
Abstract

A 61-
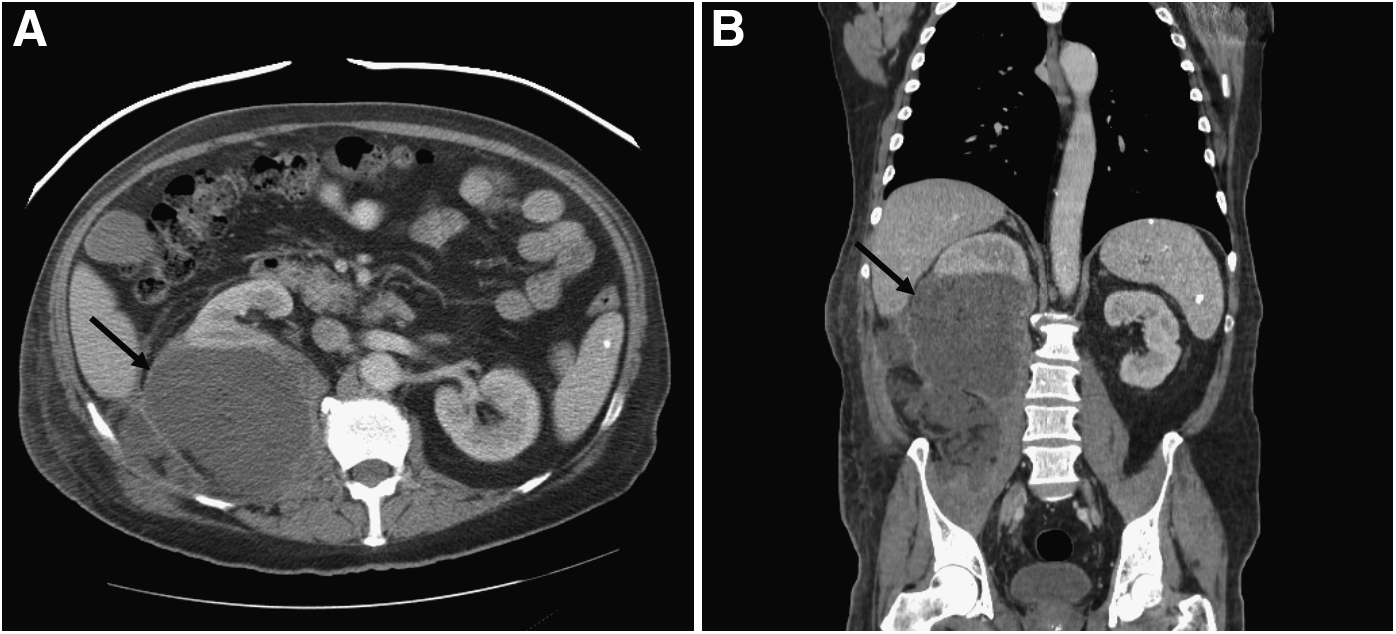
Axial (
Despite continued IV antibiotic and infusions of tissue plasminogen activator into the abscess cavity, repeat imaging demonstrated a persistent multiloculated abscess, measuring 15×9.2×7.6 cm. The patient then underwent laparoscopic-assisted washout and drainage of the abscess cavity. Following a 19-day course of IV ceftriaxone and surgical drainage, the patient was discharged on a 30-day course of oral cephalexin. Subsequent imaging demonstrated resolution of the abscess.
Although recognized commonly as a leading cause of sepsis and meningitis in newborns, GBS, or Streptococcus agalactiae, also has the potential to cause invasive disease in children, pregnant women, elderly patients, and adults with comorbid medical conditions [1,2]. Invasive GBS infection is defined as isolation of GBS from a normally sterile anatomic site [2]. Rarely, invasive GBS infection can result in abscess formation, often from an occult source [2,3]. Although there are reports of GBS abscesses of various retroperitoneal structures [3], a search of the English-language literature did not identify any other cases of a GBS abscess primary to the retroperitoneal cavity.
The pathogenesis of invasive GBS in adults is not understood fully, but is likely multifactorial, and diabetes mellitus is a common risk factor [2,4]. The organism is known to colonize genital and lower gastrointestinal sites, and failure to contain the organism within normal anatomic barriers likely results in invasive infection. Proposed factors contributing to this failure include immune senescence, altered integrity of anatomic barriers, and chronic underlying medical conditions, including diabetes mellitus [4].
The exact etiology of our patient's retroperitoneal abscess remains unclear; however, the patient was found to be a newly diagnosed diabetic with an HbA1C value of 11.7%. Treatment failure with IV antibiotic and percutaneous drainage was attributed to the large, multiloculated nature of the abscess. Laparoscopic-assisted drainage was effective in breaking up the loculations, thus allowing immediate and postoperative drainage of a large volume of pus from the retroperitoneum. Surgical drainage should be considered early in cases of multiloculated invasive GBS abscesses that fail standard treatment with IV antibiotic and percutaneous drainage in order to improve abscess clearance and enhance antibiotic penetration.
Footnotes
Author Disclosure Statement
The authors have no financial disclosures or any conflicts of interest.
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the consent form is available for review on request.