
Abstract
Abstract
Background:
Forty-six patients (38 females and 8 males) with infected knee arthroplasties were included in this study. In 31 patients (group A) an antibiotic-impregnated articulating spacer was used, whereas in 15 patients (group B) a combination of spacer and antibiotic carrier was used.
Methods:
All patients were reviewed weekly with laboratory examinations (white blood cell count [WBC], erythrocyte sedimentation rate [ESR], C-reactive protein [CRP]) prior to re-implantation. At a mean follow-up of 36 mo (range, 8–60 mo) no patient was lost to follow-up or had died.
Results:
White blood cell count and ESR showed no differences at any time interval. C-reactive protein values had a statistically significant difference between the two groups after the second week (third week p = 0.042) and group B had significantly lower CRP values at every checkpoint thereafter. The re-infection rate was 16.12% in group A and 6.6% in group B (p = 0.192).
D
Recently, new composite biomaterials have been created in an effort to facilitate local antibiotic delivery at the site of infection in new and creative ways and to achieve high local antibiotic concentrations without associated systemic toxicity [12]. These novel local antibiotic delivery systems were designed to provide a framework of osteoinductive and osteoconductive materials along with antibiotic delivery [13]. PerOssal® (Coripharm, Dieburg, Germany) is a new osteoconductive biodegradable composite carrier material consisting of a combination of calcium sulfate and nanocrystalline hydroxyapatite (Ostim®, Osartis, Obernburg, Germany). Because of its good biocompatibility and sufficient and individualized antibiotic release it represents a new treatment option in chronic bone infection [11,14]. The rationale of this study is that a calcium hydroxyapatite local antibiotic delivery system (PerOssal) may overcome the known disadvantages of cement spacers and lead to better outcome in terms of clinical parameters and re-infection rate when combined with pre-formed articulating spacers. Our purpose was to identify potential clinical and laboratory differences between cases that underwent conventional two-stage revision arthroplasty and cases treated with PerOssal as an additional antibiotic carrier.
Patients and Methods
Study design and population
We conducted a single-center cohort study including 46 consecutive patients with deep chronic peri-prosthetic infection after primary total knee replacement (TKR). All patients were diagnosed and treated at our institution during the period 2006–2009. We included consecutive cases of late peri-prosthetic knee joint infections that needed debridement and implant exchange of the existing total knee arthroplasty. We excluded cases with a history of more than one previous total knee arthroplasties at the same joint and patients with known allergy to calcium sulfate, which is an ingredient of the local antibiotic delivery system (PerOssal).
Results of diagnostic tests including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were abnormal in all patients, whereas white blood cell count (WBC) was within normal range. In most cases, radiographs revealed signs of osteolysis or loosening. Triple-phase technetium 99m bone scan was positive in all patients, even in those with normal radiographs. After arthrocentesis, knee joint cultures were positive in 38 of the 46 patients. Infection was diagnosed definitively when more than two intra-operative cultures showed growth of the same organism or when there was a sinus or clinically apparent pus in the knee joint.
Treatment protocol
Initially we performed a pilot study with four cases of infected TKRs (one surgeon) treated by a two-stage revision procedure and the combination of PerOssal with cement spacers; the results were promising. Therefore, we extended the protocol involving two more surgeons and randomized 46 consecutive patients (38 females and 8 males) with mean age 65.3 y (range, 32–84) in two groups. The cases of the two groups were matched regarding age, comorbidities, and types of micro-organisms. All patients had peri-prosthetic TKR infection and underwent a two-stage revision protocol. In the first group (group A), which consisted of 31 patients (25 females and 6 males), only a conventional articulating cement spacer impregnated with tobramycin was implanted whereas in the second group (group B), which consisted of 15 patients (13 females, 2 males), the combination of a spacer and PerOssal pellets applied intra-medullary as an additional antibiotic carrier was used. The antibiotics used in the PerOssal pellets were vancomycin, amicacin, or rifambicin and were applied according to the causative organism. The mean follow-up period of the study was 36 mo (range, 8–60 mo) and was focused on the quality of surgical incision healing and the early clinical and laboratory response of infection to treatment.
