
Abstract
Abstract
Background:
This randomized clinical trial evaluated orally administered trimethoprim-sulfamethoxazole and metronidazole (TSM) in elective colorectal surgery as prophylactic for post-operative surgical site infections (SSI).
Methods:
Patients undergoing elective colorectal resection were evaluated for inclusion. Randomized subjects received either orally administered TSM or intravenously administered cefuroxime and metronidazole (control group, CXM). The primary endpoint was the rate of SSI.
Results:
A total of 1073 subjects were randomized to either control (540) or TSM (533). 486 patients in the TSM group and 499 in the control group were followed-up with after 4 weeks. Thirty-seven (3.8%) patients were afflicted by SSI at discharge from hospital and 69 (7.0%) at follow-up four weeks after surgery. After four weeks, the rate of incisional SSI was 7.0% in the TSM group and 3.6% in the control group (p=0.022). For organ/space SSI and the other complications monitored in the study, no differences were observed between the groups.
Conclusion:
Orally administered TSM as prophylaxis before elective colorectal surgery results in a low rate of organ/space SSI but an increased rate of incisional SSI compared with intravenously administered cefuroxime and metronidazole. Thus, when considering orally administered TSM, because of environmental concerns or for economic reasons, the slightly increased infection rate has to be kept in mind.
T
Thus, since in the beginning of the 1980s, antibiotic prophylaxis in colorectal surgery has been standard treatment and has substantially reduced the post-operative infection rate [3]. Numerous studies have been conducted to find the most effective antibiotic or antibiotic combination, and according to a Cochrane review, an aerobic intravenous antibiotic combined with a non-absorbable oral anaerobic antibiotic is the most effective combination [1]. In spite of this, in Europe the most common infection prophylaxis is exclusively intravenous aerobic and anaerobic antibiotics. The reason for using only systemic antibiotics is a fear of increased frequency of Clostridium difficile infections and post-operative nausea when oral non-absorbable antibiotics are used [4,5]. Further uncertainty exists regarding the efficacy of non-absorbable antibiotics when there is no mechanical bowel cleansing [6]. To be effective, the intravenous combination has to be given pre-operatively within a narrow time frame, a circumstance that may be difficult to accommodate [7,8]. A combination of intravenously administered cefuroxime and metronidazole is an established and well documented regimen for prophylaxis in colorectal surgery and has been the most common prophylaxis in Sweden [2,9]. However, oral absorbable aerobic and anaerobic antibiotics in combination have gained increased popularity and have been used in many Swedish surgical centers in colorectal surgery both with and without bowel preparation for some years. There are advantages with prophylaxis administered orally, regarding costs and timing of administration. However, no large randomized trials comparing intravenous with oral absorbable infection prophylaxis has been published, and we consider it important to study this change of practice in a randomized trial.
The ideal prophylactic antibiotic regime should have an adequate anti-bacterial spectrum, few side effects, minimal negative environmental effect, low cost, and should be used infrequently as treatment of manifest infections. In addition, oral prophylaxis should have rapid and complete absorption and a long half-life. Trimethoprim-sulfamethoxazole and metronidazole (TSM) have many of these properties with a bioavailability of more than 90%, maximum concentration after 2–4 h and 1 h respectively, and a half-life of 10 h and 8 h, respectively. Pharmacokinetic studies of this combination have been performed for prophylaxis in colorectal surgery with good results [10].
In this randomized controlled trial, orally administered TSM is compared with intravenously administered cefuroxime and metronidazole (CXM).
Patients and Methods
Methods
This prospective multicenter single-blind randomized, controlled clinical trial was conducted in seven surgical units in southern Sweden between June 2007 and February 2011. The study protocol was approved by the Ethical Committee at Lund University (Dnr 224/2006) and was registered at ClinicalTrials.gov (registration number NCT00613769). It was also registered at the European Union Drug Regulating authorities (EudraCT number 2006-006575-20). Prior to the study, all local collaborating staff attended information meetings to ensure uniformity of practice and adherence to the protocol. Local investigators were responsible for consecutively identifying eligible patients, recruitment, obtaining consent, and data collection. An independent monitor visited each center on a regular basis to validate the Case Report Forms with the individual patient journals.
