
Abstract
Abstract
Background:
A factor that may influence the incidence of surgical site infections (SSIs) is the suture used for closure of the abdominal wall because bacteria may adhere to the suture material. Sutures can be coated with antibacterial substances that may reduce the bacterial load in the incision.
Objective:
The aim of this study was to evaluate the effect of triclosan-coated sutures used in abdominal wall closure in patients with fecal peritonitis.
Methods:
A randomized study was performed. Inclusion criteria were intra-operative diagnosis of fecal peritonitis secondary to acute diverticulitis perforation, neoplastic tumor perforation, or colorectal anastomotic leak of previous elective colorectal resection. The patients were randomly assigned to either abdominal wall closure with triclosan-coated sutures (group 1) or sutures without triclosan (group 2).
Results:
Fifty patients were included in group 1 and 51 in group 2. The incisional SSI rate was 10% in group 1 and 35.3% in group 2 (p=0.004; odds ratio [OR]=0.204; 95% confidence interval [CI] 0.069–0.605). A significant reduction in SSIs caused by Escherichia coli and Enterococcus faecalis was observed in group 2.
Conclusion:
The use of triclosan-coated sutures in fecal peritonitis surgery reduces the incidence of incisional SSI.
S
A factor that may influence the incidence of SSIs is the suture used for closure of the abdominal wall because bacteria may adhere to the suture material [4]. Sutures can be coated with antibacterial substances that may reduce the bacterial load in the incision. Triclosan (2,4,4-trichloro-2-hydroxy-diphenylether) is an antiseptic substance that, in preclinical studies, has been shown to reduce the growth of bacteria by inhibiting fatty acid synthesis [5]. Triclosan-coated sutures have been tested clinically in different surgical procedures with conflicting results [6]. Most studies have been performed in clean or clean-contaminated operations, but little is known about the effect of triclosan-coated sutures in dirty procedures. The aim of this study was to evaluate the effect of using triclosan-coated sutures in abdominal wall closure in patients with fecal peritonitis.
Patients and Methods
A randomized study was performed of three surgeons' experiences at General University Hospital of Elche (Alicante, Spain) and University Hospital Ramon y Cajal (Madrid, Spain) between November 2007 and November 2013. Inclusion criteria were intra-operative diagnosis of fecal peritonitis secondary to acute diverticulitis perforation, neoplastic tumor perforation, or colorectal anastomotic leak of previous elective colorectal resection. All patients operated on by these three surgeons were included in the study, without any other selection criterion other than diagnosis of fecal peritonitis. All patients found eligible by these three surgeons were enrolled over this period. Post-operative mortality was the exclusion criterion. Open surgical approach was performed in all included patients and surgical procedures consisted of the Hartmann technique or a diverting stoma.
Calculated sample size was made on an expected superficial SSI incidence of 30% in the control group (non-triclosan suture) based on epidemiology data at our institutions. With 80% power and a p value of 0.05, it was necessary to include 48 patients in each group to demonstrate a 50% reduction in superficial SSIs in the experimental group (triclosan suture). A possible loss of patients at follow-up because of peri-operative mortality was calculated in 15%; therefore, 14 additional patients were added to the sample.
The patients were randomized by means of a sequentially numbered container method into two groups: Fascial closure without triclosan-coated sutures (group 1) or sutures coated with triclosan (group 2). The randomization was performed by the surgeon when the intra-operative diagnosis of fecal peritonitis was made. In the triclosan group, the fascial layer was closed with a polyglactin 910 antimicrobial loop suture size number 2. In the non-triclosan group, identical sutures from the same manufacturer without triclosan were used. After fascial closure, subcutaneous tissue was irrigated with 500 mL of normal saline. Subcutaneous tissue was not sutured in any of the groups. The skin was closed with staples in all patients. During the operation, the skin was prepared with chlorhexidine-alcohol solution, the incision was protected with adhesive plastic devices, body temperature was maintained with thermal blankets, and intravenous fluid infusion was optimized with a FloTrac® sensor (Edwards, Irvine, CA).
The randomization was stratified for etiology of fecal peritonitis (acute diverticulitis perforation, neoplastic tumor perforation, or colorectal anastomotic leak) and performed depending on the intra-operative findings. Peri-operative systemic antibiotics (imipenem 1 g/8 h intravenous [IV]) were used in both groups. In case of allergies to β-lactams, tigecycline (100 mg IV as starting dose, followed by 50 mg/12 h IV) was used. Both antibiotics were maintained for a minimum of 7 d (Fig. 1).
