
Abstract
Abstract
Purpose:
The aim of this retrospective study was to evaluate the efficacy of vacuum-assisted closure (VAC) and GranuFoam Silver® dressing (KCI, San Antonio, TX) compared with conventional GranuFoam® dressing in the management of diabetic foot ulcers.
Patients and Methods:
Twenty-one consecutive patients treated with conventional or silver-coated foam dressing were reviewed retrospectively. The wound duration was 6 mo. Group 1 (n=10) received conventional foam dressing (GranuFoam) and group 2 (n=11) received silver-coated foam dressing (GranuFoam Silver). The wound surface area, duration of treatment, bacteriology, and recurrence were compared between the groups. The mean age of the patients was 61.70±10.52 y in group 1 and 67.27±11.28 y in group 2.
Results:
In group 1, the average surface area of the wounds was 45.30±46.96 cm2 and 18.40±23.48 cm2 in the pre-treatment and post-treatment periods, respectively. There was a statistically significant difference between two measurements (p=0.005). Average duration of the treatment was 25.50±27.13 d in this group. In group 2, average surface area of the wounds in the pre-treatment and post-treatment periods were 41.55±36.03 cm2 and 7.64±3.91 cm2, respectively. There was a statistically significant difference between two measurements (p=0.003). Average duration of the treatment was 10.09±3.51 d in this group. The patients treated with silver-impregnated polyurethane foam dressing had reduced recurrence (2 vs. 7 wounds, p=0.030) and increased number of the culture-negative cases at the end of the treatment.
Conclusion:
With the results of the study, it was concluded that VAC GranuFoam silver dressing can be superior to conventional GranuFoam dressing in reducing the recurrence rate of infected diabetic foot ulcers.
I
Vacuum-assisted closure (VAC) and silver-coated dressings have been used in the management of challenging infected wounds [9–11]. It is well known that silver nanoparticles have an antimicrobial effect in the treatment of infected wounds. A study by Li et al. [12] showed that silver nanoparticles can destroy bacterial cell walls and inhibit enzymes for bacterial cell replication in Staphylococcus aureus cells. Exposure of S. aureus to silver results in inhibition of growth of the bacterium and in cellular lysis [13]. Silver has a low toxicity against mammalian cells, which is why silver dressings are used often in wound therapy [14,15]. Silver nanoparticles are able to kill both gram-negative and gram-positive bacteria, and have anti-fungal and anti-viral properties [16–18]. The advantage of VAC silver-coated foam therapy is the enlarged area of contact between the foam and the wound surface, resulting in increased release of antimicrobial silver ions. Furthermore, the close contact between the foam and the bacterial colonized surface under negative pressure increases the anti-bacterial effect [12].
We present our experiences with the treatment of diabetic wounds using silver-coated foam dressing and conventional foam dressing with VAC. Our results indicate that silver-coated foam dressing with VAC can promote faster bacterial clearance and decrease hospitalization time, providing faster healing in the management of infected diabetic foot ulcers.
Patients and Methods
The study was performed in the Department of Plastic Reconstructive Surgery and Infectious Diseases, Gaziosmanpasa University, Tokat, Turkey. Informed consent forms were obtained from the patients (Institutional Review Board number: 13-KAEK-189).
A total of 21 consecutive patients treated with VAC between 2011 and 2013 were reviewed retrospectively. All patients were admitted for treatment of diabetic foot ulcers. All been treated for 6 mo with various traditional methods without results. Clinical characteristics of the patients are summarized in Table 1. The wounds required delayed closure and had wound drainage for more than 5 d, and did not display signs of healing for 6 wks; culture-positive infection and evidence of adequate perfusion (ankle brachial indices ≥0.7 and ≤1.2) was detected as inclusion criteria. Diabetic foot patients with grade 2–3 ulcers were eligible for this study. We excluded the patients presenting with active Charcot arthropathy of the foot, wounds resulting from burns, venous insufficiency, collagen vascular disease, malignant disease in the wound, life expectancy of less than 1 y, and uncontrolled hyperglycemia (glycosylated hemoglobin [HbA1c] >12%). Patients were also excluded if they were being treated with corticosteroids, immunosuppressive drugs, or chemotherapy.