Patients
The study comprised patients undergoing elective clean-contaminated colorectal resection. Written informed consent was obtained from all patients included. The trial was registered in each patient's medical record. In accordance to EMEAS guidance on statistical principles for clinical trials, criteria for exclusion from the study after inclusion were: Additional abdominal surgery or other surgery with antibiotic prophylaxis within four weeks after the primary surgery (except re-operation because of deep infection), if the skin incision was not closed at the elective surgery, abdominal contamination was present before surgery but diagnosed during the operation, e.g., finding of abscess or perforation that existed prior to surgery [11]. All subjects had to be 18 years or older and understand spoken and written Swedish. Exclusion criteria are listed in Table 1.
According to the protocol, excluded patients and dropouts were not replaced. Patients who declined to participate in the study or did not meet inclusion criteria were recorded and the cause was identified in a screening log.
Randomization
A computerized block randomization was performed for each unit at the principal investigation center. The CRF 2 (treatment or control group) was selected according to the randomization and sent to each surgical unit in sealed envelopes. At the surgical units the envelopes were used in numerical order and the randomization procedure was performed by a nurse on the day of surgery.
Intervention
Patients were randomized to oral, TSM (treatment group), or intravenous, CXM (control group), antibiotic prophylaxis pre-operatively. All drugs administered to the patients were acquired from the hospital's medical storage. The trial medication was given by the nurses on the ward. This way the attending physician was blinded.
Study drug (TSM)
One tablet of sulfamethoxazole 800 mg in combination with trimethoprim 160 mg, and three tablets of metronidazole 400 mg were administered orally to the patient minimum 2 h prior to start of surgery. The tablets were administered at 06:30 with scheduled surgery start between 08:30 and 13:00 and expected to be completed by 17:00. If the operation was planned to start after 13:00 or expected to be completed after 17:00 the tablets were given at 11:00.
Control group drug (CXM)
An intravenous injection of cefuroxime 1.5 g and intravenous infusion of metronidazole 1.5 g were administered to the patient simultaneously with the induction of anesthesia, which in practice means at least 30 min before skin incision and before the surgeons' arrival [7,8,9].
Apart from the antibiotic prophylaxis, all preparations, surgical aspects, and post-operative care were conducted according to the standard procedures established in the participating hospitals.
Blinding
The surgeon and other investigators assessing the outcome parameters were blinded throughout the evaluation period as to which group each patient was assigned. Medical records only revealed the involvement in the study and concealed information of the specific antibiotic treatment. The medical staff with knowledge of the treatment as well as the patients were told not to reveal to which group a patient was assigned.
Outcome variables
The occurrence of surgical site infections (SSI) was classified according to U.S. Centers for Disease Control and Prevention (CDC) definitions [12]. However, in this study, for simplicity, superficial and deep incisional surgical site infections were classified as incisional surgical site infections.
Patients were assessed daily during their stay in hospital up to the first 28 d post-operatively. The presence of SSI, other infectious complications, non-infectious surgical site complications, and use of antibiotics were registered. Of the incisional SSIs, only incisions on the abdominal wall were included in the trial report.
All patients discharged from hospital within 28 d of surgery received a follow-up questionnaire with questions regarding outcomes. If post-operative infectious complications, such as problems with the incision, were suspected, the patients were instructed to contact health care for examination. Signs of SSI at the time of suture removal were registered specifically. Regardless of whether or not there were complications, the questionnaire was to be completed and returned by the patient 4 wks after the operation. If no response was received, after an additional 3 wks, a second letter was sent to the patient. If required, a third letter was sent. Most patients were also observed in the outpatient clinic for follow-up after surgery.
