
Abstract

E
A 70-year-old male presented to the emergency department with a 5 d history of painful mass in the right groin. During that period the mass increased in size with increasing pain. The patient had undergone a coronary angiography through the right femoral artery 1 mo ago due to angina pectoris. There was no history of groin hernia. The patient was afebrile without vomiting or abdominal pain, and with regular daily passage of stool and flatus. The mass was tender, irreducible, 3 cm in diameter, and did not increase with Valsalva maneuver. The mass was not pulsatile. Overlying skin was normal without signs of previous puncture or hematoma (Fig. 1) and pseudo-aneurysm was excluded clinically. The scrotal skin and testicles were normal without signs of tumor or infection. There was no other infective process present in the body. Plain abdominal radiograph was unremarkable.
The encapsulated dense yellowish pus collection measuring, 4×2 cm was found in the spermatic cord. Microbiology showed Staphylococcus aureus.
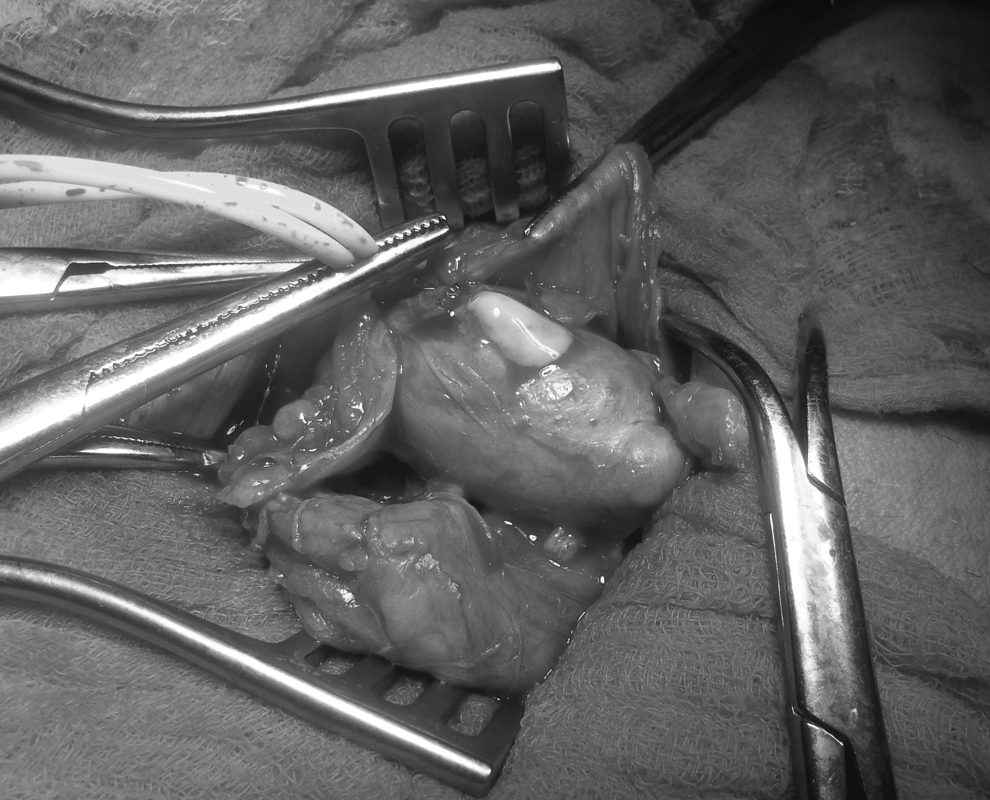
The conclusion was that emergency operation was indicated due to incarcerated inguinal hernia. During the operation, an irreducible mass was found in the spermatic cord. After division of the cremaster muscle, an oval encapsulated mass 4×2 cm was found without elements of a groin hernia (Fig. 2). The abscess was removed with the capsule intact. Because dense white-yellowish pus was present, empiric antibiotic therapy was administered against S. aureus with cloxacillin and gentamicin. The wound was left open with daily cleansing, with delayed primary closure on the third post-operative day. Cultures confirmed S. aureus sensitive to cloxacillin that was continued for 5 d post-operatively. During hospitalization the patient was afebrile. After 3 mo the patient was symptomfree.

Encapsulated pus was dissected from other structures of the spermatic cord and there were no signs of indirect or direct inguinal hernia.
The differential diagnosis of groin mass includes variety of conditions that could be divided into primary groin conditions and distant primary pathologic processes extending into the groin. The most common primary spermatic cord pathology includes tumors—rare primary tumors of the spermatic cord [3] or metastatic tumors to the cord [4]. Tumors often manifest as painless, slow-growing mass in the groin. Features suggestive of malignant disease include rapid growth, large size, and symptomatic presentation. Infections may present as tender masses with other symptoms and signs of infection: An infective process can be inoculated, may extend from a surrounding infection, or hematogenous. The third group consists of spermatic cord hematomas that may be idiopathic, traumatic, secondary to anticoagulation therapy, or as an extension of a retroperitoneal hemorrhage [5].
Whereas common inguinoscrotal swellings (hernias and hydrocoeles) can be diagnosed on clinical examination, all atypical swellings should be investigated further before surgical exploration. In our case there was no fever or signs of inflammation of the overlying skin. This is due to the small size of the abscess and its location in the deeper structures. Ultrasonography is the modality of choice to detect and evaluate spermatic cord pathology. Computed tomography is important for defining benign or malignant potential of spermatic cord tumors, equivocal ultrasound findings, or primary pathology extending to the groin. Radiologic suspicion of malignant tumor directs the surgeon to perform a wide local excision, thus avoiding the need for further re-excisions and reducing the risk of disease recurrence.
Emergent presentations of groin masses rarely benefit from therapy. Most presentations are incarcerated inguinal hernias, necrotic enlarged lymph nodes with or without abscess, an abscess from other localizations draining into the inguinal region, infected hematomas, (pseudo)aneurysms, or even sebaceous cysts (inflamed or non-inflamed). The sebaceous cyst mostly grows slowly but if inflammation is present it can enlarge over hours to days. Ultrasonography reveals the underlying cause in most cases and could be performed easily in emergency settings. It is important to define whether the pathology in the groin is secondary because the underlying cause should be treated at the same time if possible. Infection extending to the inguinal canal (but not the spermatic cord itself) includes extension of the infection from the retroperitoneum, intraperitoneal infection or scrotal infection, such as scrotal pyocoele extending to inguinal canal. Infection to the inguinal region can extend even from the infected partial/total hip replacement. A PubMed search found only two cases of true spermatic cord abscesses. One case was a mycotic spermatic cord abscess in a continuous ambulatory peritoneal dialysis patient [1] and another was a spermatic cord abscess with concurrent prostatic abscess involving the seminal vesicle [2]. Both cases were extension (or possible hematogenous spread) of the primary suppurative process inside the body. We present the first case spermatic cord abscess after femoral artery angiography due to bacterial inoculation (no other infective process in the body was detected access). It is not known how many “sticks” were required and whether they were made using ultrasound. A high index of clinical suspicion (previous trauma, infection, injections and minimally invasive access procedures) and imaging modalities are necessary for the preoperative diagnosis of the rare spermatic cord abscess.