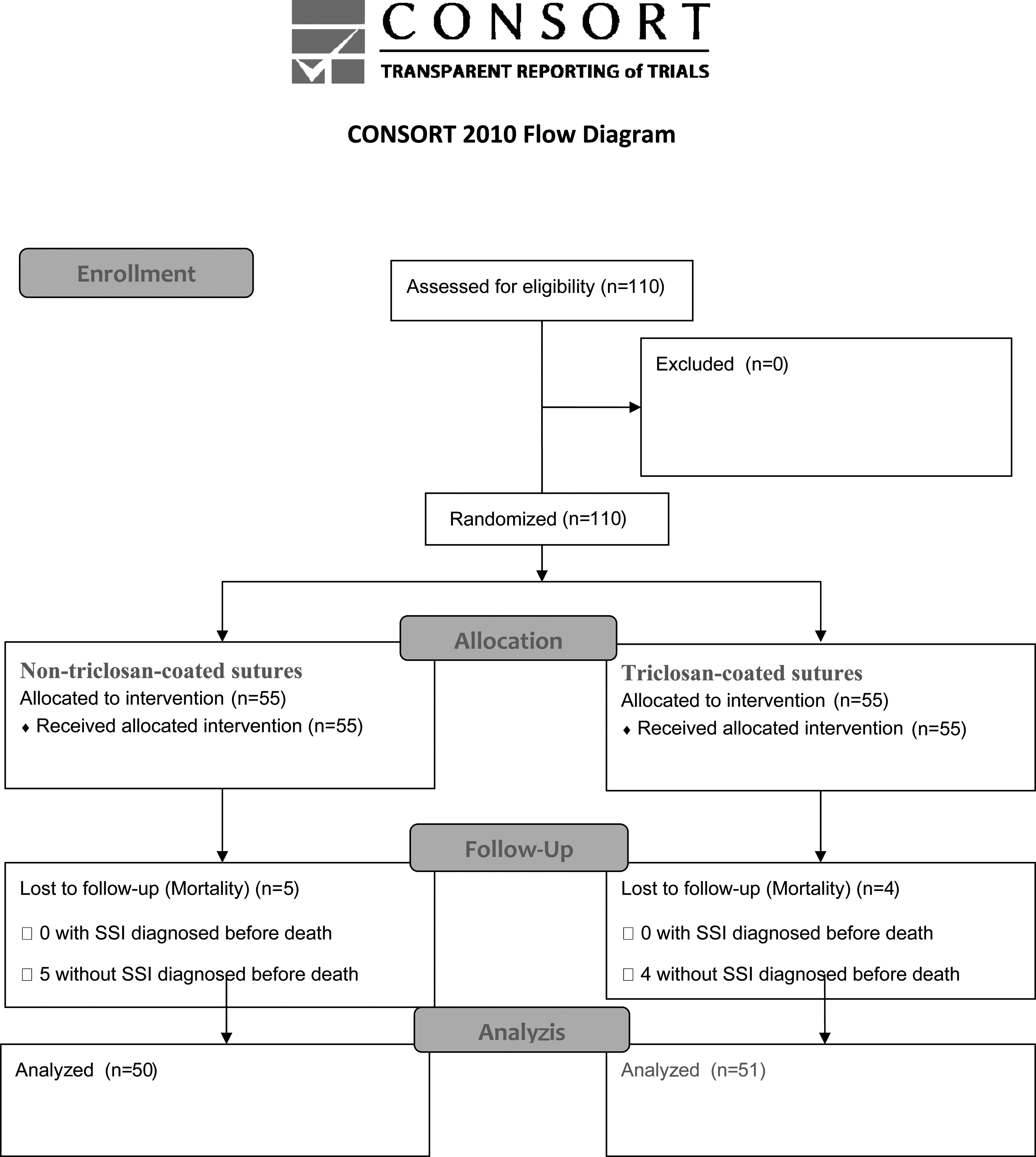
CONSORT 2010 Flow Diagram.