All outcomes were based on the presence of infections or other complications up to 4 wks after surgery. The primary outcome was the incidence of SSI within 28 d after surgery. Secondary outcomes were other post-operative infections, e.g., sepsis, pneumonia, urinary tract infection, the incidence of surgical site complications not caused by infection, anastomosis insufficiency, and additional antibiotics administered excluding the first prophylactic dose. Other variables were number of post-operative hospital days and follow-up visits to the district nurse after discharge.
Statistical analysis
On the basis of the available data that infection rate after elective colorectal surgery is ≤ than 10%, a sample size of 2160 patients would be necessary (80% power, α=0.05) to detect a difference in infection rate of 4% between the groups.
Continuous data are presented as mean (95% confidence intervals) and were compared with t-test. Categorical variables were compared using the Fisher exact test. The McNemar test was used to compare paired proportions. All statistical tests were two-sided and P≤0.05 was considered significant. Statistical support was provided by RSKC, Lund, Sweden.
Results
Enrollment was slower than planned and the fraction of patients excluded from the study was larger than expected. Thus, the number of subjects included in the study did not reach the planned number. Assuming the same effect as in the present study, full inclusion, according to the study plan would have decreased the statistical error margin from 3 to 2 percentage points. Eighty-eight subjects were excluded after inclusion in accordance to EMEAS guidance on statistical principles for clinical trials as declared previously [11]. For 13 of these patients, the exact reason for exclusion was not properly recorded in the CRF. Patient characteristics are summarized in Table 2. There were no substantial differences between the two groups in age, gender, or type of surgery performed. Of the 1073 patients randomized, 88 were excluded after inclusion. All remaining patients, 499 in the study group and 486 in the control group, were clinically evaluated after the study (Fig. 1).
