
Abstract
Abstract
Background:
Enterobacteriaceae (3,235 isolates), Pseudomonas aeruginosa (476 isolates), and Acinetobacter baumannii (106 isolates) from inpatient intra-abdominal infections (IAIs) were collected for the 2010–2012 Study for Monitoring Antimicrobial Resistance Trends (SMART) program in the United States. This report evaluates the in vitro activity of several antimicrobial agents recommended for treatment of IAIs and compares profiles of isolates from intensive care units (ICUs) and non-intensive care units (non-ICUs).
Methods:
Gram-negative bacilli from hospitalized patients with IAIs were obtained each year from 2010–2012 from hospitals in the United States and tested for susceptibility to 12 antibiotics according to 2012 Clinical and Laboratory Standards Institute (CLSI) guidelines.
Results:
The most active agents against members of the Enterobacteriaceae family from both ICUs and non-ICUs were amikacin, ertapenem, and imipenem-cilastatin, whereas the least active agent was ampicillin-sulbactam. Amikacin was the only agent with good activity against P. aeruginosa, whereas none of the agents tested exhibited substantial activity against A. baumannii. Amikacin, ceftazidime, ceftriaxone, ciprofloxacin, levofloxacin, and imipenem-cilastatin were significantly less active against Enterobacteriaceae from ICU patients, whereas cefepime and ceftazidime were significantly less active against P. aeruginosa from ICU patients. Intensive care unit isolates were more likely to be multi-drug–resistant than non-ICU isolates, although there was no difference in extended-spectrum β-lactamase (ESBL) production rates between the two patient groups.
Conclusions:
Despite increasing resistance trends, in this study amikacin, ertapenem, and imipenem-cilastatin were shown to have good in vitro activity against the most frequently isolated gram-negative bacilli from IAIs in ICU and non-ICU settings.
I
Antimicrobial–resistant gram-negative bacilli of concern include oxyimino-cephalosporin–resistant members of the Enterobacteriaceae family producing extended-spectrum β-lactamases (ESBLs) or AmpC β-lactamases [9–11]. Reliance on carbapenems to treat these pathogens has led to an increase in carbapenem resistance associated with the production of carbapenemases or a decrease in outer membrane permeability [12,13].
Pseudomonas aeruginosa and Acinetobacter baumannii are opportunistic pathogens that are resistant, either intrinsically or by acquired genetic elements, to antimicrobial agents from several classes. Although not often described as normal microbial flora in healthy individuals, P. aeruginosa and A. baumannii are of concern for hospitalized patients. Critically ill patients in intensive care units (ICUs), including those who have undergone invasive intra-abdominal surgical procedures, are at high risk for developing infections due to these organisms [14,15].
The global increase and spread of antimicrobial resistance in bacteria causing both hospital- and community-associated infections, as well as the dissemination of mobile genetic determinants for resistance between species, is well documented [16–18], with serious implications for both patient populations. However, this is especially relevant for patients hospitalized in ICUs. Delayed diagnosis and inadequate treatment of infections caused by MDR bacteria has been associated with increased rates of clinical failure, mortality, and cost [19,20], with ICU admission identified as a risk factor for infections with ESBL-producing pathogens [21]. A number of surveillance programs monitor resistance rates and have been essential in tracking the escalation of both community- and hospital-associated antimicrobial resistance. The Study for Monitoring Antimicrobial Resistance Trends (SMART) program is a global surveillance program that has monitored the susceptibility of aerobic and facultative gram-negative bacilli from patients with IAIs since 2002 and urinary tract infections (UTIs) since late 2009. This report summarizes susceptibility trends from IAIs in non-ICU and ICU settings in the United States from 2010 through 2012.
Patients and Methods
Up to 100 gram-negative bacilli from hospitalized patients with IAIs were obtained each year from 2010–2012 from each participating hospital in the United States. The number of institutions contributing isolates totaled 19 in 2010, 20 in 2011, and 18 in 2012. Sixteen hospitals participated in all 3 y of the study, four participated in 2 y, and one participated once. Each study site was requested to submit consecutively isolated, clinically important, and non-selected unique gram-negative bacilli from inpatients with IAIs. Isolates were identified to the species level at each participating site and submitted to the central reference study center (Laboratories International for Microbiology Studies, a subsidiary of International Health Management Associates, Inc., Schaumburg, IL) for identification confirmation and susceptibility testing.