Data were presented as n (%) and mean±standard deviation (SD).
The infections were evaluated together with the hospital infection committee and were followed by wound cultures and laboratory parameters (sedimentation, C-reactive protein, leukocyte count) taken twice a week. Once per week, blood samples were obtained to assess serum pre-albumin, albumin, and HbA1c. If the pre-albumin concentration was less than 0.16 g/L or the albumin amount was less than 30 g/L, dietary supplementation was initiated by a nutritionist. The biopsies were obtained from the wounds after the first debridement and the swabs were studied at 72 h after antibiotic therapy was begun. Wound evaluation included the location, date of onset, size, presence of edema, drainage type or amount, and granulation tissue formation assessment.
All patients underwent surgical debridement as soon as possible. After initial removal of necrotic tissue, the wounds were covered post-operatively with wet-to-dry moist dressing prepared by moistening cotton gauze with 0.9% normal saline. In case of progressive necrosis, surgical debridement was repeated. As the causative micro-organisms were determined, antibiotic therapy was modified accordingly. After adequate hemostasis, silver or conventional foam dressing was applied and the pump was set to a continuous negative pressure of 125 mm Hg. When the patient felt pain or too much bleeding was observed in the wound despite hemostasis, a lower negative pressure of −75 to −100 mm Hg was used.
The negative pressure system uses latex-free and sterile polyurethane foam dressing that is fitted at the bedside to the appropriate size for every wound, and then covered with an adhesive drape to create an airtight seal. A T.R.A.C.™ Pad (Therapeutic Regulated Accurate Care; KCI, San Antonio, TX) lies on top of the foam within the drape, and senses, monitors, and maintains the target pressure accurately at the wound site to provide controlled negative pressure. Tubing attached to the T.R.A.C. Pad connects to a fluid collection canister contained in a programmable, portable, computer-controlled vacuum pump creating negative pressure at the wound surface interface.
The dressing changes were made every 48 h. Further debridement was performed as needed under surgical conditions and general anesthesia. Vacuum-assisted closure therapy was continued until achieving adequate, healthy granulation tissue. The treatment was ended when sufficient accelerated granulation tissue formation, considerable shrinkage, and bacterial clearance was achieved and exudate cleared from wounds. Wounds that were more than 5 cm2 were covered by using flaps or skin grafts. In both groups, at the end of the treatment, no surgical approach was performed for small wounds of smaller than 5 cm2.
Statistical analysis
Mann–Whitney U test was used to compare the continuous variables between VAC and conventional treatment groups. Wilcoxon test was used to compare the wound areas between pre-treatment and post-treatment terms. The continuous data were presented as the mean±standard deviation. χ2 Test was used to compare the categorical data between VAC and conventional treatment groups. Categorical variables were presented as a count and percentage. A p value <0.05 was considered significant. Analyses were performed using commercial software (IBM SPSS Statistics 19, SPSS Inc., an IBM Co., Armonk, NY).
Results
Table 1 shows demographic and individual characteristics of the groups. Of all patients, 12 were male (66%) and 9 were female (34%). Mean age was 61.70±10.52 y in group 1 and 67.27±11.28 y in group 2.
In group 1 (used conventional foam), average wound size was 45.30±46.96 cm2 in the pre-treatment period. At the end of the treatment wound size was 18.40±23.48 cm2 (Figs. 7–11). There was statistically significant difference between two measurements (p=0.005). Average duration of treatment was 25.50±27.13 d. There were five additional debridements after initial debridement in this group. At the beginning of the treatment, seven bacterial cultures were reported as polymicrobial and others were detected as Enterobacter cloaca, Streptococcus agalactiae, and Clebsiella oxitoca (Table 2). In this group, the number of bacterial cultures found to be negative was three at the end of the treatment. Two patients had small wounds of less than 5 cm2 at the end of the treatment. These wounds closed without the need for any operation and were treated with wet-to-dry dressing until total closure whereas others were closed by various surgical methods.