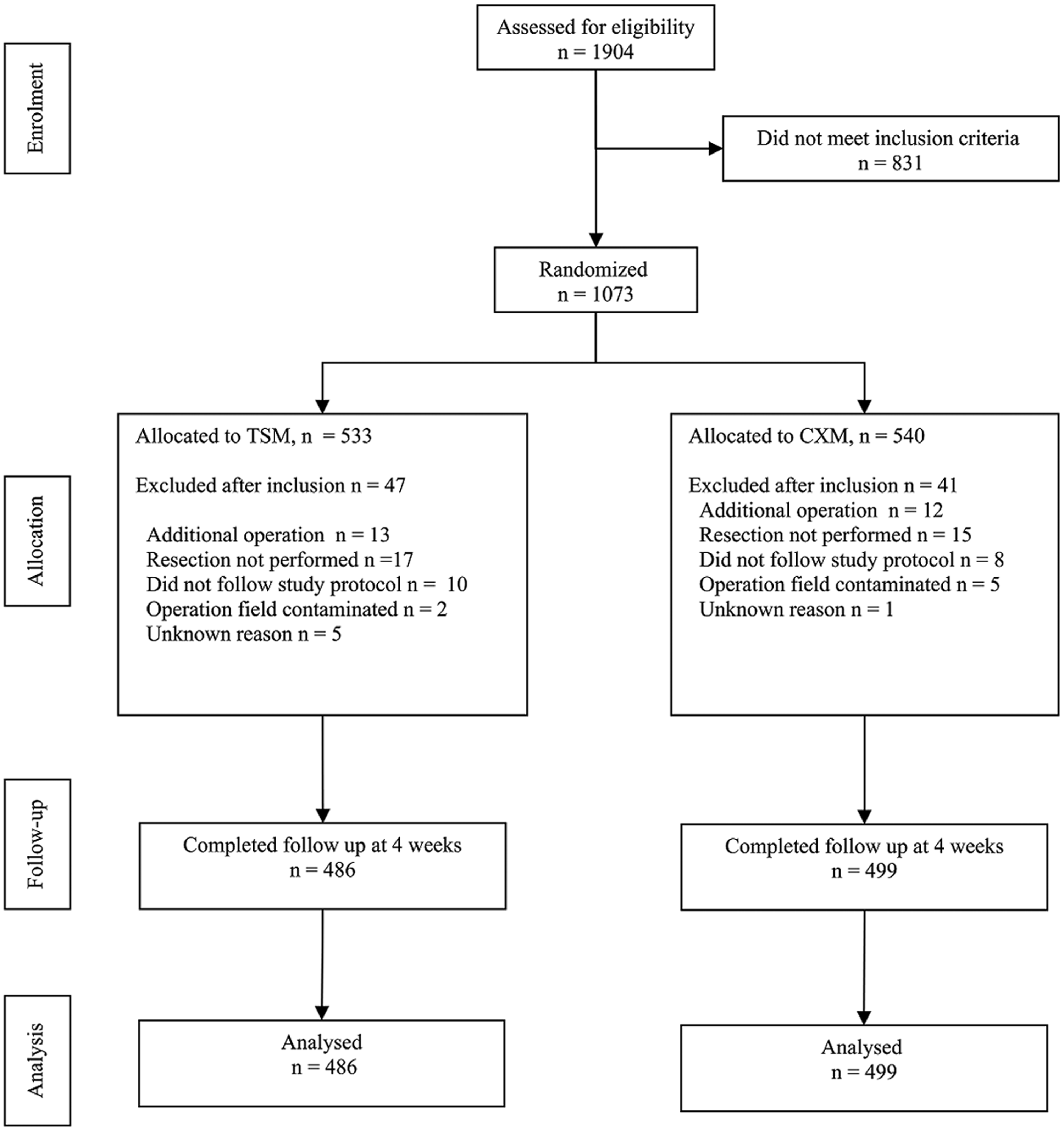
CONSORT diagram for the trial.
Values are mean (95% confidence intervals), unpaired t-test.
# Number (%), Fisher exact test.
TXM=trimethoprim sulfamethoxazole; IRA =ileorectal anastomosis.
Thirty-seven (3.8%) patients had SSI at the time of hospital discharge and 69 (7.0%) at follow-up 4 wks after surgery (Table 3). Of the 46 patients with surgical site complications without suspicion of SSI at discharge from hospital, 12 had developed incisional SSI and none organ/space SSI at follow-up 28 d after surgery. The incidence of post-operative SSI varied between the types of surgical procedure performed (Table 4).
McNemar test.
SSI=Surgical site incision.
TSM and control group values are compared with McNemar test.
SSI=surgical site infection.
The TSM group had a substantially greater rate (7.0%) of incisional SSI compared with the control group (3.6%). No difference was observed for organ/space SSI (Table 5).
Values are mean (95% confidence intervals), unpaired t-test
# Fisher exact test
SSI=surgical site infection.
Four patients (0.8%) in the TSM group and 12 patients (2.4%) in the control group developed surgical site dehiscence during the study period, but this complication was observed only in one of the 69 patients (1.4%) with SSI within 4 wks post-operatively. The rate of anastomotic leakage was 3.4% respectively 3.5% in the two groups (Table 5).
There were no differences between the groups in the total number of days with treatment of antibiotics during hospital stay, rate of septicaemia, urinary tract infection or pneumonia, post-operative hospital duration or the number of contacts with health care after discharge because of SSI within the study period (Table 5).
The study was not designed to compare costs of the two regimens. The monetary value of drugs and equipment is listed in Table 6.
Cost for staff nurse excluded.
All costs were calculated in SEK and converted to USD by taking the exchange rate in April 2014 (1 USD=6.48 SEK) [19].
Cost for staff nurse excluded.
All costs were calculated in SEK and converted to USD by taking the exchange rate in April 2014 (1 USD=6.48 SEK) [19].