Minimum inhibitory concentration values (MICs) for amikacin, ampicillin-sulbactam, cefepime, cefotaxime, cefoxitin, ceftazidime, ceftriaxone, ciprofloxacin, ertapenem, imipenem-cilastatin, levofloxacin, and piperacillin-tazobactam were determined at the central reference study center using manually read MicroScan® custom-manufactured dehydrated microdilution panels (Siemens Medical Solutions Diagnostics, West Sacramento, CA), using the Clinical and Laboratory Standards Institute (CLSI) testing guidelines and interpretive criteria [22,23]. Multi-drug resistance was defined as resistance to three or more antimicrobial classes.
Isolates were classified as ESBL-producers when there was at least an eight-fold reduction of the MICs for ceftazidime or cefotaxime tested in combination with clavulanic acid compared with the MICs when tested alone [23]. Quality control was performed on each day of testing using the CLSI recommended quality control strains: Escherichia coli ATCC 25922, E. coli ATCC 35218, P. aeruginosa ATCC 27853, and Klebsiella pneumoniae ATCC 700603 (positive ESBL control, American Type Culture Collection, Rockville, MD). Results were included in the data analysis only when corresponding quality control values were within the acceptable range as specified by CLSI [23].
Statistical analysis
Differences in susceptibility percentages, ESBL rates, and MDR rates were evaluated for statistical significance using the Fisher exact test, two-tailed. A p value of <0.05 was deemed significant. Analysis was run using XLSTAT 2011.1.05 software (Addinsoft, Paris, France).
Results
In 2010–2012 3,888 gram-negative bacilli were collected from inpatient IAI sources in the United States, including 3,235 (83.2%) Enterobacteriaceae, 476 (12.2%) P. aeruginosa, and 106 (2.7%) A. baumannii. Seventy-one (1.8%) consisted of other genera and species. Overall, 809 isolates came from patients in ICUs (surgical, medical, pediatric, or unspecified), and 3,079 came from non-ICUs (general medicine, pediatric, or surgical units). Table 1 illustrates the MIC50, MIC90, and percents susceptible, intermediate, and resistant for all Enterobacteriaceae, P. aeruginosa, and A. baumannii versus amikacin, ampicillin-sulbactam, cefepime, cefotaxime, cefoxitin, ceftazidime, ceftriaxone, ciprofloxacin, ertapenem, imipenem-cilastatin, levofloxacin, and piperacillin-tazobactam for the years 2010 to 2012. Based on a percent susceptible of ≥90%, amikacin, ertapenem, cefepime, imipenem-cilastatin, and piperacillin-tazobactam were the most effective agents in vivo against members of the Enterobacteriaceae from non-ICU locations. Only amikacin, ertapenem and cefepime were effective in vivo against Enterobacteriaceae from ICUs. Ampicillin-sulbactam was the least effective antimicrobial against isolates from all locations. Amikacin, cefotaxime, ceftazidime, ceftriaxone, ciprofloxacin, levofloxacin, and imipenem-cilastatin were all significantly less active against Enterobacteriaceae isolates from ICU patients (p<0.05).
Values≥90% susceptible are shaded; values that are significantly lower in ICUs than non-ICUs are in bold (p<0.05).
MIC50=minimum inhibitory concentration required to inhibit the growth of 50% of organisms; MIC90=minimum inhibitory concentration required to inhibit the growth of 90% of organisms; AMK=amikacin; SAM=ampicillin-sulbactam; FEP=cefepime; CXT=cefotaxime; FOX=cefoxitin; CAZ=ceftazidime; CRO=ceftriaxone; CIP=ciprofloxacin; ERT=ertapenem; IPM=imipenem-cilastatin; LVX=levofloxacin; TZP=piperacillin-tazobactam; na=breakpoint not defined.
Of the agents with CLSI breakpoints tested in this study, none exhibited good activity against A. baumannii. The most active antimicrobial was imipenem-cilastatin with 70% of non-ICU isolates susceptible. The percentage susceptible to amikacin was significantly greater in non-ICU isolates compared to ICU isolates (p=0.0335), whereas there were no significant differences between susceptibilities of ICU and non-ICU isolates of this species to the other antimicrobials tested (p>0.05).
Amikacin was the only compound with good activity against P. aeruginosa from both ICU and non-ICU isolates with susceptibility percentages of 97% and 96%, respectively. Ceftazidime and piperacillin-tazobactam inhibited 82% and 81%, respectively, of non-ICU isolates. All other compounds inhibited≤78% of all isolates. Ceftazidime and cefepime were significantly less active against isolates from ICU patients (73% and 68%, respectively) than non-ICU patients (82% and 78%, respectively).
