
Abstract
Abstract
Background:
Sepsis is among the leading causes of death in the United States, and patients undergoing surgical procedures are at greater risk for infectious complications. The incidence of sepsis and its association with outcomes among patients undergoing surgical procedures in various specialties were investigated. Additionally, the infectious sources and associated primary procedures were reported for sepsis-related deaths.
Methods:
Patients undergoing procedures performed by surgical services at our academic medical center between January 2010 and June 2013 were reviewed. Sepsis was identified by the assignment of related ICD-9-CM billing codes. Patient outcomes included hospital length of stay, intensive care unit (ICU) admission, ICU length of stay, and death. A subset of sepsis-related deaths was reviewed further for infectious sources and primary procedure codes.
Results:
A total of 25,522 patients underwent a procedure by a surgical service, and sepsis developed in 863 patients (3.38%) during their hospital stays. Overall, patients with sepsis had significantly longer hospital and ICU stays, greater likelihood of ICU admission, and a higher mortality rate. The incidence of sepsis was highest in patients with procedures performed by cardiothoracic surgery (8.39%), trauma/acute care surgery (7.55%), and plastic/reconstructive surgery (5.35%). Sepsis was associated with a significant increase in the mortality rate among vascular surgery, trauma/acute care surgery, and cardiothoracic surgery patients. The most common infectious sources in sepsis-related deaths were pulmonary infections (39.5%), blood stream infections (35.1%), and gastrointestinal infections (31.6%). The procedures associated with the greatest number of sepsis-related deaths were extracorporeal membrane oxygenation, small bowel resection, and insertion of implantable heart-assist systems.
Conclusions:
Sepsis is not an uncommon condition and is associated with longer hospital and ICU stays, greater likelihood of ICU admission, and a higher mortality rate. Accurate benchmarking of sepsis is essential for the development and monitoring of sepsis-reduction quality-improvement initiatives.
T
Several factors make surgical patients different from medical patients: The relative health of those presenting for elective surgery, the invasiveness of surgery that predisposes to iatrogenic and hospital-acquired infections, and the relative post-operative immunologic vulnerability. Although the incidence of sepsis among medical and surgical patients as a whole has been reported, there is limited literature on the differential incidence and impact of sepsis among the various surgical specialties. Currently, the Agency for Healthcare Research and Quality (AHRQ) collects and reports data on sepsis from institutions through review of International Classification of Diseases, 9th Edition, Clinical Modifications (ICD-9-CM) billing codes.
In this single-center review, the incidence of sepsis and its association with death, intensive care unit admission, and hospital length of stay (LOS) among the various surgical specialties were investigated through review of patients receiving ICD-9-CM codes corresponding to sepsis.
Patients and Methods
At our urban academic tertiary-care center, outcomes of patients aged 18 years or older undergoing a procedure on a surgical service between January 2010 and June 2013 were queried from the University Health System Consortium (UHC) database. Patients with sepsis were identified by the presence of ICD-9-CM codes corresponding to sepsis as prescribed by AHRQ and UHC (Table 1). Patients who presented to the hospital with sepsis at the time of admission were excluded. Institutional Review Board approval was obtained for this study.
ICD-9-CM=International Classification of Diseases, 9th Edition, Clinical Modifications; SIRS=systemic inflammatory response syndrome.
Surgical services were categorized as cardiothoracic, gastrointestinal (GI) and bariatric, neurosurgery, oncologic, orthopedic, otolaryngology, plastic/reconstructive, transplantation, trauma/acute care, urology, and vascular. The outcomes investigated were hospital length of stay (LOS), intensive care unit (ICU) admission, ICU LOS, and in-hospital death.
A physician further reviewed the records of a subset of patients with sepsis who died during their hospitalization between January 2012 and June 2013. The records were reviewed to deetermine the infectious sources of sepsis and the primary procedures associated with the patients' hospitalization. Infectious sources were classified as blood stream, central nervous system (CNS), abdominal, pulmonary, skin or soft tissue, and urinary. Primary procedures were obtained through the primary Current Procedural Terminology (CPT) code associated with the hospitalization.
Continuous data with equal variance were analyzed using the Student t-test, and those with unequal variance were analyzed using the unequal variance t-test. Groups with small samples were assessed for differences using the nonparametric Wilcoxon rank test. Differences were considered statistically significant if the p value was<0.05. All analyses were performed using JMP version 11.0.
Results
Between January 2010 and June 2013, 25,522 patients underwent a procedure in a surgical service at our hospital. There were 863 (3.38%) patients in whom sepsis developed during their hospital stays, as indicated by the assignment of a sepsis-related ICD-9-CM code. The incidence of sepsis was highest in patients undergoing cardiothoracic surgery procedures (233/2776; 8.39%), followed by trauma/acute care surgery (164/2171; 7.55%) and plastic/reconstructive surgery (50/934; 5.35%). Table 2 provides a summary of outcomes by surgical service.