Grade IV diabetic ulcer on the right foot.

The wound was debrided properly and standard granufoam dressing was applied every 48 hours.

The wound was ready for covering with skin graft at the end of the treatment of 31 days.

The photograph shows the patient with left infected diabetic heel ulcer after initial debridement.
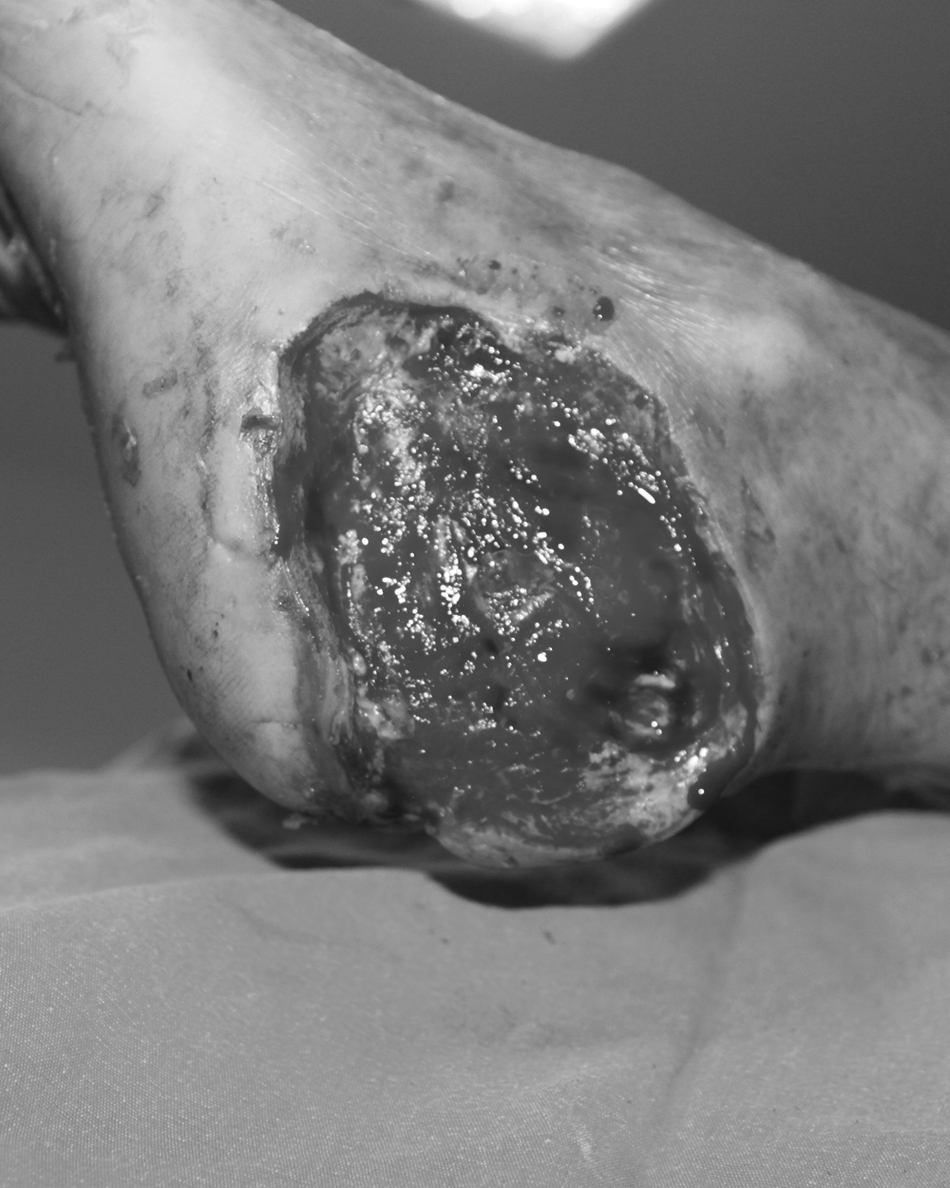
The view of the same patient after the application of 23 days with standart foam dressing.