Table 2 compares the susceptibility of the 10 most frequent pathogens from ICUs and non-ICUs. Amikacin was the most active compound for all species, although activity was low against all A. baumannii (39% ICU, 64% non-ICU), and was reduced against ESBL-positive E. coli from ICU patients (83%) and all ESBL-positive K. pneumoniae (67% ICU, 48% non-ICU). Ciprofloxacin and levofloxacin showed good activity against Enterobacter spp., K. oxytoca, and Serratia marcescens, with percent susceptible ranging from 92%–100% for ICU isolates and 83%–99% for non-ICU isolates. The quinolones were significantly less active against ICU isolates of the most commonly isolated species, E. coli, with 64% and 66% susceptible to ciprofloxacin and levofloxacin, respectively, versus 73% for each among non-ICU isolates. ESBL-positive isolates of K. pneumoniae displayed reduced susceptibilities to all agents tested, with the carbapenems showing the greatest activity with susceptibility to ertapenem and imipenem-cilastatin of 63% and 67%, respectively, in non-ICU isolates, and 71% for both in ICU isolates. The carbapenems retained better activity against ESBL-positive E. coli from both ICU and non-ICU isolates, with susceptibility to ertapenem at 92% and 97%, and imipenem-cilastatin 96% and 99%, respectively. Of all the other compounds tested, only amikacin and piperacillin-tazobactam showed activity>80% against ESBL-positive E. coli, while no antimicrobials other than the carbapenems displayed activity of >67% against ESBL-positive K. pneumoniae.
Values≥90% susceptible are shaded; values that are significantly lower in ICUs than non-ICUs are in bold (p<0.05).
ICU=intensive care uni; AMK=amikacin; SAM=ampicillin-sulbactam; FEP=cefepime; CXT=cefotaxime; FOX=cefoxitin; CAZ=ceftazidime; CRO=ceftriaxone; CIP=ciprofloxacin; ERT=ertapenem; IPM=imipenem-cilastatin; LVX=levofloxacin; TZP=piperacillin-tazobactam; ESBL=extended-spectrum β-lactamase; na=breakpoint not defined.
In evaluating all Enterobacteriaceae combined, ICU isolates were significantly less susceptible than non-ICU isolates to amikacin, ceftazidime, ceftriaxone, ciprofloxacin, levofloxacin and imipenem-cilastatin (p<0.05). There were no significant differences in susceptibility between ICU and non-ICU isolates for most antimicrobials when stratified by individual species, with the exceptions of reduced susceptibilities in ICU isolates to amikacin, ciprofloxacin, and levofloxacin against all E. coli and non-ESBL E. coli, cefepime and ceftazidime against P. aeruginosa, and cefepime against Citrobacter freundii. Susceptibility to cefotaxime was significantly higher against non-ESBL E. coli from ICU patients (98%) versus non-ICU patients (97%), although the susceptibilities differed by only one percentage point.
Table 3 shows the percentage of isolates exhibiting multidrug resistance based on resistance to 2, 3, and ≥4 classes of antimicrobials. For all gram-negative isolates combined, ICU isolates were significantly more likely to be MDR than non-ICU isolates at all three levels of resistance, with percentages of 29.5, 11.0, and 5.6 for ICU isolates resistant to one, two, or three classes versus 23.3, 8.5, and 3.7 for non-ICU isolates (p<0.05 for each combination). When separated by genus, Enterobacteriaceae and P. aeruginosa isolates from ICU patients were significantly more likely to be resistant to two antimicrobial classes than isolates from non-ICU patients (p<0.05), whereas A. baumannii from ICU patients were highly significantly more likely to be resistant to ≥4 classes (p=0.0017).
Percent resistant values that are significantly higher in ICU patients than non-ICU patients are bolded (p<0.05).
ICU=intensive care unit.
The ESBL-positive rates for E. coli and K. pneumoniae are shown in Figure 1. The rates of 8.5% (ICU) and 6.4% (non-ICU) for E. coli were lower than the 15.2% (ICU) and 12.1% (non-ICU) rates of K. pneumoniae, however, there were no significant differences between ESBL rates in the ICU and non-ICU isolates (p>0.05).