ICU=intensive care unit; LOS=length of stay.
Patients in whom sepsis developed had significantly longer hospital (13.04 vs. 3.61 d; p<0.01) and ICU (7.41 vs. 1.99 d; p<0.01) stays, a higher rate of ICU admission (81.18% vs. 28.84%; p<0.01), and a higher mortality rate (22.31% vs. 2.21%; p<0.01) than all patients undergoing a surgical procedure. Sepsis was associated with a longer mean hospital LOS in every specialty (Fig. 1A). The need for ICU admission among those with sepsis was increased in every specialty other than otolaryngology (Fig. 1B). The mean ICU stay in those with sepsis was increased in every specialty other than plastic/reconstructive surgery, urology, and vascular surgery (Fig. 1C). Sepsis was associated with a higher mortality rate in cardiothoracic, GI/bariatric, trauma/acute care, oncologic, and vascular surgery (Fig. 1D).
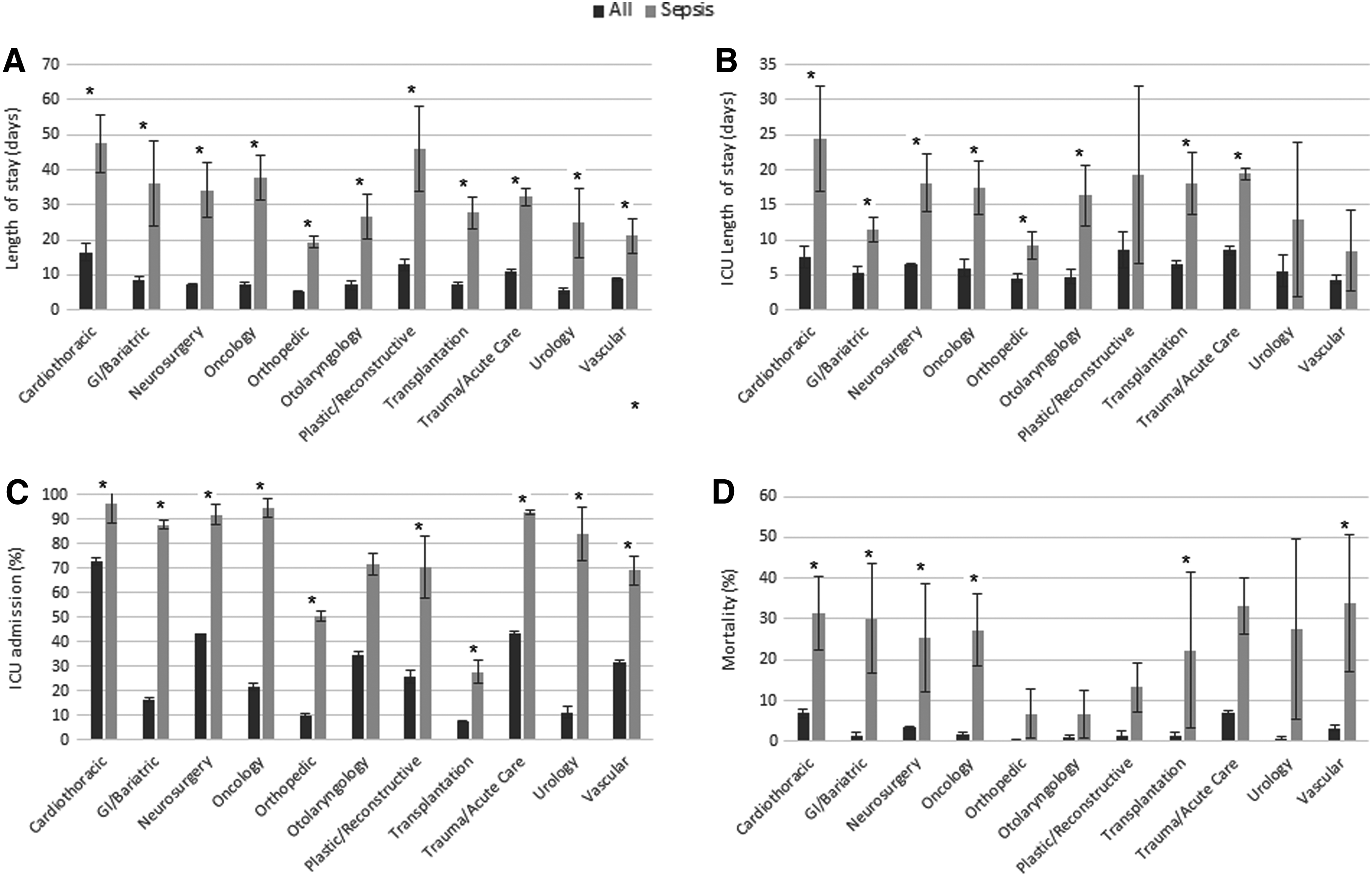
Comparison of outcomes of all patients vs. patients with sepsis by surgical service. *Significant difference at p<0.05. (
