
Abstract
Abstract
Background:
A retrospective study was conducted to investigate the validity and the effectiveness of early empiric antibiotic and de-escalation therapy for the treatment of severe sepsis and septic shock patients in the intensive care unit (ICU).
Methods:
Patients admitted to the ICU at Chiba University Hospital from January 1, 2010, to December 31, 2012, for the treatment of severe sepsis or septic shock were selected for analysis.
Results:
One-hundred and ten patients were enrolled for the analysis. Carbapenems were selected most frequently (57.3%), followed by cephalosporins (22.7%), and penicillins (21.8%). Empiric antibiotic therapy was appropriate for 85 (77.3%) patients. Mortality rates for patients with inappropriate empiric therapy was 36.8%, whereas mortality rates for patients with appropriate empiric therapy was 17.5%. Among the patients with appropriate empiric antibiotic administration, de-escalation was associated with lower mortality rates of 5.0% for severe sepsis and 9.7% for septic shock patients. The mortality rates for the no de-escalation group were 19.0% and 35.7%, respectively.
Conclusion:
Empiric antibiotic therapy was acceptable for severe sepsis and septic shock patients treated in the ICU. The appropriate selection of empiric antibiotics was related to a greater rate of de-escalation and better survival. The risk of multi-drug-resistant bacterial infections was not as high as expected, but will need further attention in the future.
S
A retrospective study was conducted to investigate the validity and the effectiveness of early empiric antibiotic and de-escalation therapy for the treatment of severe sepsis and septic shock patients in the ICU.
Patients and Methods
Study design
A retrospective analysis of the patients who admitted to the ICU at Chiba University Hospital from January 1, 2010, to December 31, 2012, for the treatment of severe sepsis or septic shock was conducted. The study protocol was approved by the ethics committee at Chiba University Graduate School of Medicine.
Patient selection
The patient selection from the hospital database was conducted according to the following procedure. First, patients who were registered with the diagnosis of sepsis according to the ICD-10 classification at the time of the ICU admission, with records of blood cultures within 7 d of their diagnoses, were selected. Then, to select patients with organ dysfunctions, patients with records of mechanical ventilation (MV), continuous renal replacement therapy (CRRT), or both, during their ICU stays were selected. Mechanical ventilation and CRRT are strongly recommended for the treatment of respiratory, renal, and other organ dysfunctions such as cardiovascular instability in the local treatment protocol for severe sepsis and septic shock patients. Finally, the medical records of all the selected patients were reviewed for the final confirmation of the eligibility criteria, and the final discrimination was made between severe sepsis and septic shock. We adopted the definitions for sepsis, severe sepsis, and septic shock as described by the Consensus Conference Committee of American College of Chest Physicians and the Society of Critical Care Medicine [12].
Methods
Patient characteristics including age, gender, and diagnosis upon admission were recorded. The source of the infection was determined according to the medical records and the results of the microbial cultures. The results of the cultures were considered positive if a microorganism was cultured from the predicted source or the blood, and it was considered pathogenic. A microorganism was considered pathogenic if it was outside the normal flora for the site of the infection, detected in dominant counts, or suspected from the medical records. If multiple microorganisms were cultured, those considered pathogenic were all included for the analysis.
The empiric antibiotic therapy regimens, i.e., the antibiotics administered before the results of the cultures, were recorded. Empiric antibiotic therapy was considered effective if the administered antibiotic was susceptible for the cultured organism, or when patient condition recovered despite failure to identify the source or the cause of infection. De-escalation was defined as narrowing of the antibiotic spectrum according to the result of the culture or the patient condition, either by changing or decreasing the number of antibiotics. The selections of empiric antibiotics were analyzed for the effectiveness against the target organism and site of the infection. Antibiotics were classified according to their mechanism of action, chemical structure, or spectrum of activity; e.g., penicillins, cephalosporins, carbapenems, fluoroquinolones, aminoglycosides, anti-MRSA (and other resistant gram-positive bacteria), and lincomycin. Mortality rates were analyzed according to the source site of the infection, the type of bacteria, infected organism, and the type of antibiotic used. The relations between successful empiric therapy and de-escalation to mortality rates were also analyzed, respectively.
Statistical Analysis
Data are presented as mean and standard deviation, or absolute numbers and percentages. We tested for differences between the two groups using an unpaired t-test for continuous data and Chi square test for categorical data. All statistical analyses were carried out on PASW statistics 18 (SPSS Inc., Chicago, Illinois).