The two-stage revision protocol followed in this study was a modification of the procedure originally described by Insall et al. [15]. In both groups the causative organism and its sensitivity to antibiotics was determined by pre-operative knee joint aspiration with the patient free of antibiotic treatment for at least 25 d. First-stage surgical procedure was performed with the patient free of antibiotics for at least 14 d. Multiple culture samples were taken (soft tissue, bone, and fluid), the components were removed, and the joint capsule, synovium, and bone ends were irrigated and debrided thoroughly. In both groups a pre-molded articulating tobramycin-loaded cement spacer was used to maintain the soft tissue tension around the knee, as well as to release high doses of antibiotics locally. In group A the spacer was implanted using vancomycin-impregnated bone cement that was applied early to the components but applied late to the femur, tibia, and patella to allow molding to bone defects and without adherence to bone. In group B, PerOssal pellets, impregnated with the appropriate antibiotic, were implanted both in femoral and tibial intra-medullary canal and sealed by molded cement and the spacer to achieve high antibiotic concentrations (Fig. 1A and 1B). In both groups peri-operative antibiotic therapy was continued until culture results were available and then the appropriate six-week intravenous antibiotic course was implemented based on the antimicrobial sensitivities. Post-operatively all patients were evaluated and reviewed clinically with laboratory examinations (WBC, ESR, and CRP) every seven days.

Anteroposterior (
The re-implantation procedure in both groups was performed at least 6 mo post-operatively according to the suggestions of our infection department, based on the virulence of the isolated pathogens or the medical status of the patients. Re-implantation of definitive implants was considered only if the inflammation markers remained in normal range, the knee joint had satisfactory clinical appearance, and the repeat joint fluid aspiration was negative after a six-week antibiotic-free interval. The second stage of the revision TKR consisted of cement spacer and PerOssal removal, multiple intra-operative cultures, tibial and femoral medullary canal reaming, and thorough joint irrigation with 10 L of normal saline prior to a constrained knee prosthesis implantation (Fig. 2A and 2B). All patients followed a post-operative intravenous antibiotic course until intra-operative culture results were received (at least seven days of incubation); if they appeared positive the appropriate antibiotic treatment was continued for at least six weeks. Rehabilitation began immediately after the second stage. The authors of this study reviewed all patient charts and recorded their status with respect to early response to treatment, eradication of infection, and knee function at the time of the most recent clinical follow-up evaluation.
