
Abstract
Abstract
Background:
Deep incisional surgical site infection (SSI) is a devastating and costly complication of primary total knee arthroplasty (TKA). The effectiveness of antibiotic-loaded bone cement (ALBC) in preventing these infections remains controversial.
Methods:
A meta-analysis was conducted to assess the efficacy of ALBC in preventing deep infection in primary TKA after a detailed and systematic search of the PubMed, Embase, CNKI, and Cochrane databases had been performed to identify appropriate comparative trials on the prophylactic use of ALBC in primary TKA.
Results:
Five comparative trials were included. In total, 3,461 patients (ALBC group) received ALBC, whereas 3,176 patients (non-antibiotic-loaded cement; NALBC group) did not. The incidence of deep incisional SSI in the ALBC group was 1.32% (n=46) whereas the incidence in the NALBC group was 1.89% (n=60), figures which are not significantly different. No adverse events associated with ALBC were reported in any studies.
Conclusion:
Statistical analysis did not reveal a significantly different incidence of deep or superficial SSI in patients receiving and not receiving antibiotic-loaded cement. The prophylactic application of ALBC thus did not show efficacy in primary TKA. More large-sample studies are required to confirm this finding.
D
How to prevent deep incisional SSI in TKA is always a substantial concern. Some surgeons use antibiotic-loaded bone cement (ALBC) in an attempt to prevent infection However, the efficacy of this measure remains controversial [1,9–12], so a meta-analysis was performed to determine the effect of prophylactic use of ALBC in primary TKA.
Materials and Methods
Identification and Selection of Studies
We performed a literature search using the PubMed (MEDLINE), Embase, and CNKI databases and the Cochrane Central Register of Controlled Trials to identify all articles published between 1966 and 2014 that evaluated the clinical outcome of ALBC use in primary TKA. Comparative studies of primary TKA alone were included; re-operations were not considered. The key terms were “total knee arthroplasty/replacement,” “bone cement,” “antibiotic prophylaxis,” “prosthesis-related infection,” and “antibiotic-loaded bone cement.” A literature search was taken for each author of identified studies to locate other relevant studies. Each study and previous review was examined manually to find further studies on similar topics. As we did not include unpublished research, publication bias could not be avoided.
In consideration of the selection bias, the criteria for inclusion were as follows: English- and Chinese-language papers and neither a history of knee infection nor other knee surgery associated with any of these patients. Although randomized controlled trials (RCTs) may be preferable in meta-analysis, number of such suitable studies was small, so reports were also considered suitable if they described comparative trials between antibiotic-loaded and non-antibiotic cement in primary TKA provided their sample size was more than 100 subjects and their main outcome was the incidence of deep incisional SSI after primary TKA. Infections had to be confirmed by laboratory measures such as the erythrocyte-sedimentation rate, C-reactive protein concentration, radiologic examination, bacterial culture of joint fluid, and signs and symptoms such as purulent drainage from the incision, incisional dehiscence, fever (>38°C), and localized pain or tenderness. Three authors made independent assessments of the quality of the studies before they were accepted for inclusion. After all suitable studies were chosen, data were extracted independently by the three authors.
Data Analysis
Although strict inclusion criteria were used, some aspects of the studies differed, such as the surgical technique, type of implant, and use of systemic antibiotics and their dosages. Therefore, a random-effects model was used for the meta-analysis. All analysis was performed by Review Manager (RevMan) 5.0 (Cochrane Informatics & Knowledge Management, Oxford, U.K.). Relative risk (RR) was used to express the value of antibiotic cement in preventing deep and superficial incisional SSI. The results were shown as forest plots. We used 95% confidence intervals (CI) for each study. In our plots, values <1 indicate ALBC is effective in reducing the rate of infection after primary TKA, whereas values >1 indicate non-antibiotic-loaded bone cement (NALBC) is more effective. In the plots, the statistical significance was set at p<0.05 when the 95% CI did not include 1.0.
