case only partially (patient one) and in the other completely (patient four) but with immediate placement of a new mesh. Three patients had previous antibiotic therapy without resolution of their symptoms. Reconstruction of the abdominal wall defect after mesh removal was accomplished by separation of components in two cases, and use of autologous and acellular dermal grafts in two others. In one case with an onlay mesh only, no repair was necessary, as no defect resulted after mesh removal. All patients ultimately had complete healing of their incisions, and none had recurrent hernias at the site of repair with lengthy follow-up. One patient did develop a new parastomal hernia at the site of his re-located ostomy, and one patient underwent exploratory laparotomy to rule out internal hernia and small bowel obstruction, but subsequently healed well. Pre-, intra-, and post-operative photos of the patients are shown in Fig. 1.
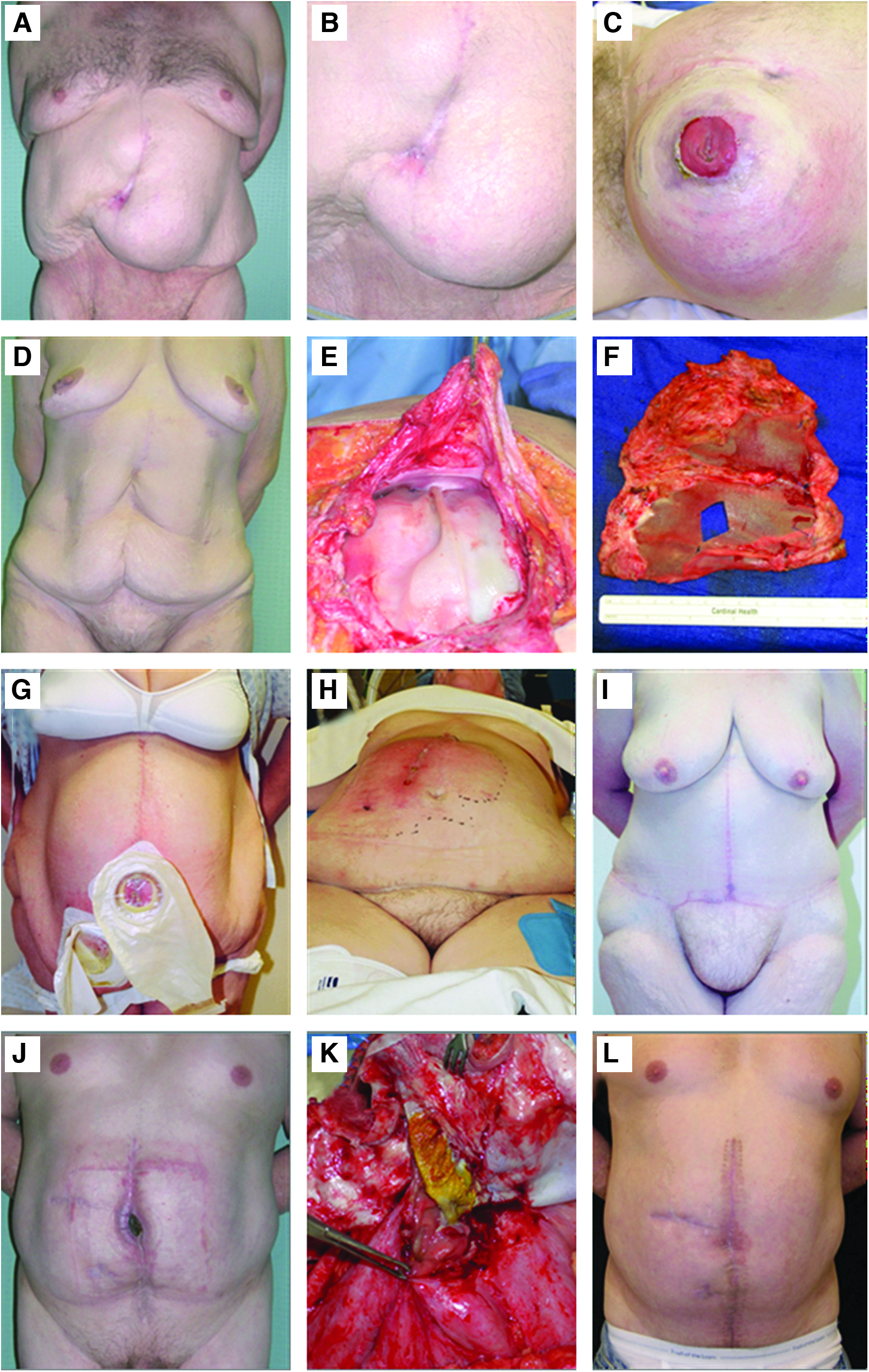
Pre-operative, intra-operative, and post-operative images of patients undergoing mesh explantation.