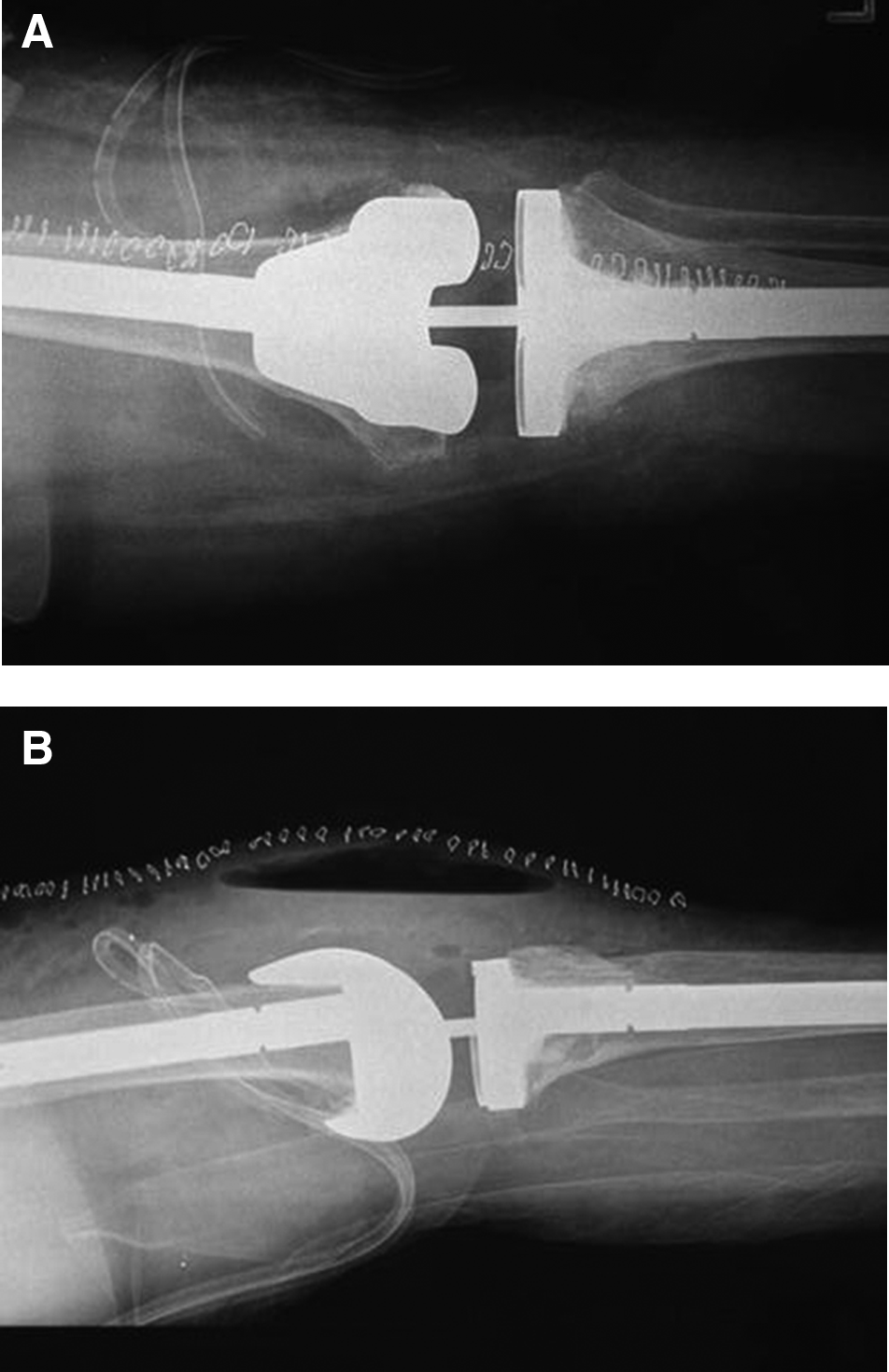
Anteroposterior (
Statistical analysis
One-way analysis of variance (ANOVA) and a post hoc Tukey test were used to test for any significant differences between the mean values of inflammation markers (WBC, ESR, CRP) to reveal potential differences between the two groups.
Results
The underlying diagnosis leading to index arthroplasty was osteoarthritis in 39 patients, rheumatoid arthritis in six patients, and in psoriatic arthritis in one patient. The median time between the index arthroplasty and the resection arthroplasty was 2.8 y (range, 4 mo to 7 y).
The presenting symptoms in all patients were a slowly progressive knee pain and limping after a post-operative symptom-free interval. All patients had a warm, swollen knee with decreased range of motion.
No patient died or was lost to follow-up after a mean duration of 36 mo (range, 8–60 mo). All patients had positive identification of an infecting organism on intra-operative culture specimens.
The most common micro-organism isolated from the intra-operative cultures was Staphylococcus spp. (S. epidermidis in 12 cases, S. aureus in 18 cases, methicillin-resistant S. epidermidis [MRSE] in four cases, methicillin-resistant S. aureus [MRSA] in six cases) and Pseudomonas aeruginosa in two cases, Streptococcus spp. in two cases, Proteus mirabilis in one case and Enterococcus spp. in one case. The second-stage procedure took place at a mean of 8 mo after the resection stage (range, 6–12 mo) (group A mean time interval 8.4 mo [range, 6–12 mo], group B mean time interval 7.6 months [range, 6–11 mo]).
At the latest follow-up, we found that the re-infection rate was 16.13% in group A (5/31 patients) and a 6.67% in group B (1/15 patients) (p = 0.192). All cases revealed the same causative micro-organism with the initial surgery and underwent a repeat two-stage procedure. In all the other cases of both groups, clinical evaluation as well as laboratory (ESR, CRP, complete blooc count [CBC]) and imaging examinations (radiographs, triple-phase technetium 99m Tc-MDP bone scan) revealed no signs of re-infection to date. Pre-operative pain and function improved substantially compared with those at the latest follow-up. We found no difference in the quality of incision healing or clinical eradication of infection between the two groups.