Results
Patient demographics
Table 1 presents the patient demographics. There was no substantial difference between the patient characteristics. SOFA score was greater in the septic shock patients (12.7 ± 5.0) compared with the severe sepsis patients (8.7 ± 4.9). Acute Physiology and Chronic Health Evaluation II (APACHE II) score and serum IL-6 concentrations were also relatively greater in the septic shock patients. Empiric antibiotic therapy was administered as a combination of two or more antibiotics in a greater majority of the patients (63.6%). The number of administered antibiotics for severe sepsis patients was 1.9, whereas it was 2.1 for septic shock patients. The empiric therapy was appropriate for 80.4% of the severe sepsis patients and 74.6% of the septic shock patients. Among them, antibiotics were de-escalated in 48.8% and 68.2%, respectively. ICU mortality rates were 15.7% for the severe sepsis patients and 27.1% for the septic shock patients.
, Unpaired t-test
, Chi-square test
#, mean ± SD
APACHE II = Acute Physiology and Chronic Health Evaluation II; ICU = intensive care unit; SOFA = sequential organ failure assessment.
Empiric antibiotic therapy
Figure 1 shows the frequency of the type of empiric antibiotics used for the study patients. Carbapenems were selected most frequently (57.3%), followed by cephalosporins (22.7%) and penicillins (21.8%). The frequency varied among the different foci of infection (Fig. 2). The greater trend for the selection of fluoroquinolones (23.3%) for the respiratory tract infections, carbapenems for the abdominal infections (78.3%), cephalosporins for the urinary tract infections (54.6%), and penicillins and lincomycins for the soft tissue infections (47.6% and 52.4%) reflect the guideline oriented selection of antibiotics by the attending doctors [9].
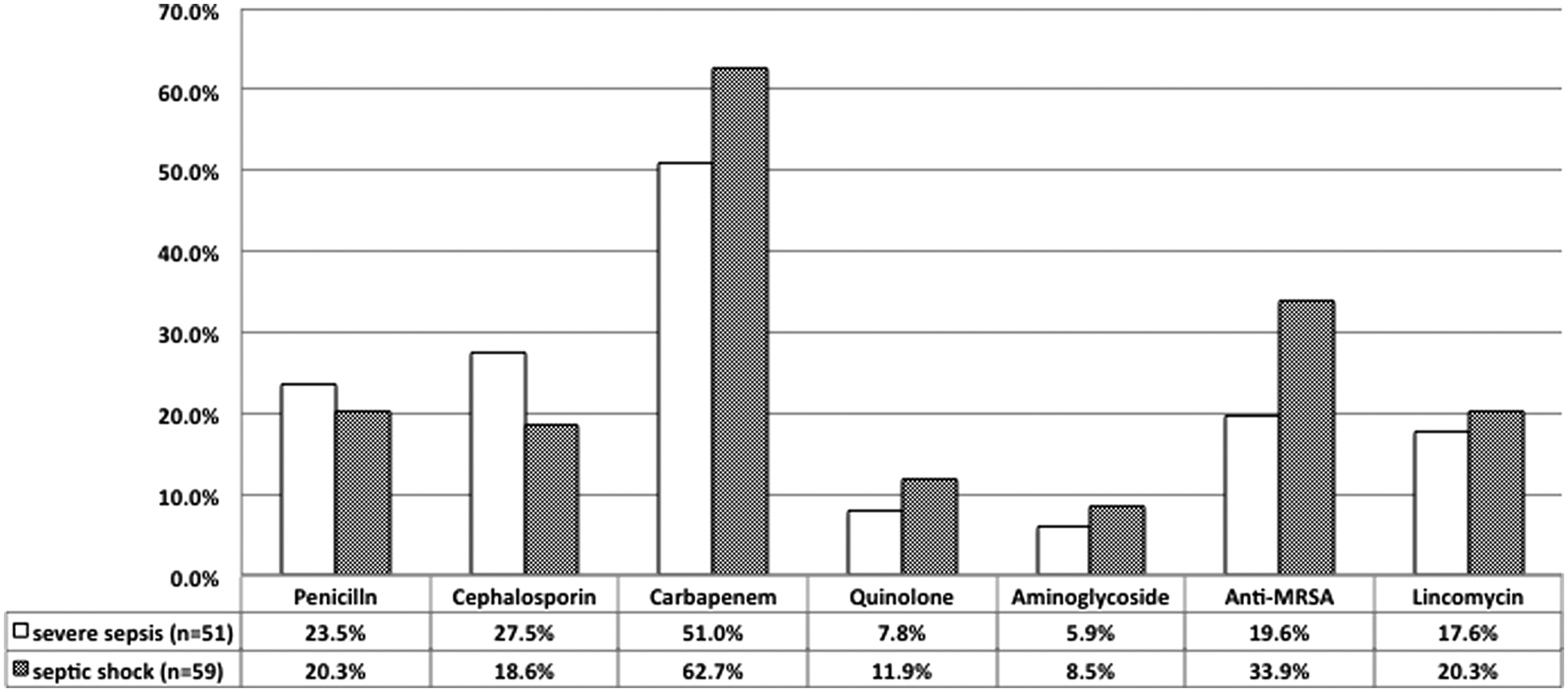
Selection of antibiotics for severe sepsis and septic shock: Selection of the initial empiric antibiotic regimen for severe sepsis and septic shock are indicated. White bars represent the selection in severe sepsis patients, and shaded bars represent the septic shock patients. Carbapenems were selected most frequently, followed by cephalosporins and penicillins.