All explanted meshes had clear evidence of bacterial biofilms in residence. The CLSM using Live/Dead staining identified adherent communities of viable bacteria in every case, often showing both bacilli and cocci, indicative of a polymicrobial infection (Fig. 2). Fibrous tissue surrounding the mesh also was found to host biofilm. Bacterial FISH in some instances was able to speciate the constituent microorganisms in polymicrobial biofilms (Fig. 3). In one case, Enterococcus and S. aureus were demonstrated in intimate association, seemingly forming clusters of attached bacteria cooperatively. In another, abundant S. aureus was found cheek-by-jowl with distinctly rod-shaped bacteria at one location, but only sparse S. aureus was seen in other clusters dominated by non-S. aureus cocci, showing that even within an individual patient, the biofilm composition was heterogeneous. These data demonstrate conclusively that prosthetic mesh is a relevant substrate for bacterial biofilm formation in vivo.
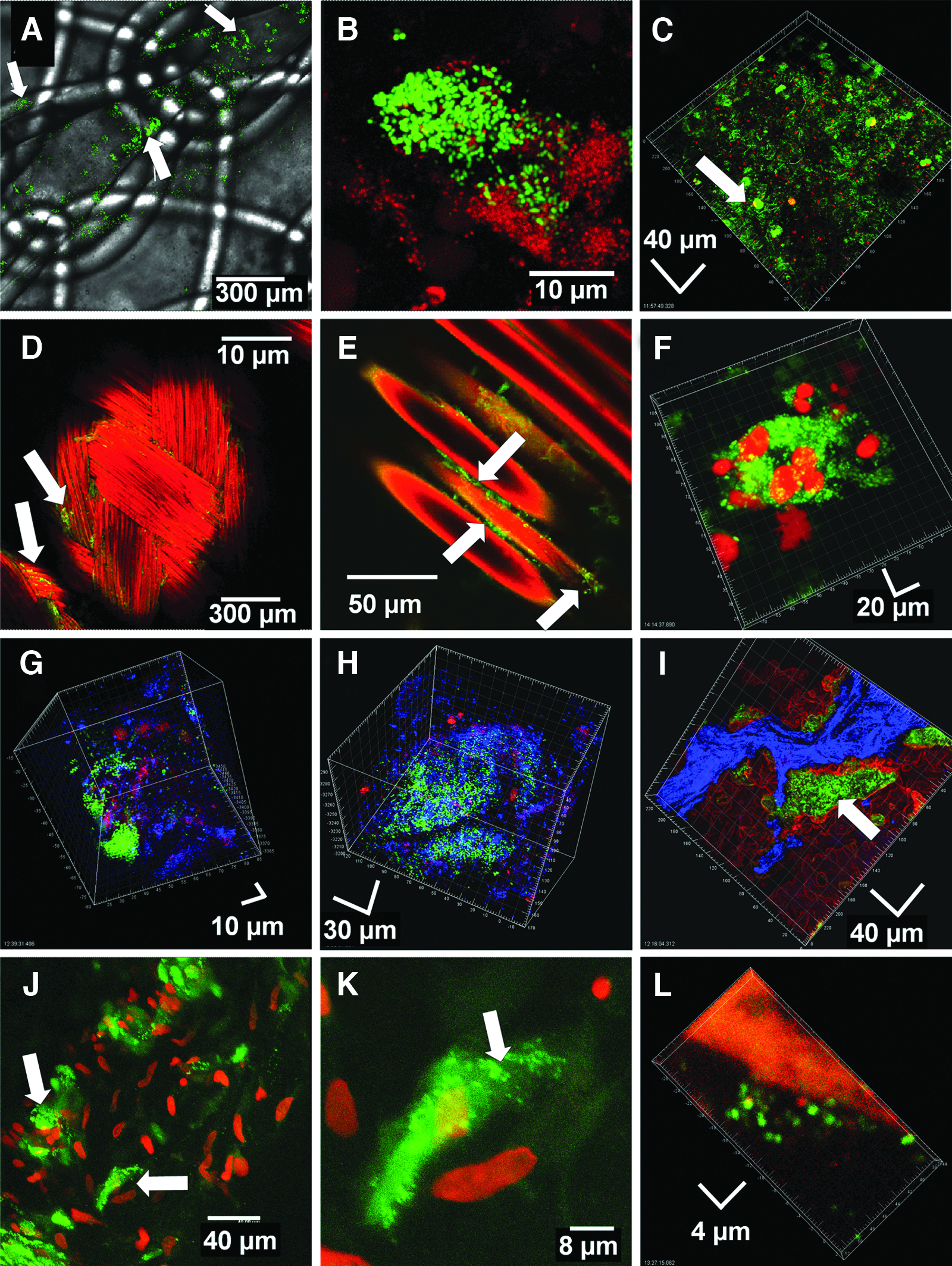
Confocal micrographs showing live bacteria in biofilm on mesh, an anchoring suture, and reactive tissue from five patients. (
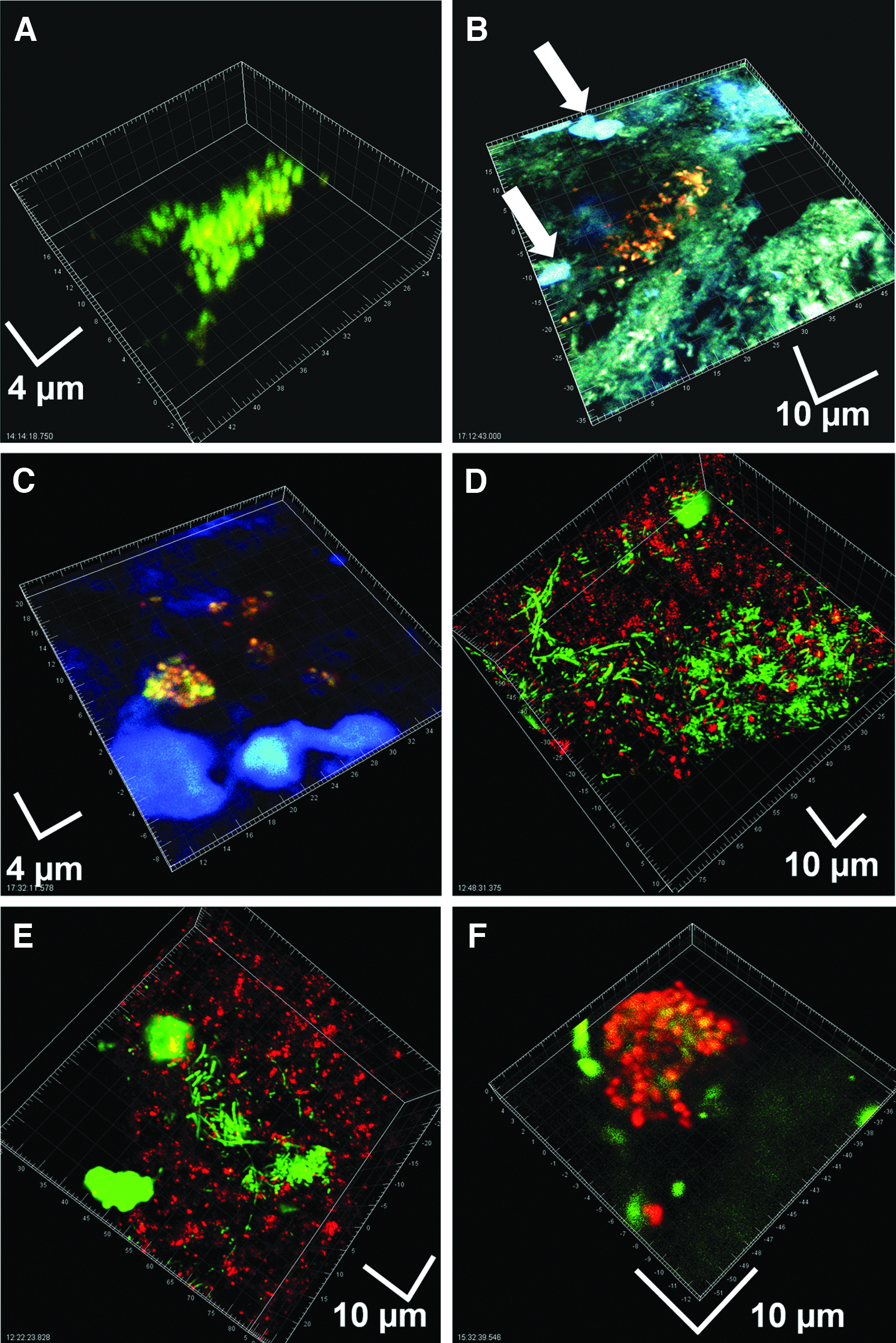
Fluorescence in situ hybridization (FISH) imaging of mesh and tissue from patients four and five demonstrating polymicrobial biofilms. (
In two cases, we used a novel multiprimer PCR-mass spectrometric technology, the Ibis T5000, to determine the constituent microorganisms of the biofilm on the basis of DNA content in addition to plain culture (Table 2). An early attempt to use Ibis found three component bacteria (S. aureus, E. faecalis, and Enterobacter cloacae) in patient 4. Interestingly, these same samples were cultured in two separate laboratories, with one reporting S. aureus and E. faecalis only, and the other growing S. aureus and E. cloacae only. Only the Ibis technology identified all three resident species. Use of Ibis to examine the dense biofilm residing on mesh involved with an enterocutaneous fistula revealed numerous species of bacteria beyond those identified by culture alone. Many of these (e.g., Lactobacillus, Bifidobacterium, Campylobacter) were unsurprising, given the enteric nature of the incision site. Ibis also confirmed the presence of the mecA gene and thus the presence of methicillin-resistant S. aureus. Strikingly, multiple unexpected bacteria also were found. Both samples of mesh tested were found to harbor large amounts of DNA from the predatory bacterium Bdellovibrio bacteriovorus, which has not been implicated previously in human disease, and one also was positive for Rhodopseudomonas palustris, known as a photosynthetic bacterium.