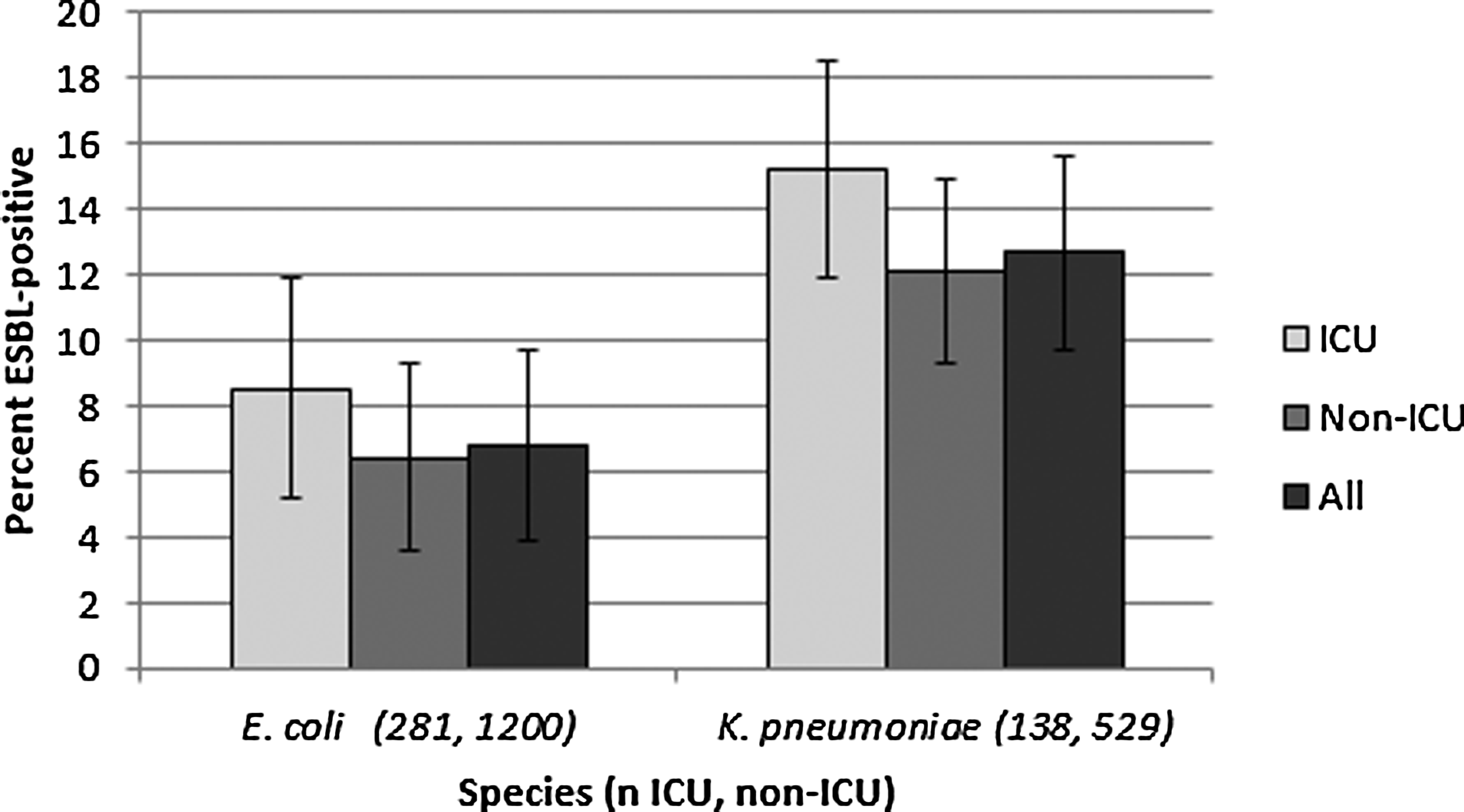
Percentage of extended-spectrum β-lactamase (ESBL)-positive Escherichia coli and Klebsiella pneumoniae from intensive care unit (ICU) and non-ICU patients in the United States, 2010–2012, with 95% confidence intervals.
Extended-spectrum β-lactamase-positive E. coli from both ICU and non-ICU patients were significantly more likely to be non-susceptible to ertapenem (p≤0.05) than ESBL-negative isolates, while ESBL-positive K. pneumoniae from both ICU and non-ICU patients were more likely to be non-susceptible to both imipenem-cilastatin and ertapenem than ESBL-negative isolates (p≤0.05; Table 2).