We also analyzed the differences in several inflammatory markers during the observation period. Specifically, the WBC count showed no statistically significant differences between the two groups (p > 0.05) at any time interval (Fig. 3) nor did the ESR show statistically significant differences (p > 0.05) at any time interval (Fig. 4). However, CRP values had a statistically significant difference between the two groups after the second week post-operatively (Fig. 5). Moreover group B had substantially lower CRP values compared with group A at every time point after the second week (third week p = 0.032, fourth week p = 0.038, fifth week p = 0.031, sixth week p = 0.034)

Mean white blood cell count (WBC) values of the two study groups after first-stage revision surgery. No statistically significant differences between the two groups were observed at any time interval.

Mean erythrocyte sedimentation rate (ESR) values of the two study groups after first-stage revision surgery. No statistically significant differences between the two groups were observed at any time interval.

Mean C-reactive protein (CRP) values of the two study groups after first-stage revision surgery. There is a statistically significant difference between the two groups after the second week post-operatively. Group B had significantly lower CRP values compared with group A at every time point thereafter.
Our complications included three cases with spacer dislocation or knee instability (two in group A, one in group B) and four spacer fractures (two in group A, two in group B). No statistically significant differences regarding the complication rates between the two groups were observed (p = 0.768). No adverse effects were observed with the use of PerOssal except in cases in which it was not applied intra-medullary and predisposed in declining incision leakage. At the re-implantation stage PerOssal was removed without difficulty and no bone loss was noted. However, no evidence of osseo-induction or osseo-integration of the substitute in any case could be confirmed.
Discussion
The incidence of peri-prosthetic knee infection ranges between 0.5% and 3% and is a serious problem despite modern technology and rigorous prophylaxis [2,7,15–18]. The rates are higher for rheumatoid arthritis and revision surgery than for primary knee replacement surgery [1,2,7,15]. Numerous options are available to treat the chronically infected total knee arthroplasty, such as antibiotic suppression, irrigation and debridement with component retention, arthrodesis, amputation, and one-stage and two-stage exchange procedures [9]. One-stage exchange arthroplasty has been successful in isolated cases or small series and has the advantages of a single surgical procedure, the ability to maintain motion and soft tissue health, and lower cost, but generally it has not had adequate results in larger series [1,2,19–25]. The two-stage exchange procedure has been shown to provide the best chance for eradication of infection and restoration of joint function, achieving success rates over 90% [7,9,15,26–35]. In our study the overall infection control rates equals the standards reported in the literature. It is now well established that the two-stage re-implantation protocol similar to the one we followed in our study, with systemic antibiotic therapy and use of an articulating antibiotic loaded spacer to provide a high concentration of local antibiotic delivery, maintenance of the knee joint space, and range of motion between stages is the gold standard in the management of peri-prosthetic infections [12,26,29,34–39].
However, the problems related to cement as an antibiotic carrier, in spacer or bead form, are well recognized including bone thermal necrosis, random porosity and unspecified antibiotic delivery rate, bone erosion, and bone damage upon cement removal [10,11]. Although the pre-formed articulating spacers have demonstrated good mechanical properties and standardized antibiotic release [9], they have certain drawbacks, namely they are specific-antibiotic loaded and can be applied on bone surface only. The inferior elution properties of the impregnated cement spacers and the large variability in antibiotic release may result in sub-inhibitory local antibiotic concentrations compromising the effectiveness of the two-stage revision procedure [10,11,16].