In the subset analysis, the records of 243 surgical deaths between January 2012 and June 2013 were reviewed by a physician for the presence and sources of sepsis. There were 62 (25.5%) patients with a sepsis-related death (25.5%). Figure 2 describes the various infectious sources identified in the patients having surgical deaths in each specialty. Of these, 62 patients had 98 total infections, with 40.3% of the patients having two or more concurrent infectious sources. The most common sources of sepsis in the physician-reviewed subset of patients who died during their hospitalization were pulmonary (39.5%), blood stream (35.1%), and abdominal (31.6%) infections. Urinary and skin/soft tissue infections were associated with 17.5% and 18.4% sepsis rates, respectively. Half of the infectious sources in trauma/acute care surgery were of abdominal origin, and almost 70% of infectious sources in neurosurgery were of pulmonary origin. The primary procedures associated with the greatest numbers of sepsis-related deaths were extracorporeal membrane oxygenation (associated with 3.6% of these deaths), small bowel resection (3.0%), insertion of an implantable heart-assist system (2.4%), and open total abdominal colectomy (2.4%).
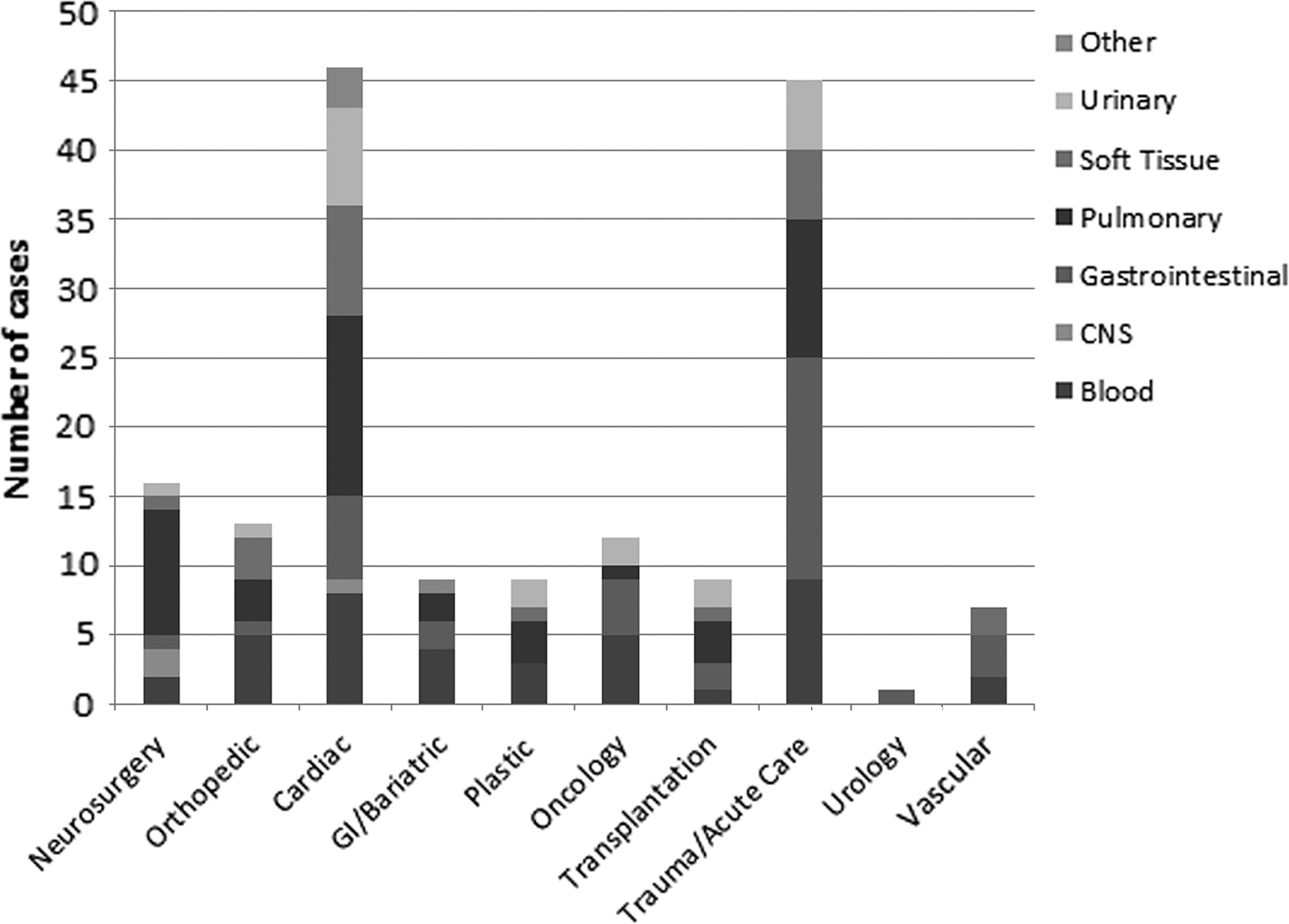
Infectious sources of sepsis-related surgical deaths.