Results
A total of 258 potential studies were identified (104 from PubMed, 132 from EmBase, 22 from CNKI, and none from the Cochrane databases). Of these, 185 were excluded on the basis of the titles alone, whereas 50 reports were excluded after review of the abstracts and 18 studies were excluded after detailed review of the full text, leaving five studies for inclusion in this meta-analysis (Fig. 1).

Flow diagram of study selection.
Table 1 summarizes the characteristics of the five studies, which were published between 2001 and 2013. These studies included three RCTs [14–16], one retrospective comparative trial [17], and one prospective comparative trial [18]. A total of 6,637 cases were described in these papers and were included in the final analysis. We compared the incidence of deep incisional SSI in the ALBC and NALBC groups of the patients and also performed a subgroup analysis of the findings in the three RCTs [14–16]. Another analysis was performed of superficial incisional SSIs.
AEC=adverse effect of cement; ALBC=antibiotic-loaded bone cement; DI=deep incisional surgical site infection; DM=diabetes mellitus; MF=mean follow-up (mos); NA=not applicable; NALBC=non-antibiotic-loaded bone cement; NK=Number of knees; PRO=prospective trial; RCT=randomized controlled trial; RE=retrospective trial; SD=standard deviation; SI=superficial infection.
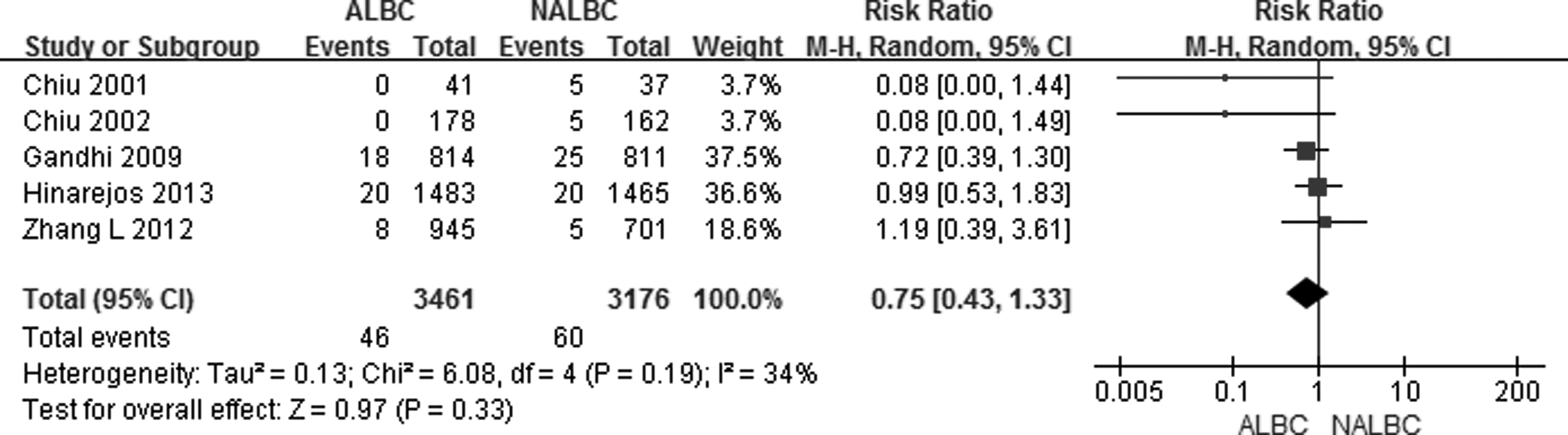
Efficacy in Avoiding Deep Incisional SSI
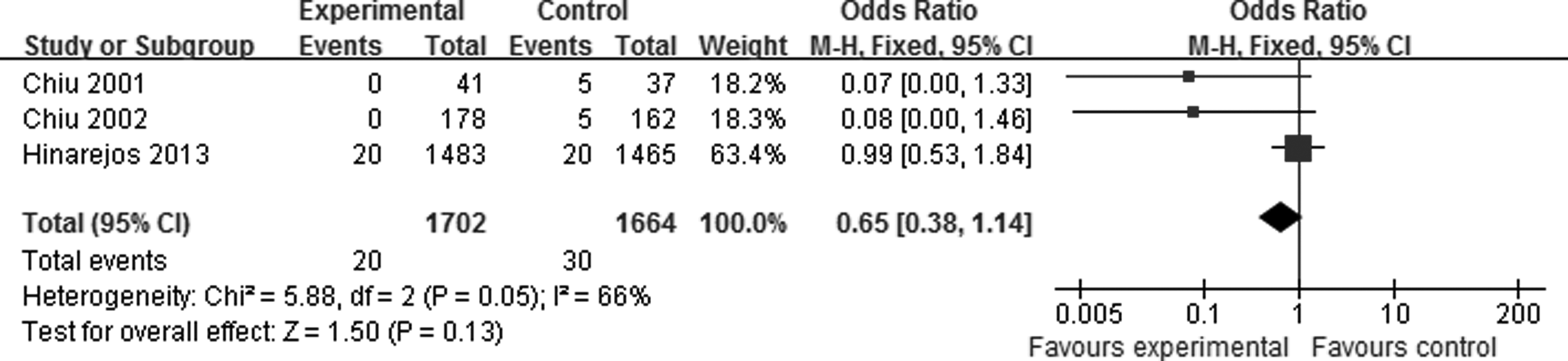
First, we examined the incidence of deep incisional SSI after primary TKA (Fig. 2). Although the overall RR showed no significant difference in the first two studies (Fig. 2), the overall results suggested that prophylactic application of ALBC in primary TKA did not decrease the incidence of deep incisional SSI compared with NALBC (RR=0.75; 95% CI 0.43–1.33; p=0.33; I2=34%; Fig. 2). The results of the subgroup analysis of the RCTs also showed no significant reduction in the incidence of deep incisional SSI with ALBC (RR=0.28; 95% CI 0.04–1.25; P=0.22; I2=65%; Fig. 3).
Forest plot of deep incisional surgical site infection after primary total knee replacement.
Forest plot of incisional surgical site infection after primary total knee replacement. Data from three randomized studies.
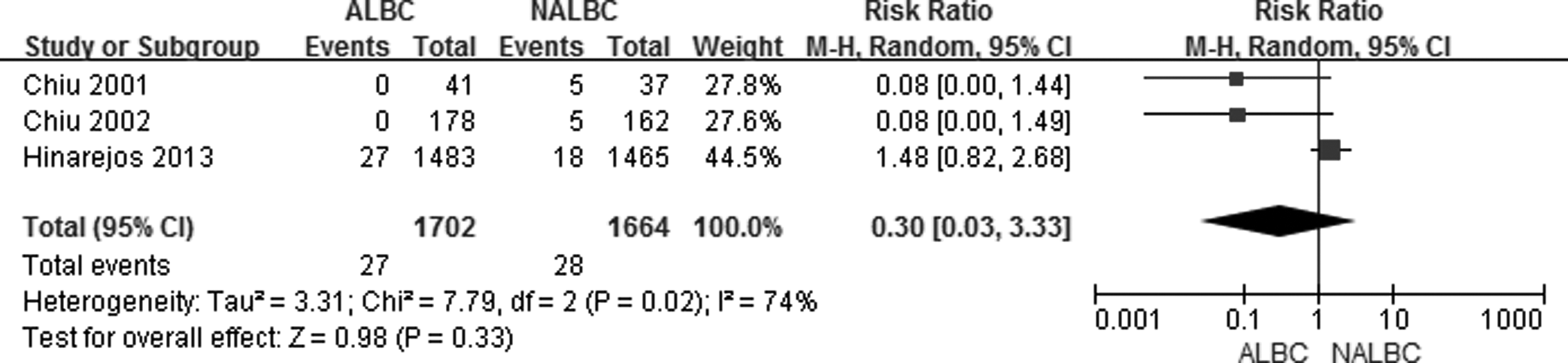
Efficacy in Avoiding Superficial Incisional SSIs
Three studies [14–16] were relevant to the analysis of superficial infection. Prophylactic application of ALBC was not associated with a significant reduction in the incidence of these infections (RR=1.40; 95% CI 0.08–2.43; p=0.24; I2=0; Fig. 4).