In group 2 (used silver-coated foam; Figs. 1–6), at the beginning of the treatment, the average wound size was 41.55±36.03 cm2 and the same measurement was 7.64±3.91 cm2 at the end of the treatment. The number of additional debridements after initial debridement was six in this group. There was statistically significant difference between two measurements (p=0.003). The average duration of total application was 10.09±3.51 d in this group. In group 2, seven bacterial cultures were reported as polymicrobial and others were isolated as E coli, Morganella morgagni, Staphylococcus epidermidis, and Staphylococcus aureus at the beginning of the treatment (Table 3). At the end of the treatment, the number of bacterial culture found to be negative was nine. The number of wounds that did not require performing an operation was three and were left for secondary healing. Three patients had small wounds of less than 5 cm2 at the end of the treatment. These wounds closed without the need for performing any operation and were treated by wet-to-dry dressing until total closure. There was no statistically difference between two groups in terms of the change of the wound surface area (p=0.549). The other complications of VAC such as hematoma or excessive bleeding were not observed.

An infected and grade IV diabetic foot ulcer in a 56 year-old-male.

After the wound debridement silver granufoam dressing was performed.

Photograph shows that enhances granulation tissue formation, improves wound healing. The dressing changes were made every 48 hours. Total application time was 9 days.

A case of right diabetic heel ulcer. The patient had an arterial insufficiency and a history of left leg amputation.
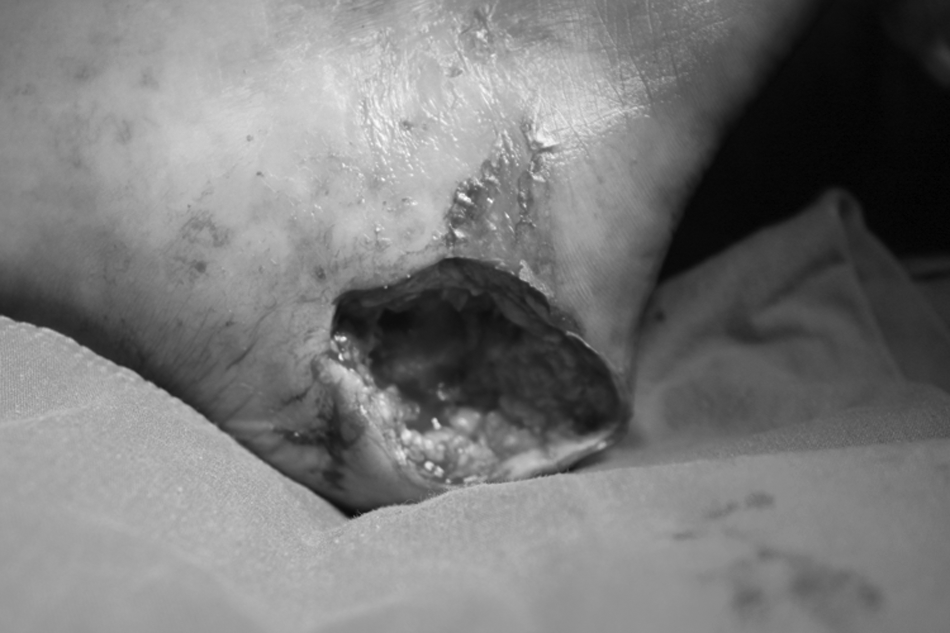
A case of right diabetic heel ulcer. The patient had an arterial insufficiency and a history of left leg amputation.

The wound was debrided and silver-impregnated foam with VAC therapy was followed for 8 days.
All patients were followed for an average of 12 mo; two recurrences were found 1 mo after discharge in group 2 and seven cases in group 1. There was statistically significant differences concerning the recurrence rate between the groups.