Note that in patient four, Ibis detected three species, whereas two independent laboratories both failed to recover all three by culture, although additively, they did validate the Ibis findings. No reliable quantitative information was obtained in this early Ibis assay. In patient five, Ibis examination of two samples (5a and 5b) revealed numerous species undetected by culture. Genome copies per well are noted. Although three species were common to both samples, six were not, indicating the heterogeneity of the biofilm.
Discussion
Although the propensity of bacteria to form biofilms on commonly used mesh materials has been investigated in vitro, clinical confirmation that this is a relevant in vivo process has thus far been lacking. A single case of biofilm bacteria on explanted mesh has been reported [9], but in that case, bacterial viability was inferred from a metabolic assay but not confirmed. No micrographic evidence of communities of attached bacteria was presented, and standard culture was used to identify the resident micro-organisms, an oftentimes-inadequate tool given the resistance of biofilm bacteria to culture. The present report is the first direct demonstration of viable bacteria in biofilm configuration attached to prosthetic mesh retrieved from patients experiencing infectious complications.
Although the criteria for diagnosing biofilm-associated infections are still being refined, we suggest that the clinical consequences suffered by these patients derive from bacterial biofilms by application of the criteria proposed originally by Parsek and Singh [18]. These are enumerated and explicated as follows: (1) “The infecting bacteria were adherent to some substratum or are surface-associated.” Our confocal micrographs clearly depict bacteria adherent to both abiotic (mesh) and associated soft tissue surfaces. (2) “Direct examination of infected tissue shows bacteria living in cell clusters, or microcolonies, encased in an extracellular matrix.” Our confocal micrographs clearly depict bacteria in aggregates, often polymicrobial, as demonstrated by morphology or FISH. Extracellular matrix was not stained specifically in this study, but nevertheless appeared occasionally, as in Fig. 2K, where a hazy enveloping substance can be seen surrounding the bacterial cluster. (3) “The infection is generally confined to a particular location. Although dissemination may occur, it is a secondary phenomenon.” In all of our cases, the infection affected the tissues of the abdominal wall or structures directly adjacent (bowel). In no case did the infection progress to bacteremia or manifest at remote sites. (4) “The infection is difficult or impossible to eradicate with antibiotics despite the fact that the responsible organisms are susceptible to killing in the planktonic state.” Three of our patients were treated unsuccessfully with antibiotics (both oral and parenteral).
Even in this small series, there is considerable variety in the clinical dimensions of the biofilm infections. Although such infections classically are believed to manifest with low-grade but chronic or recurrent complaints, they also can serve as the source of acute infectious exacerbations, that may arise from detachment of “planktonic” bacteria from the biofilm, which are then more able to provoke a fulminant course. Such a phenomenon may explain the appearance of cellulitis and abscess in patient four after a long period with only draining sinuses, and the appearance of cellulitis (accompanied by bowel obstruction) in patient three. It is possible that unrecognized biofilm plays a role in mesh failure, leading to hernia recurrence. In this scenario, the presence of a subclinical biofilm may lead to a localized inflammatory response that, while ineffective in clearing the biofilm, may prove injurious to the surrounding tissues and prevent mesh incorporation. It may even cause tissue resorption: We have reported previously a case where a biofilm on implanted abdominal wall suture material led to chronic surgical site infection that progressed ultimately to frank gastrocutaneous fistula [11]. We also have managed multiple other cases where suture used for musculofascial closure that was found to host biofilm has been coincident with the loci of hernia formation, whereas sutures without biofilm in the same patient were free of subjacent hernia defects.