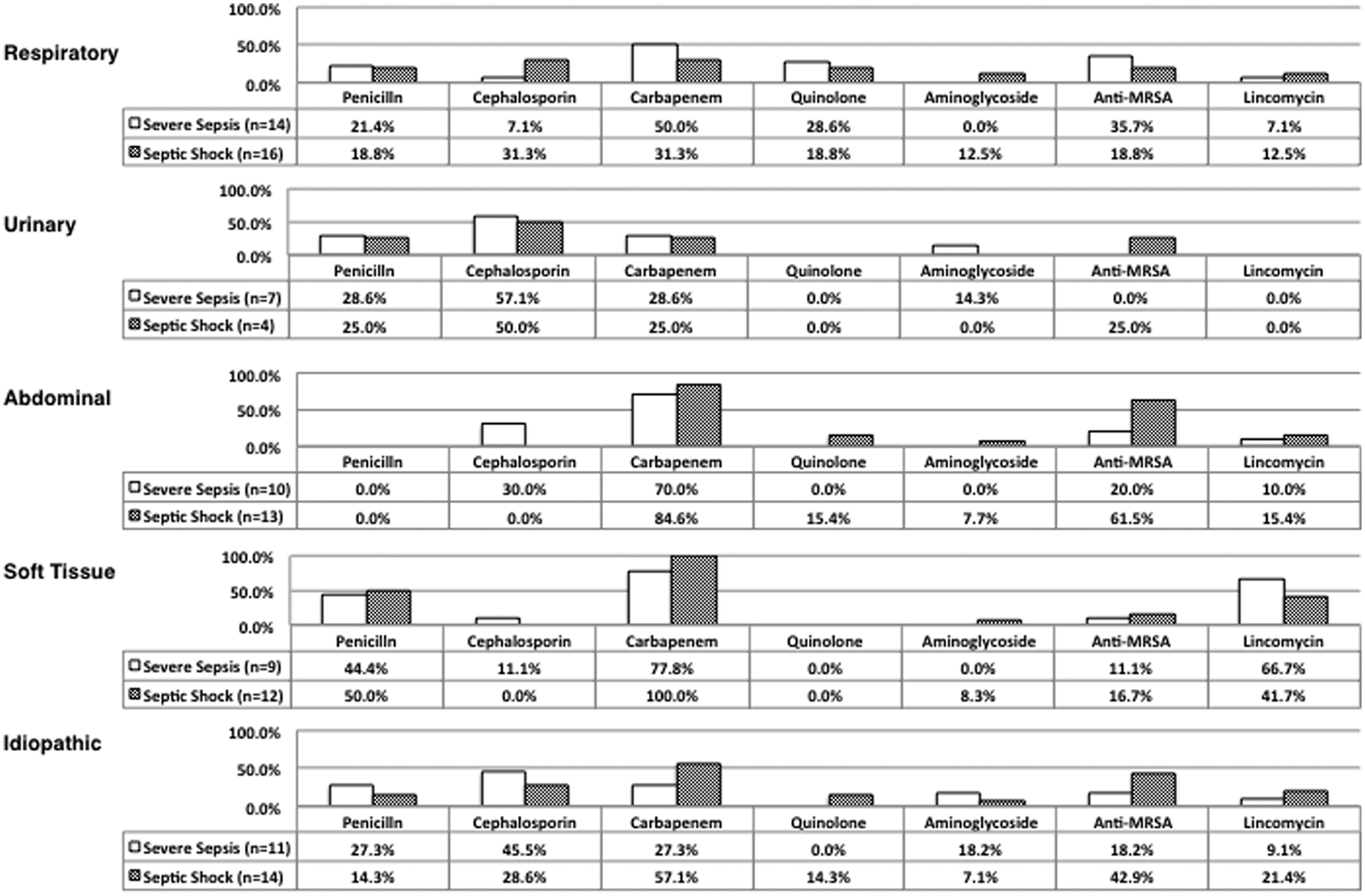
Antibiotic selection by focus of infection: Selection of antibiotics are classified according to the foci of infection: Respiratory, urinary, abdominal, soft tissue, and idiopathic. White bars represent the selection in severe sepsis patients, and shaded bars represent the selection in septic shock patients. The pattern for the selection of empiric antibiotics varied among the different foci of infection.