Discussion
It is well known that the existence of more than three species of micro-organisms increases the risk of infection in a chronic wound because they may develop synergies with each other [12]. In infected wounds with multiple species, distinguishing which is the causative organism may be difficult. In the absence of true quantitative cultures, immediate broad-spectrum antibiotic coverage and treatment should be administered. In our patients, multiple incisional biopsies for pathologic examination and tissue samples for bacterial culture were obtained. Intravenous antibiotics were started empirically. At the beginning of the treatment, a total of 14 cultures were polymicrobial in both groups. Aerobic gram-positive cocci was isolated in 2 patients while aerobic gram-negative bacilli in 5 patients. Antibiotic regimens were changed considering the culture results. To determine the predominant pathogens in diabetic foot infections, bacterial culture specimens should be obtained appropriately and the microbiology laboratory should be informed.
In diabetic foot infections, aerobic gram-positive cocci (especially Staphylococcus aureus) are the predominant pathogens. Patients who have acute or chronic wounds or who have recently received antibiotic therapy may also be infected with gram-negative bacilli and those with foot ischemia or gangrene may have obligate anaerobic pathogens [19]. Staphylococcus aureus is much more pathogenic than S. epidermidis. However, S. epidermidis plays an important role in implant-associated infections [20,21]. In clinical practice, although silver-coated foam is the common interface material used in the treatment of chronic and infected ulcers, the depth of penetration into tissue in vivo and the behavior of silver and micro-organisms under higher negative pressure are still unknown. Ionic silver can be considered as an ideal antiseptic for the treatment of local infections and the struggle against antibiotic-resistant opportunistic and strict pathogenic bacteria in wounds because of its broad-spectrum bactericidal activity [22–24]. The antimicrobial effects of silver include direct inhibition of bacterial cell respiration, inactivation of intracellular enzymes, and alterations to the cell membrane. It has been reported previously to be effective in inhibiting growth of commonly found pathogens in the diabetic foot, including methicillin-resistant Staphylococcus aureus (MRSA) [25]. Silver ions are released into the wound bed from the dressing upon contact with wound exudate and the dressing has a rapid (within 30 min) and long-lasting antimicrobial activity (up to 7 d) against a wide range of diabetic foot wound pathogens [26]. Also there are several reports suggested that silver-coated dressings may be a suitable option to accelerate wound re-epithelialization [27].
The combination of silver foam and negative-pressure therapy can provide an optimal distribution of silver ions in infected tissue. Compared with conventional foam, the antibacterial effect of the silver foam may reduce the times of treatment [28]. In an in vitro study, Sachsenmaier et al. [13], confirmed the in vitro antimicrobial effect of silver ions against S. aureus and S. epidermidis under continuous negative-pressure therapy of 25 mm Hg [13]. Asavavisithchai et al. [29] used GranuFoam Silver dressing in various pore sizes and porosity with negative pressure. In that study, the foams demonstrated stronger microbial growth inhibition on gram-negative bacterium (E. coli) than gram-positive bacterium (S. aureus). Higher antimicrobial efficacy was found for silver foams with larger pore size. Nevertheless, the difference in the antimicrobial effects between various pore sizes of the foam was smaller when foam porosity increases from 60% to 80%. The study showed that the effect of particle addition on the bacterial growth inhibition was stronger than the effect of particle sizes and pore sizes of the foams. The positively charged silver ions released from the surface of silver foam structure altered the morphology of bacteria strains in which disruption of cell wall and eventually damage were implemented. GranuFoam Silver dressing takes advantage of the potency of silver via a coating on standard GranuFoam dressing that enables the release of silver ions into the wound through the oxidation of the silver coating [30].
In the present study, the average surface area was 45.30 cm2 in group 1 and 41.55 cm2 in group 2 at the beginning of the treatment. At the end of treatment these measurements were 18.40 cm2 and 7.64 cm2, respectively. The difference between pre-treatment and post-treatment measurements was statistically significant in each group. Significant difference was not found in the change of the wound surface areas between the groups. However, there were significantly different post-treatment measurements between group 1 and 2. In group 2 (silver-coated foam), duration of the treatment was 2.5 times shorter (25.50 vs. 10.09 d) than group 1 and there was statistically significant differences between two groups.