Patient 2 is particularly interesting in that her only complaint was abdominal pain; she had no evidence externally of any infectious process (see Fig. 1D). We suggest that pain alone, even in the absence of any other inflammatory signs and symptoms, may be indicative of an underlying biofilm process. We previously reported a case where pain was the only presenting symptom after inguinal herniorrhaphy, in which biofilm was found to reside on a porcine xenograft that had been placed at the time of repair [19]. Removal of the graft (and therefore the biofilm) and repair with autologous tissue resolved the pain; patient two also had marked improvement of her pain after mesh explantation. In orthopedic prosthetic joint infection, also a biofilm-mediated disease, pain can be the sole presenting symptom.
Patient five, at the other extreme, presented to us with an enterocutaneous fistula. The biofilm we document in this report was post-fistula, and we are unable to assess what role biofilms played in the development of the fistula itself. However, given our observation that suture-associated biofilm can lead to gastrocutaneous fistula, it may similarly be possible for mesh-associated biofilm to lead to enterocutaneous fistula.
In this report, we used a combination of methods (Live/Dead confocal imaging, bacterial FISH, and Ibis T5000) to document the polymicrobial nature of some of the biofilms. Because biofilm bacteria are recalcitrant to standard culture, culture alone underestimates frequently the complexity of a biofilm community, which often appears to be culture-negative. Micrographic methods remain the gold standard for biofilm diagnosis, because they reveal the spatial arrangement of the biofilm, confirm that the biofilms are the result of a “growth in place” process (not incidental free-floating bacterial contaminants), and can even speciate the organisms with the use of FISH. However, micrographic methods are labor-intensive, require specialized expertise, and examine only a minute fraction of the material typically gathered at aspiration/biopsy/surgery. Molecular means of detecting biofilm bacteria therefore are becoming increasingly common, with most such assays relying on PCR amplification, typically of bacterial 16S rDNA sequences [20]. We used the Ibis T5000 multiprimer PCR-mass spectrometric assay to examine the bacterial components of our biofilms in two cases.
The Ibis results are striking. Ibis examination of patient four was very early in our experience, and we did not obtain reliable quantitative data, but Ibis did identify three species involved in the biofilm (Table 2). By comparison, standard microbiologic culture by the hospital microbiology laboratory identified only two species (S. aureus and E. faecalis), and our own cultures of the specimens likewise yielded only two (S. aureus and E. cloacae), but together, these results confirmed the Ibis data, showing the presence of three species. Ibis was even more revealing in patient five, whose biofilm derived from an enterocutaneous fistula. Numerous organisms were detected beyond those cultured, and two separate pieces of mesh harbored somewhat different bacterial species, again showing that polymicrobial biofilms can be heterogeneous in their composition even within an individual patient. Although many of the species detected were unsurprising, as they are known enteric or cutaneous flora (e.g., Lactobacillus, Bifidobacterium, Campylobacter, S. aureus, S. intermedius), some were unexpected. Rhodopseudomonas palustris is best understood as a marine and terrestrial photosynthetic organism, although Rhodopseudomonas spp. have been noted in chronic wounds [21]. Even more surprisingly, the single most common bacterium in both specimens was Bdellovibrio bacteriovorus, a predatory bacterium that invades and kills gram-negative bacteria. Indeed, Bdellovibrio has been contemplated as a probiotic agent that could be effective against biofilm-forming enteric pathogens and has been isolated from human and animal intestines [22]. Its role in perpetuating or combating the biofilm involved with this fistula remains unclear. It remains possible (perhaps likely) that many more types of bacteria were involved in this biofilm, beyond even the ability of the Ibis to detect in this circumstance.
In sum, we demonstrated for the first time bacterial biofilms on mesh in patients that likely contributed to the mesh-related complications experienced by said patients. These biofilms were frequently polymicrobial and underappreciated by culture alone. We demonstrated the utility of a novel technology, the Ibis T5000, to characterize better the organisms present on mesh surfaces. Removal of the mesh substratum and all associated reactive and fibrous tissue (which is itself host to biofilm) in all cases led to resolution of the presenting complaints. These observations clarify the importance of bacterial biofilms in mesh-related infections.
Acknowledgments
We acknowledge the support of the Department of Surgery, Allegheny General Hospital, in conducting this work. This work also was supported in part by a grant from the National Institutes of Health to SK (DE014780).
Author Disclosure Statement
The authors have no conflicts of interest to disclose.