Source of infection and infected pathogens
The results of the bacterial cultures are shown in Figure 3. Positive cultures were obtained from 96 (85.5%) patients. No specific trends were observed for the pathogens of the respiratory and the abdominal infections. The urinary tract infections were caused mainly by gram-negative bacteria such as Escherichia coli, and the soft tissue infections were caused by Streptococcus and other gram-positive bacteria (Fig. 3a). There was no apparent difference between the overall trends in the pathogens for severe sepsis and septic shock patients (Fig. 3b). Inappropriate empiric antibiotic therapy was identified for a small portion of resistant bacteria, such as MRSA, E. coli, and Pseudomonas aeruginosa (Fig. 3c). However, only the pathogens that induced inappropriate empiric antibiotic therapy caused mortality events, suggesting a relation between inappropriate therapy and greater mortality rates (Fig. 3c, d).
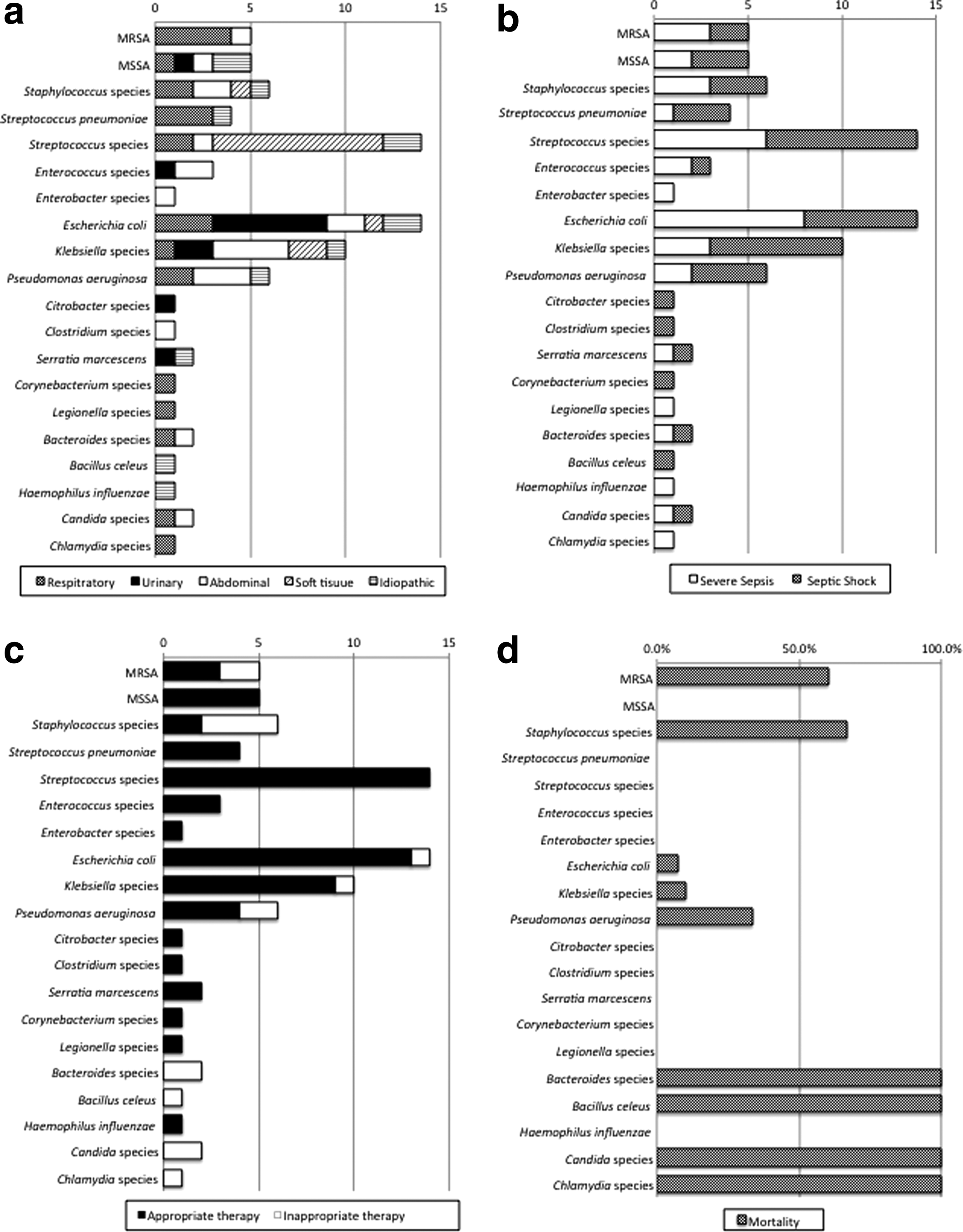
Result of microbial cultures:
Appropriate therapy and mortality rates
The relation between the types of empiric antibiotics and mortality rates is shown in Figure 4. The mortality rate was the lowest for patients treated with penicillins (8% overall), despite their relatively frequent use. The relation between appropriate empiric therapy and the overall mortality is as shown in Figure 5a. Mortality rates for patients with inappropriate empiric therapy was 36.8%, whereas mortality rates for the patients with appropriate empiric therapy was 17.5%.