Discussion
This study reiterates the negative overall association of sepsis with hospital LOS, ICU requirement, ICU LOS, and death among patients undergoing surgical procedures. Associated hospital costs, although not explicitly explored in this study, likely increased commensurate with the trends in LOS and level of care. This study also characterizes the specialty-specific effect of sepsis, with all specialties demonstrating a significant positive correlation with hospital stay and almost all noting an association with increased ICU requirements. Six of the 11 specialties also recorded a significant association between sepsis and death.
Patients who are older, have multiple co-morbidities, and are undergoing non-elective surgery are at greater risk for sepsis [10]. This was reflected in the high incidence of sepsis among patients undergoing cardiovascular, vascular, and trauma/acute care surgical procedures. Among the specialties, otolaryngology did not demonstrate a statistically higher ICU need with sepsis, possibly as a result of routine post-operative ICU admission of otolaryngology patients for airway monitoring after major resections and reconstructions. The morbidity of sepsis for otolaryngology is therefore likely better reflected in the significantly greater ICU LOS with sepsis. Plastic/reconstructive surgery did not demonstrate a significantly longer ICU stay, and this may be because, at our institution, plastic/reconstructive surgery patients with free or high-risk flaps are routinely cared for in the ICU for the duration of their hospitalization, thereby skewing the ICU LOS of all plastic/reconstructive surgery patients.
Sepsis was associated with a higher mortality rate among patients undergoing cardiothoracic, GI/bariatric, oncologic, trauma/acute care, and vascular surgery procedures. The correlation between infection and delays in elective surgery after admission supports the idea that the peri-operative period serves as a sentinel point of infection transmission [11]. Overall, pulmonary, blood stream, and urinary infections were the main sources of sepsis among the sepsis-related deaths, emphasizing the importance of adopting proved interventions to reduce such infections [12-14]. Among sepsis-related deaths, extracorporeal membrane oxygenation, heart-assist system implantation, total abdominal colectomy, and small bowel resection were the most common primary procedures. Patients undergoing these procedures are often older, have more co-morbidities, undergo more invasive procedures, are depleted of physiologic reserve, and therefore are likely more sensitive to physiologic insults such as sepsis [9,10,15,16]. The mortality rate associated with sepsis in high-risk patients undergoing major surgery illustrates the association between sepsis and death among vulnerable surgical patients and reiterates the need for greater surveillance and prevention of peri-operative and post-operative infections.
Various strategies for the measurement of sepsis have been used in landmark national epidemiologic surveys of sepsis in the United States, with demonstrated variability in incidence between methods [17]. In the present study, ICD-9-CM administrative codes were reviewed to identify sepsis in surgical patients. Although the approach of ICD-9-CM screening offers a relatively easy method of evaluating sepsis, it has several drawbacks. We have previously reported that the validity of ICD-9-CM screening for sepsis remains questionable, with sensitivity and specificity of only 82.3% and 78.3%, respectively [18-20]. Furthermore, given the undue influence of factors such as ICD-9-CM coding and documentation accuracy on sepsis identification, the ability to generalize such data may be limited. However, this method is being adopted and formalized for benchmarking, reporting, and reimbursement by federal agencies and payers and hence was chosen for the present study. An additional limitation of this approach is that the reports of sepsis obtained from UHC, the current AHRQ data collection consortium, are de-identified. This precludes abstraction of pertinent demographic and co-morbidity information, which would allow better characterization of baseline differences and confounders. The advantage of such an approach is the ability to characterize the relative incidences and correlation of sepsis uniformly with patient morbidity and death within institutions and to use this as a tool for institutional performance evaluation and improvement.
In conclusion, development of sepsis in surgical patients correlates with considerably increased morbidity and mortality rates, with the greatest negative association being observed among patients undergoing cardiothoracic, vascular, and trauma/acute care surgery procedures. Further studies into the effect of and compliance with infection-reduction strategies are required to investigate whether broad-based institutional strategies to reduce pulmonary, blood stream, and abdominal infections prevent the onset of sepsis and its attendant morbidity and death.
Footnotes
Author Disclosure Statement
None of the authors of this study has any relevant disclosures to report.