Discussion
The most effective antibiotic prophylaxis in colorectal surgery according to a Cochrane review is a combination of intravenous peri-operative antibiotics and oral non-absorbable antibiotics [1]. This combination is commonly used in the United States. However, in Sweden (and Europe), often only peri-operative systemic antibiotics are used. The arguments against oral non-absorbable antibiotics are uncertainty regarding effect on unprepared bowel and the increased risk for Clostridium difficile infection. Because this study was conducted in Sweden, we decided to study locally practiced regimes. In this study, we found a low rate of SSI; however, we detected a substantially increased risk of incisional SSI for the peroral (TSM) treatment compared with the intravenously administered (CXM) alternative, the latter which is well documented as prophylaxis. Regarding organ/space SSI, the rate was low and there was no difference between the groups. The study was completed within the planned time frame.
However, the number of patients planned to be included was not reached because of a lower inclusion rate. The fraction of excluded patients from the study was also larger than expected. The most common reason for exclusion in the group of 831 patients was pre-operative radiation therapy in patients with rectal cancer. Unfortunately patients had been recorded as excluded during periods when inclusion was not performed because of absence of the local investigator. Thus, some small differences between the groups may be overseen. Also, the original power calculation was based on detecting a difference in SSI of 4% from a rate of 10% in the control group. In this study the rate of SSI in the control group was 5.4%.
When considering type of antibiotics to be used as prophylaxis, other factors such as ecological adverse effects—often associated with the use of cephalosporins and quinolones—have to be taken into account [13]. The difference in rate of incisional SSI between the groups seems to be most marked for colectomies with ileorectal anastomosis. Probably the patients' diagnosis is of less importance compared with body mass index (BMI), duration of surgery, per-operative estimated blood loss, and procedure performed [14]. A pharmacokinetic study supports the idea that perorally administered TSM gives satisfactory serum concentrations when used in conjunction with elective colorectal surgery [9]. On the other hand, in elective upper gastrointestinal surgery when this regimen was used in patients with malignant disease of the liver, biliary tract, or pancreas, only 37% of the patients were found to have adequate serum concentrations despite presumed normal gastrointestinal function [15]. Unfortunately we have no data on BMI or serum concentrations in this study to explain the difference in incisional SSI in the treatment arm. The low incidence of organ/space SSI has been observed in earlier studies of antibiotic prophylaxis in elective colorectal surgery as well as in surgery of non-perforated appendicitis [16,17]. These results could be interpreted as that the effect of infection prophylaxis with antibiotics or differences in effect of different antibiotics is hard to demonstrate on organ/space SSI, either because of the low rate or because of low effect of antibiotics on this type of SSI. However, differences between treatments are detected when incisional SSI is monitored. This makes the level of incisional SSI a suitable end point, in colorectal surgery, for an estimate of effects of different antibiotic prophylaxis regimens in studies as well when monitoring the level of SSI in the clinical routine.
When comparing different studies, there is great variation in the rate of SSI after colorectal surgery. This is explained partly by different ways of defining SSI, different periods of follow-up and whether or not the surgical site infection rate included perineal infections [2].
We found that approximately 50% of the incisional SSIs were detected until discharge from the hospital compared with 4 wks after surgery. Thus, registration after the patients are discharged from hospital is necessary; this has also been shown in earlier trials [18]. The cost of the study drugs is less than 10% of the intravenous alternative used in this study. However, the monetary gain alone could not justify using the TSM regimen.
In conclusion, orally administered TSM gives as low a rate of organ/space SSI as intravenous prophylaxis in this study, but an increased rate of incisional SSI. When choosing type of antibiotic prophylaxis in colorectal surgery, the increased risk of incisional SSI should be weighed against other factors such as cost and environmental factors.
When considering perorally administered TSM as a prophylactic regime in elective colorectal surgery the increased infection rate has to be kept in mind.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest.
Acknowledgments
This study was funded by the Scientific Advisory Board, Halland Region, Sweden, the Southern Regional Health Committee, Sweden and the Research Fund at Skaraborg Hospital, Sweden.