Discussion
Antimicrobial resistance is a well-documented concern for clinicians treating all patients, but the challenge is compounded in ICU patients with IAIs. The selection of effective antimicrobial therapy is essential, because initially ineffective empiric therapy is associated with complications and increased length of hospital stay [24]. The increasing resistance to broad-spectrum cephalosporins due to ESBLs in Enterobacteriaceae has left few choices for treatment, with carbapenems often the only active β-lactams against these bacteria. This has led to their increased use both against documented infections and for empiric treatment, with the opportunity for greater selection for carbapenem resistance, as well as resistance to other antibiotics as carbapenemase-producing strains are likely to exhibit simultaneous resistance to fluoroquinolones and aminoglycosides [25]. Recent studies have documented the increased prevalence of MDR isolates when carbapenem use is unrestricted, particularly A. baumannii and P. aeruginosa, with highly resistant clonal strains spreading rapidly [26,27]. The SMART program has examined antimicrobial susceptibility in IAI pathogens globally since 2002, and provides specific data for the United States. The current analysis confirms decreased activity of amikacin, ceftazidime, ceftriaxone, ciprofloxacin, levofloxacin, and imipenem-cilastatin against all Enterobacteriaceae from ICU patients. Of the antimicrobials included in this analysis, only amikacin has retained good activity against P. aeruginosa in the United States, with 96% and 97% susceptible from non-ICU and ICU isolates, respectively. This compares favorably with 92% and 93% amikacin susceptible P. aeruginosa reported from 1998–2001 non-ICU and ICU isolates [14]. There were significant differences in susceptibility of P. aeruginosa to the cephalosporins cefepime and ceftazidime between ICU and non-ICU isolates, although as the differences are small, the clinical importance is unclear. Induction of chromosomally encoded β-lactamases (AmpC genes) by previous exposure to β-lactam antibiotics causes enzymatic inactivation of many β-lactams, including ceftazidime and, to a lesser extent, cefepime [28].
Isolates of A. baumannii exhibited reduced susceptibility to all compounds evaluated in this study, and were considerably less susceptible than isolates evaluated in a 2003 study [14]. Most notably, amikacin susceptibilities for non-ICU and ICU decreased from 75.8% and 84.5% to 64% and 39%, respectively, whereas imipenem-cilastatin susceptibilities were reduced from 93.4% and 96.2% to 70% and 44%. In this study, isolates from ICUs were significantly less susceptible to amikacin than non-ICU isolates (p=0.0335). Differences in percent susceptible between non-ICU and ICU isolates for imipenem-cilastatin were not quite significant (p=0.0537). The incidence of ESBL-positive E. coli isolates from IAI patients in the United States has increased slightly in all hospital units, with 4.6% reported as ESBL-positive in an analysis of 2007–2008 SMART data [29] compared to 6.8% for all E. coli in 2010–2012. ESBL-positive rates for K. pneumoniae have actually decreased from 17.5% in 2007–2008 to 12.7% in 2010–2012. Whereas regional differences in the prevalence of ESBLs in the United States and varying sample numbers from sites from year to year make this observation difficult to interpret, the SMART program has documented a general flattening of ESBL rates globally [29]. An analysis of pediatric ICU isolates from 2008–2010 showed ESBL rates in North America of 4% and 25% for E. coli and K. pneumoniae, respectively [30]. Whereas there was no significant difference in the ESBL rates for ICU isolates and non-ICU isolates, ESBL-positive isolates were associated with lower susceptibilities to fluoroquinolones and carbapenems. Carbapenem resistance can result from selective loss of outer membrane permeability, the combination of impermeability with various ESBLs or cephalosporinases, or the production of carbapenemases [17]. Although this analysis does not include molecular characterization of resistant isolates, it is highly likely that the reduced susceptibility levels of ESBL-positive K. pneumoniae reported in this study are due to carbapenemase-producing (KPC) isolates, as ESBLs alone do not confer resistance to carbapenems, and resistance due to outer membrane permeability or the combination of ESBLs plus AmpCs is relatively rare. Multi-drug resistance based on resistance to two, three, or four classes of antimicrobials was significantly more prevalent in ICU isolates as compared to non-ICU isolates as has been reported previously [6,9,14]. Prescribing carbapenems empirically before bacterial culture and susceptibility results are available in patients with polymicrobial IAIs may increase the likelihood of the development of resistance to these agents [5,24].
National, regional, and local surveillance programs are essential for providing clinicians with the necessary information for choosing empiric and directed therapy. This analysis from the SMART program provides epidemiologic trends in resistance profiles for the most commonly isolated gram-negative pathogens from IAIs. Despite increasing resistance trends, in this study, amikacin, ertapenem, and imipenem-cilastatin were shown to have good in vitro activity against the most frequently isolated gram-negative bacilli from IAIs in ICU and non-ICU settings.
Footnotes
Acknowledgments
The authors thank all SMART investigators for their years of valuable contribution to this program, and Sibylle Lob for the statistical analysis for this manuscript.
Author Disclosure Statement
All authors are employed by IHMA, Inc., which receives funding from Merck & Co., Inc., to conduct and manage the SMART program. None of the authors declare a conflict of interest associated with the production of this article.