Follow-Up
All incisions were inspected by an epidemiology nurse who was blinded to group allocation at 5, 30, and 60 d after surgery and evaluated according to the U.S. Centers for Disease Control and Prevention (CDC) definition of SSIs (i.e., an incisional SSI must have at least one of the following: Purulent drainage; positive culture; pain, tenderness, redness, and swelling) [7]. In those patients with incisional SSI, the incision was opened by a surgeon and a microbiologic culture was obtained in all cases.
Variables
The investigated clinical variables were age, gender, comorbidities, etiology of fecal peritonitis, incisional SSIs (including deep and superficial), mortality, and hospital stay. Microbiologic cultures were obtained.
Statistics
Statistical analysis was performed with the statistical software SPSS 19.0 for Windows (IBM, Armonk, NY). Quantitative variables that followed a normal distribution were defined by the mean and standard deviation. For non-Gaussian variables, the median and range were used. Qualitative variables were defined by number and percentage of cases.
Comparison of variables was performed with the Student t-test (Mann-Whitney test was used for non-Gaussian variables). Comparison of qualitative variables was performed with the χ2 test; in those cases with fewer than five observations in the cell, Fisher exact probability method was used. The effect was quantified with risk ratio (RR); p<0.05 was considered significant. The study was approved by the local ethics committee. All patients provided written informed consent for the operation and for inclusion in the study.
Results
A total of 110 patients were included in the study; 76 were operated on at University Hospital Ramon y Cajal and 34 at General University Hospital Elche. Nine patients were excluded because they presented with multi-organ failure secondary to septic status and died post-operatively. Because all of the deceased patients died before 96 h post-operative, SSIs could not be evaluated. In total, 50 patients were analyzed in group 1 and 51 in group 2. The patient sample consisted of 62% male and 38% female, with a mean age of 64.7±15.9. Comorbidities included diabetes mellitus (34%), high blood pressure (48%), dyslipidemias (32%), cardiopathies (21%; 15% ischemic cardiopathy and 6% atrial fibrillation), chronic obstructive pulmonary diseases (11%), and non-decompensated liver cirrhosis (1%).
The etiology of fecal peritonitis was colorectal anastomotic leak in 42 patients (41.6%), perforated colonic neoplasm in 25 (24.7%), and perforated acute diverticulitis in 34 (33.7%). There were no differences in comorbidities and etiology of the fecal peritonitis between groups, and their distribution is summarized in Table 1. All patients underwent a Hartmann procedure.
ASA=American Society of Anesthesiologists; NS=not significant.
Mortality was 8.2%, affecting five patients in group 1 and four patients in group 2 (not significant [NS]). Mortality causes were multi-organ failure secondary to septic status. Median hospital stay was 9 d (range, 7–32 d) in group 1 and 9.5 d (range, 7–54 d) in group 2 (NS).
The incisional SSI rate was 10% in group 1 and 35.3% in group 2 (p=0.004; odds ratio [OR]=0.204; 95% confidence interval [CI] 0.069–0.605). The number of patients necessary to treat (NNT) to obtain a benefit was 3.95. There was no association between any of the comorbidities and incision infection. The etiology of fecal peritonitis did not impact incisional SSI. Organ/space SSI was 8% in group 1 and 10% in group 2 (NS). There were no differences in the number of SSIs among hospitals. One hundred and one patients were treated with imipenem and 9 with tigecycline; there were no differences in the SSI rate depending on the antibiotic treatment received.
Microbiologic samples of intra-peritoneal fluids were obtained from all patients intra-operatively. Detected micro-organisms are described in Table 2. There were no significant differences in the microbiologic cultures between groups. A microbiologic sample was also obtained in all patients with incisional SSIs. A reduction in the SSIs caused by Escherichia coli and Enterococcus faecalis was observed (Table 3). In the multivariable analysis, the use of triclosan-coated sutures was the only independent variable associated with a reduction in incisional SSIs (p=0.026) (Tables 4 and 5).
NS=not significant.
NS=not significant.
We strongly recommend reading this statement in conjunction with the CONSORT 2010 Explanation and Elaboration for important clarifications on all the items. If relevant, we also recommend reading CONSORT extensions for cluster randomized trials, non-inferiority and equivalence trials, non-pharmacologic treatments, herbal interventions, and pragmatic trials. Additional extensions are forthcoming: For those and for up-to-date references relevant to this checklist, see www.consort-statement.org.