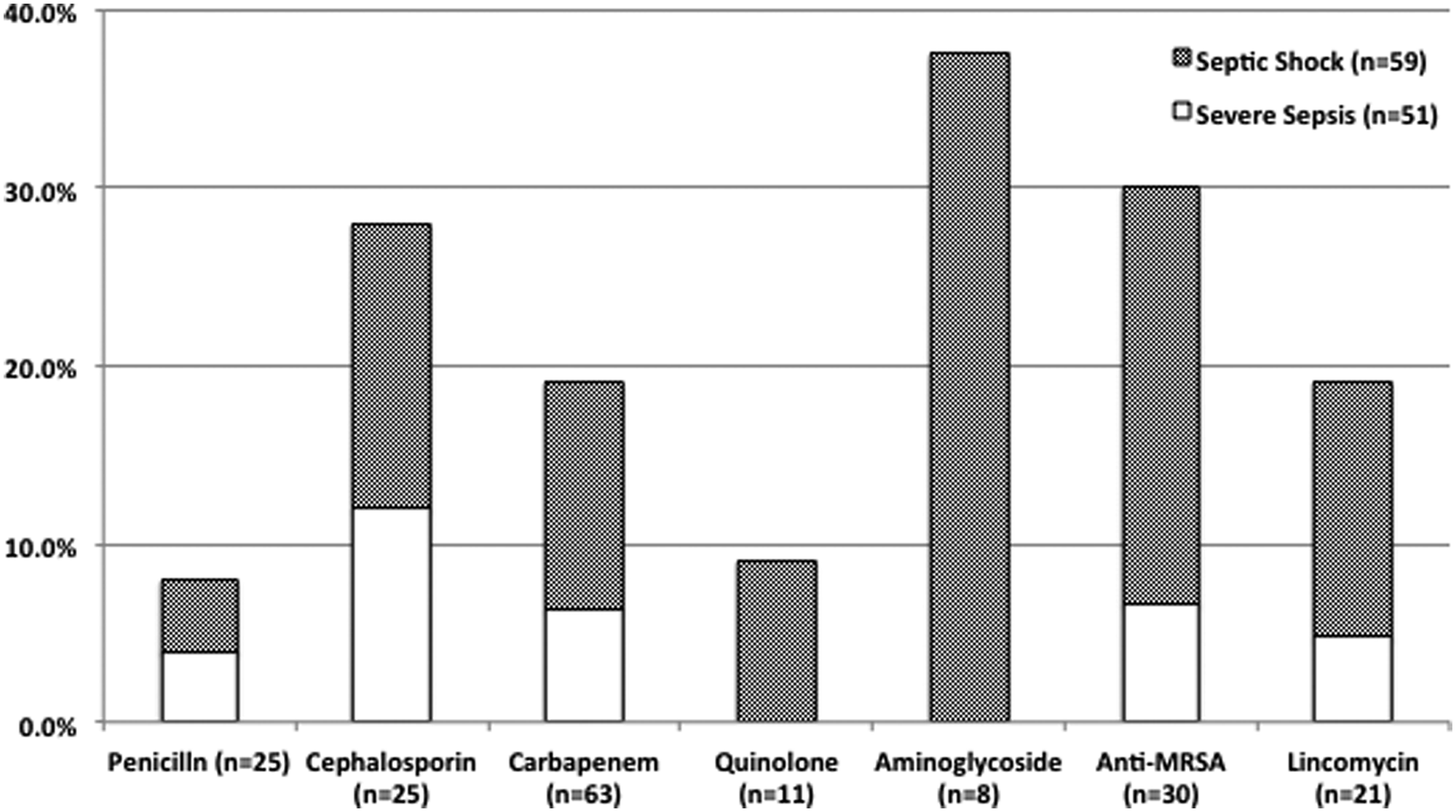
Relation between ICU mortality and empiric antibiotic therapy: Mortality is classified according to the initial empiric antibiotic selection. White bars represent mortality in severe sepsis patients, and shaded bars for septic shock patients. The mortality rate was the lowest for patients treated with penicillins, despite the relatively frequent use.
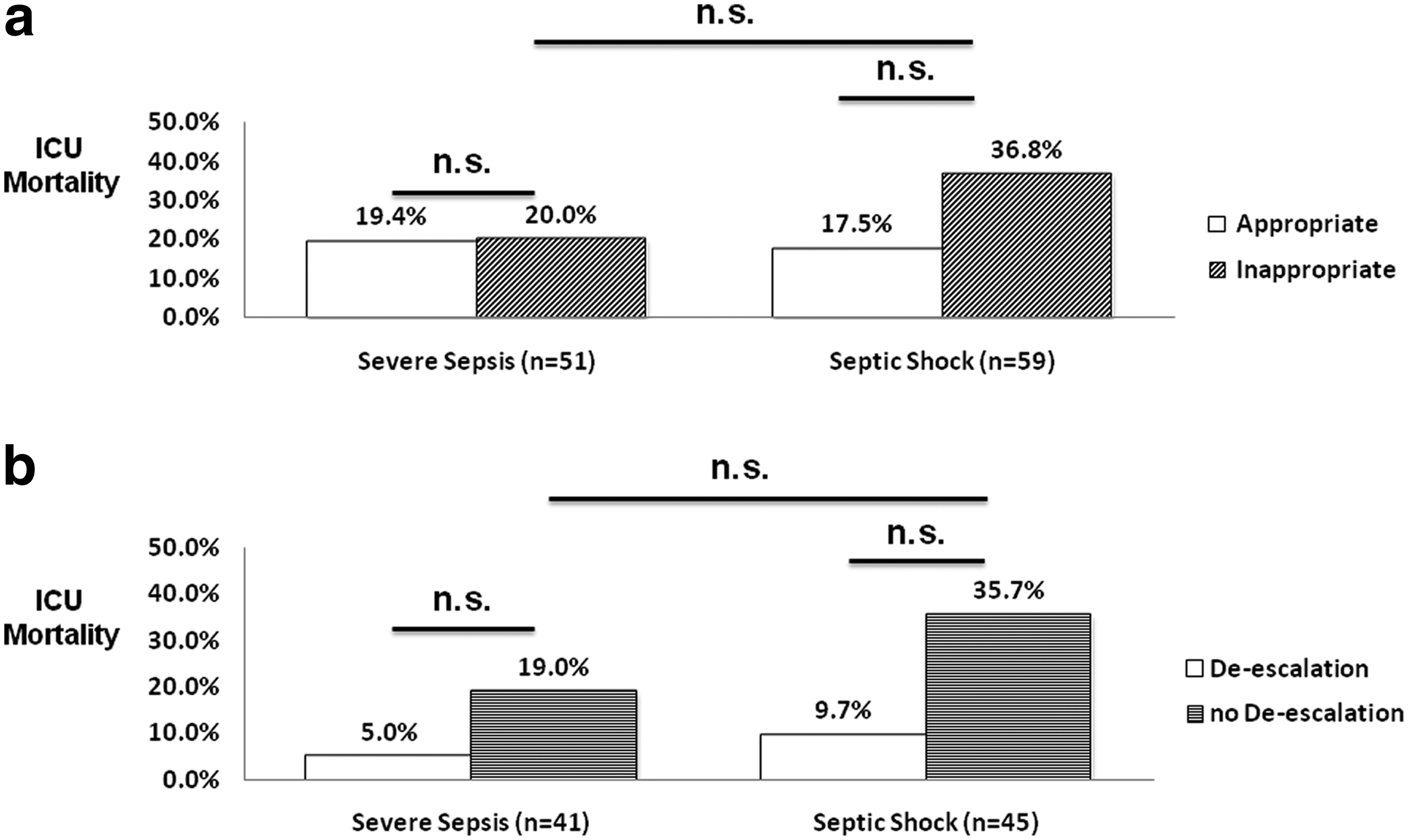
The effect of appropriate empiric antibiotic therapy and de-escalation on ICU mortality rates:
De-escalation and mortality
Among the patients with appropriate empiric antibiotic administration, the de-escalation group presented lower mortality rates of 5.0% for severe sepsis and 9.7% for septic shock. The mortality rates for the no de-escalation group were 19.0% and 35.7%, respectively (Fig. 5b).
Figure 6 shows the rates of de-escalation for frequently used antibiotics. Carbapenems were de-escalated most frequently, 64.0% when used for septic shock and 46.2% for severe sepsis patients.
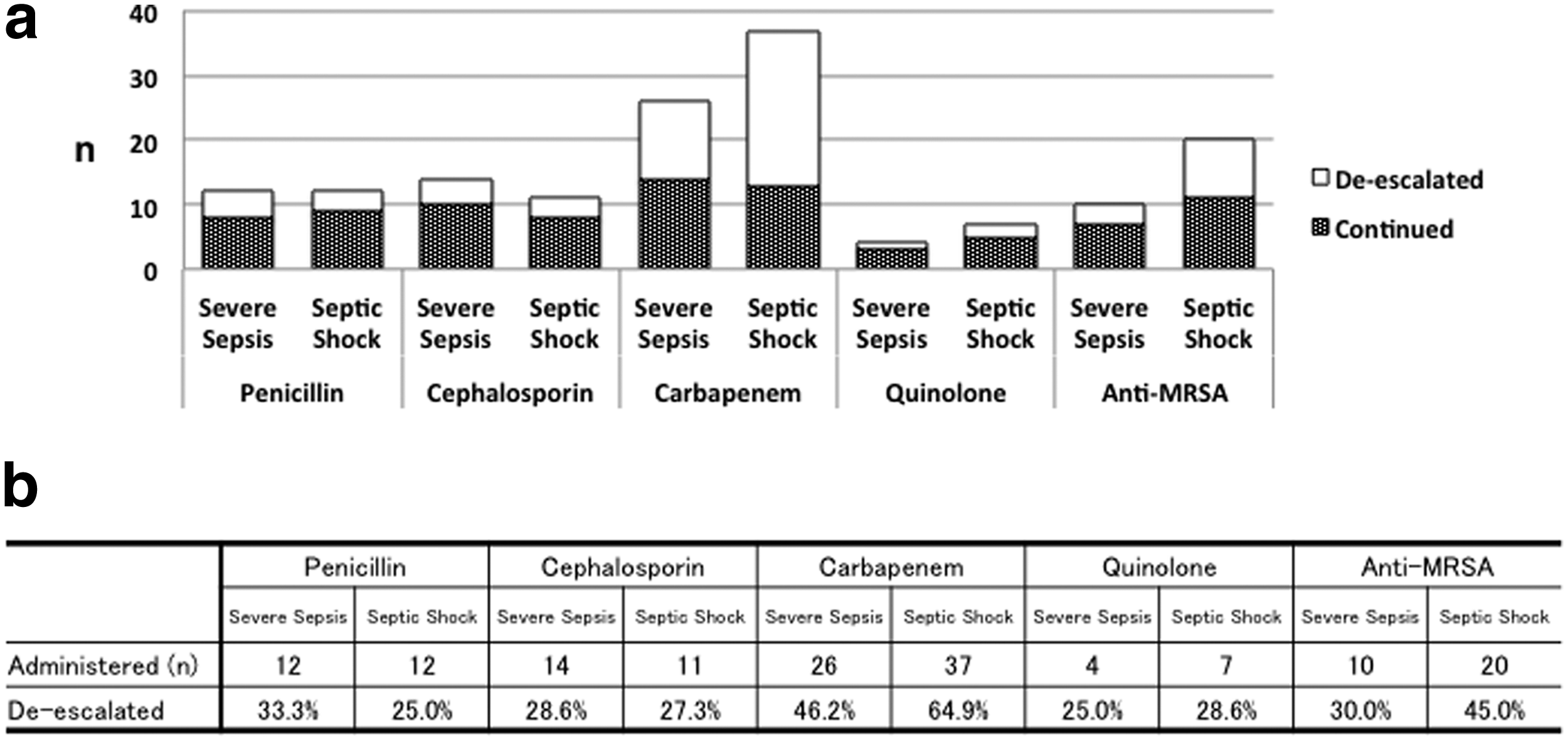
Rate of de-escalation for frequently used antibiotics:
Discussion