Forest plot of superficial incisional surgical site infections after primary total knee replacements.
Discussion
Antibiotic-loaded bone cement has been used in orthopaedic surgery for more than 40 years and has been popular in primary TKA. Indeed, some surgeons regard it as routine in such procedures [7]. Efficacy has been demonstrated in primary total hip arthroplasty and revision procedures [19–22], but it is still unclear whether ALBC is efficacious in primary TKA.
This meta-analysis covered all suitable published papers, including three RCTs [14–16] and two comparative studies [17, 18]. Two small-sample RCTs showed a significant effect of ALBC in preventing deep infection in primary TKA, but the three other studies did not. However, we cannot conclude that ALBC is not efficacious because the difference between the two groups was small and the patients may have been too few for meaningful analysis. A retrospective cohort studied by Namba et al. [13] containing 22,889 cases showed that the results in the NALBC patients were better than those in patients receiving ALBC. However, the difference in the sample sizes in the two groups was large, and the selection bias was substantial, so that paper was not included in this analysis. Bohm et al., in their latest retrospective case-control study [23], showed no significant difference between the groups in the incidence of deep infection. Superficial incisional SSI after primary TKA was examined in three RCTs, and no significant difference was observed.
No adverse event after the application of ALBC was reported in any of the studies we analyzed. For many years, antibiotics such as gentamicin and tobramycin have been the most common antibiotic additives to bone cement [17]. Many papers reported that the proportion of Staphylococcus aureus infections has decreased, but the proportion of coagulase-negative staphylococci causing infection was higher [24–26]. The effectiveness of gentamicin and tobramycin has been reduced greatly in recent years by mutations causing resistance [25], which may be a reason for the lack of efficacy of ALBC. Two in vitro studies suggested that about 8% of the antibiotic in ALBC is released quickly after surgery, and the protracted low-dose release thereafter may cause lack of efficacy and contribute to the problem of antibiotic resistance [27,28].
Some studies have indeed reported the appearance of bacterial resistance after prophylactic use of ALBC in primary TKA. Randelli et al. [29] deemed that prophylactic use of ALBC was a safe tactic, and Sader et al. reported that Sweden, which used ALBC in TKA and THA for many years, had the lowest rates of methicillin-resistant S. aureus and the lowest incidence of carbapenem resistance in the European Union [30]. Hansen et al. likewise reported that no direct evidence suggested that ALBC could lead to resistance [31]. On the other hand, Josefsson et al., through biopsy and bacterial cultures of infection sites, found that 88% of infected patients (30/34) who had received gentamicin-loaded cement in primary joint arthroplasty harbored at least one gentamicin-resistant isolate [32].
Deep incisional SSI after TKA is a costly complication [7]. Jiranek et al. [9] said that every 40 g of ALBC cost USD284–349. However, those authors mentioned that if the incidence of deep incisional SSI was reduced from 1.5% to 0.3% after using ALBC in primary TKA, such use would be cost-neutral. Gutowski et al. [33] also reported that medical costs increase with the use of ALBC.
To our knowledge, this is the first meta-analysis of the efficacy of prophylactic application of antibiotic-loaded bone cement in primary TKA, and there were several shortcomings. The sample size was small, as was the number of RCTs. Inclusion of non-randomized studies increased the heterogeneity of the population. Cement and antibiotic types were not standardized. Finally, some ALBC-related aspects were not scrutinized, such as the potential of ALBC to cause systemic toxicity.
In our meta-analysis, no significant decrease in the infection rate was observed when ALBC was used in primary TKA. Few adverse events were reported, but the cost increased. We conclude that the prophylactic application of ALBC did not demonstrate efficacy in primary TKA. More studies of larger numbers of patients are required to confirm or refute this conclusion.
Author Disclosure Statement
No external funding was provided for this study.