In a similar study by Armstrong et al. [1], the authors used VAC therapy in the treatment of acute and chronic diabetic foot ulcers compared to standard wound therapy. They suggested that there was no statistically significant difference in terms of achieving complete wound closure in either treatment group. In a study by Nather et al. [31], changes in wound dimension, presence of wound granulation, and infection status of diabetic foot ulcers in 11 consecutive patients with diabetes mellitus were followed over the course of VAC therapy. In that study, healing was achieved in all wounds. Nine wounds were closed by split-skin grafting and two by secondary closure. The average length of treatment with VAC therapy was 23.3 d. Ten wounds showed reduction in wound size. All wounds were satisfactorily granulated and cleared of bacterial infection at the end of VAC therapy. The authors concluded that VAC therapy was useful in the treatment of diabetic foot infection and ulcers after debridement. In a similar study, Egemen et al. [10] used GranuFoam Silver dressing with VAC and suggested that application of negative-pressure wound therapy provides quick wound-bed preparation and complete graft take in venous ulcer treatment [10].
In another study by Kalemikerakis et al. [32], 26 patients with malodorous wound were evaluated. Thirteen patients formed intervention group A (foam dressings with silver) and another 13 patients formed the control group B (foam dressings without silver); patient selection was random. The dressing changes were carried out according to the needs of the ulcer and depending on the level of the exudates. Odor was evaluated 4 wks after the start of the study. In group A, 10 of 13 (76.9%) patients showed a significant reduction of the odor compared with 4 of 13 (30.8%) patients in group B.
Similarly, Gery et al. [33] investigated GranuFoam Silver with VAC therapy compared with moist saline dressing changes [33]. The authors reported that silver-impregnated VAC therapy may be a useful adjunct in wound bed preparation when standard treatment modalities have failed. In addition, they suggested that the silver-impregnated VAC device could combine an antimicrobial effect with the microdeformational advantages of VAC therapy. Therefore, infectious micro-organisms that impair wound healing can be eradicated by the antimicrobial properties of silver while granulation tissue formation is induced. Although chronically colonized wounds are often refractory to definitive treatment, the patients in that study were able to undergo substantial split-thickness skin grafting following 2 to 4 wks of silver-impregnated VAC therapy. Two months after treatment with the silver-impregnated VAC device, these patients' skin grafts were more than 90% healed, requiring only minimal wound care. In a study by Cho et al. [34], they used silver-impregnated polyurethane foam dressing in an experimental wound model. The authors suggested that it had an excellent wound healing effect without any inflammation [34]. Leininger et al. [35] used VAC therapy in the treatment of 88 contaminated soft tissue wounds. Their experience suggested that conventional wound management may be improved with VAC therapy, resulting in earlier, more reliable primary closure of wartime injuries. In that study, the wound infection rate was 0% and the overall wound complication rate was 0%. In our study, after the application of silver-impregnated foam with VAC, the number of the wounds with negative bacterial culture was nine. This result was significant compared with group 1 and can be explained by the clearance and absorption behavior of polyurethane foam under negative pressure and the efficacy of silver as a topical antibacterial agent. In this study, there were three patients in group 2 who had wounds smaller than 5 cm2 at the end of the study. These patients had secondary wound healing whereas eight of ten patients in group 1 required surgical intervention to close the wounds. We suggest that silver-coated foam with VAC therapy could provide a higher proportion of healed wounds in a shorter period of time than conventional GranuFoam dressing treatment with VAC.
Conclusion
In the present study, our results showed that efficacious wound care and appropriate antimicrobial therapy can have crucial roles in the treatment of challenging diabetic ulcers. Also, silver-coated foam dressing combined with VAC provided good clinical efficacy, and the hospitalization duration was also decreased. In conclusion, silver-coated foam dressing in VAC therapy was found to be superior to conventional foam dressing in obtaining healthy, faster wound healing and bacterial clearance with a lower recurrence rate.
Footnotes
Author Disclosure Statement
No competing financial interests exist.