There has been a dramatic increase in new technologies designed to improve already existing or invent new and more effective ways of delivering antibiotics to bone and they have shown promising results in vitro [12,40,41]. Specifically, the hydroxyapatite composite is a better local carrier for vancomycin in treating MRSA osteomyelitis [42]. There are few studies in the literature that report on the effectiveness of such carriers in treating chronic bone infection in vivo [41,43] and we are not aware of any that compare such antibiotic delivery systems with the classic cement antibiotic-loaded spacers in the clinical setting. In a study of 25 patients with post-traumatic osteomyelitis, the use of an antibiotic-impregnated calcium sulfate bone substitute as an integral part of a standard surgical protocol was effective (92% success rate) in treating recalcitrant bone infection [43]. The biodegradable nanocrystalline hydroxyapatite and calcium sulfate antibiotic carrier (PerOssal) has been used successfully in a poly-traumatized patient with lower limb osteomyelitis [44] and demonstrated encouraging results regarding infection control, handling, resorption, biocompatibility, and antibiotic release when loaded with gentamicin or vancomycin in 19 patients with spondylodiscitis [41]. In group B in our study, in whom PerOssal had been used as an additional local antibiotic delivery system, the infection control rate was higher compared with group A, in whom the articulating spacer was implanted alone during the first-stage procedure (93.4% in group B versus 83.88% in group A) although the difference was not statistically significant.
One of the most important issues for both the patient and surgeon is determination of when it is safe and appropriate to proceed with re-implantation. C-reactive protein serum concentration obtained just before re-implantation is the most useful post-operative marker after the first-stage procedure because this concentration changes and returns to normal more rapidly than ESR concentrations [45]. C-reactive protein concentrations typically normalize by day 21 after surgery; if they remain elevated this may suggest the presence of persistent infection [46,47]. Definitive treatment by implantation of the prosthesis is performed safely once the CRP values have decreased to normal concentrations [40]. The fact that group B of our study had lower post-operative CRP values compared with group A at every checkpoint after the second week may indicate that the additional use of PerOssal contributes to a better early infection control. Therefore, safe shortening of the waiting period between revision stages might be possible.
The most common complications encountered with the use of spacers include dislocation/instability, implant extrusion, and implant or peri-prosthetic fracture [48]. In our study, complications were few and fortunately of little clinical significance. The use of PerOssal causes no adverse effects as long as it is applied intra-medullary; in other cases it seems to compromise the quality of healing and possibly the overall clinical result. Furthermore, it should be pointed out that neither osseoinductive or osseoconductive properties, nor sufficient mechanical strength [14,49] were observed during the re-implantation stage. Similar to other studies concerning the use of this type of biomaterial, there was no bone loss noted during removal of PerOssal. However, there was no macroscopic evidence that the composite could promote bony union in situations in which structural integrity was less assured [12,43].
One drawback from this clinical study is the limited number of patients contained in each group. Larger series of patients are needed to reveal statistically significant differences in the re-infection rates as indicated by the clinical experience of our study and better determine the effectiveness of PerOssal in the clinical setting. Furthermore, variables such as the chronicity of the infection, host factors, and virulence of the infecting organism should be taken into account when comparing the treatment protocols [1,50]. Another shortcoming is the limited period of follow-up. Longer periods of follow-up may reveal a higher infection recurrence rate in any or both groups of our study.
Conclusion
The nanocrystalline hydroxyapatite and calcium sulfate biocomposite (PerOssal) can be used as an additional antibiotic carrier with pre-molded articulating cement spacers in a standardized two-stage revision surgery protocol of infected total knee arthroplasties. It may be proven to be a useful adjunct in managing knee peri-prosthetic infections by achieving high local antibiotic concentrations and sterilizing tibial and femoral medullary canals. It is associated with more rapid reduction of CRP concentrations, probably because of greater porosity, bacteria-specific antibiotic delivery compared with impregnated cement, and absorption via the medullary canal. Therefore, safe shortening of the waiting period between resection and re-implantation stages might be possible. However, larger series of patients are needed to reveal potential differences in the re-infection rates as indicated by our study and for the investigation of this potentially bone-friendly behavior of PerOssal or similar local delivery systems.
Footnotes
Acknowledgments
Institutional Review Board approval was obtained before initiating the study. The subject permits photographs and information about the case to be published and understands that his or her name will not be published.
The authors had no financial, commercial, or proprietary interest in any drug, device, or equipment mentioned in the submitted manuscript.
Author Disclosure Statement
No competing financial interests exist.