Recent guidelines for treatment of sepsis recommend the use of empiric antibiotic therapy for better survival [2,7,8,13]. Selecting an effective antibiotic empirically requires an accurate prediction of the site of the infection and the causative microorganism. The selection is complicated by the recent trend of infections caused by multi-drug-resistant organisms even in the community setting [11]. The selection of empiric antibiotics observed in the present study presented different patterns for the different foci of infections, suggesting the guideline oriented selections by the attending physicians [9]. The rates of appropriate therapy as the result of the selections were feasible for this population of patients.
There is a growing trend for the use of carbapenems as the first-line antibiotic for sepsis, because of their broad coverage, including anaerobic bacteria, and their strong bactericidal activity [14]. However, this has led to the prevalence of multi-drug-resistant bacteria in the hospital and community settings [14]. Guidelines call for the limited the use of carbapenems for patients in severe conditions for whom the success of the initial antibiotic therapy is vital for survival, or for pathogens proven non-susceptible to other antibiotics by culture [2,14,15]. The rate of carbapenem use was 57.3% overall for the present study, reflecting the selection of a reliable antibiotic by the doctors as the initial treatment for severe sepsis and septic shock patients. However, carbapenems were most frequently de-escalated in both septic shock and severe sepsis patients, which represents that carbapenems were used properly and effectively, under the premise of de-escalation. The patients treated with aminoglycosides and anti-MRSA antibiotics presented greater mortality rates, reflecting their use for patients with greater severity [5,6]. On the other hand, the recently developed extended-spectrum penicillins [15,16] presented possible survival benefit for the population of the present study.
The rate of multi-drug-resistant infections was not as high as expected [17], and also not related to greater mortality rates, consistent with previous reports [15,18]. Because we did not differentiate between community-acquired and hospital-acquired infections, the present data consist of both. The mixture of the hospital-acquired and community-acquired infection patients may have accounted for the relatively low rate of the resistant organism related infections.
Mortality rates were greater in patients who had inappropriate empiric therapy, those who were not de-escalated, and those who had multi-drug-resistant infections. This trend was also consistent with previous reports [13,19]. These observations may be interdependent, because the greater incidence of resistant infections will likely contribute to a greater rate of inappropriate empiric therapy, and thus the lower rate of de-escalation.
This study has several limitations. First, because the patients are from a single university hospital, the patients enrolled may be biased towards more intensive treatment on admission. The second limitation is the relatively small number of the study population. A larger population is required for more generalized analyses and recommendations. Thirdly, the retrospective nature of the study disables the possibility to preclude bias from other treatment modalities. Although most of the treatments are carried out according to the decisions made through clinical conferences, treatment protocols and available medical resources may have varied slightly during the study period.
Conclusion
Empiric antibiotic therapy was acceptable for severe sepsis and septic shock patients treated in the ICU. The appropriate selection of empiric antibiotics was related to a greater rate of de-escalation and better survival. Risk of multi-drug-resistant bacterial infection was not as high as expected, but will need further attention in the future.
Footnotes
Author Disclosure Statement
The authors have no commercial associations to disclose that might create a conflict of interest concerning this manuscript.