Discussion
Suture materials have an important role in the development of SSIs by providing a local surface for the adherence of micro-organisms. Once pathogens have colonized suture materials, a biofilm may form subsequently to promote the attachment and reinforce resistance against the attack from the host's immune system and antibiotic treatment, thus predisposing to SSI. Accordingly, the use sutures coated with antimicrobial agents to reduce the risk of suture-related SSI has been investigated. Triclosan dissipates passively from implanted sutures to the surrounding tissues, creating a barrier against bacterial colonization [4,8].
Pre-clinical studies have shown that triclosan-coated sutures reduce the growth of gram-positive and gram-negative bacteria [9,10]. These studies have been followed by retrospective series and prospective controlled trials in different surgical populations to test whether triclosan-coated sutures reduce incisional SSIs; however, results have been conflicting. Justinger et al. [11] reported in a non-randomized study a reduced incidence of infections with triclosan-coated sutures after abdominal surgery. Galal et al. [12] described a reduced infection rate in a randomized study of mixed surgical patients. On the other hand, Baracs et al. [13] found no difference in infection incidence in a randomized controlled trial in colorectal surgery. In a recent systematic review and meta-analysis of randomized trials with triclosan-coated sutures, Chang et al. [14] concluded that triclosan-impregnated sutures do not decrease the rate of SSIs, but also indicated that the quality of the studies was moderate and further high-quality independent studies are required. However, a recent meta-analysis by Wang et al. [15] including 17 randomized controlled trials and involving 3,720 participants, reported that triclosan-coated sutures showed a significant advantage in reducing the SSI rate by 30%. Sub-group analysis revealed consistent results in favor of triclosan-coated sutures in abdominal procedures, but only in clean or clean-contaminated procedures. This meta-analysis included two studies of contaminated and dirty procedures and both failed to demonstrate any advantage of the use of triclosan-coated sutures. This contrasts with our results, which show an 80% reduction of incisional SSIs when triclosan-coated sutures are used.
Unlike antibiotics, which have slower acting, more specific actions that risk mutation and spread of resistance through plasmid transfer and other mechanisms, antiseptic agents carry little risk of resistance because their rapid, direct, and disruptive action is on multiple, non-specific sites of microbial cell biology. Moreover, it has been reported that the Fabl gene encodes the enoyl-acyl carrier protein reductase enzyme, which is essential in bacterial fatty acid biosynthesis; triclosan is a Fabl inhibitor and therefore inhibits fatty acid biosynthesis [16]. Therefore, triclosan can reduce 90% to 99.9% of the inoculates of E. coli and Staphylococcus aureus [10,17]. However, some bacteria have shown a certain resistance to triclosan, such as Pseudomonas aeruginosa, which possesses multi-drug efflux pumps that remove triclosan from the cell [16]. These data are confirmed in our patients, presenting a significant reduction in the involvement of E. coli in incisional SSIs in the triclosan group, whereas that of P. aeruginosa remains unchanged. It is remarkable that in the triclosan group there were no infections caused by or with participation of Enterococcus faecalis, while in the non-triclosan group this micro-organism is involved in 27.7% of the SSIs. Triclosan has been shown to be effective against gram-positive bacteria, although most studies have evaluated only S. aureus, the bacterostatic efficacy of triclosan can be extrapolated to E. faecalis [10].
Although the triclosan-coated polyglactin suture is more expensive, it may be more cost-effective for health care resources in the long term. Nakamura et al. [18] performed an economic analysis of the use of triclosan-coated sutures in elective colorectal surgery. They reported that the additional cost per patient of using triclosan-coated polyglactin suture was $10.80. The total additional cost for 200 patients in 1 y was $2,160. The median additional cost of SSI management was $2,310 per patient. The annual cost of the antimicrobial-coated sutures corresponded with the cost of treating one patient with SSI. Therefore, if 0.5% (1 in 200 patients) of SSIs are prevented, the use of triclosan-coated sutures is cost effective. In our study, the NNT to obtain a benefit was 3.95, thus, the use of triclosan-coated sutures in dirty operations (fecal peritonitis) is a cost-effective measure.
One of the limitations of this study is the small sample size, which prevents the performance of a multivariable analysis. Future studies with larger sample sizes should be performed to confirm our results.
Conclusion
The use of triclosan-coated sutures in fecal peritonitis surgery reduces the incidence of incisional SSIs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.