
Abstract
Abstract
Background:
Ceftaroline is a broad-spectrum cephalosporin antibiotic with activity against drug-resistant bacteria, including strains of methicillin-resistant Staphylococcus aureus (MRSA), and may be useful to prevent and treat ventriculostomy-related infections (VRIs). The purpose of this study was to analyze the pharmacokinetics and pharmacodynamics of prophylactic ceftaroline in neurosurgical patients with an external ventricular drain (EVD).
Methods:
Adult patients in the neurosurgical intensive care unit with an EVD were given prolonged prophylaxis with ceftaroline. Serum and cerebral spinal fluid (CSF) were obtained simultaneously at 2, 6, and 12 h after initiation of the fourth dose of ceftaroline and concentrations were measured by a liquid chromatography tandem mass spectrometry assay. Time-kill curves against isolates of coagulase-negative S. aureus, methicillin-sensitive S. aureus, MRSA, and Streptococcus pneumoniae were determined in serum and CSF at each collection time point.
Results:
A total of five patients with a mean age of 63 y and mean weight of 83 kg were enrolled. The mean CSF:serum penetration ratios of ceftaroline were 0.005 (0.5%), 0.021 (2.1%), and 0.043 (4.3%) at 2, 6, and 12 h, respectively. The mean ceftaroline exposure ratio area under the curve (AUC)csf/AUCserum) was 0.011 (1.1%). Bactericidal activity at each collection time point was observed against each strain of staphylococci from serum samples and a penicillin-sensitive strain of S. pneumoniae from CSF samples.
Conclusion:
This investigation suggests that ceftaroline could have clinical utility for the prevention of VRIs in patients with EVDs.
T
The use of prophylactic antibiotics may mitigate VRIs although studies evaluating their effectiveness remain conflicting and are at times contradictory [3]. In a recent systematic review of randomized clinical trials and observational studies, Sonabend et al. [4] found a protective effect (risk ratio: 0.32; 95% confidence interval [CI]: 0.18–0.56) of prophylactic systemic antibiotics when used throughout the duration of external ventricular drainage. The authors note that available data are heterogeneous and of suboptimal quality. Moreover, the management of prophylactic antibiotics in patients with EVDs varies between institutions and among specialists within a medical center [5]. Options for prophylaxis include peri-procedural as well as prolonged systemic antibiotics with either a ß-lactam (e.g., cefazolin) or vancomycin [6]. Prophylaxis with vancomycin is usually reserved for hospitals in which methicillin-resistant Staphylococcus aureus (MRSA) and coagulase-negative staphylococci are common causes of VRIs or in patients allergic to cephalosporins [7].
Ceftaroline, a new parenteral cephalosporin with broad-spectrum antibacterial activity including MRSA, may be a suitable alternative agent for prevention and treatment of VRIs in patients with EVDs. In addition to good activity against multi-drug–resistant gram-positive cocci (MDR-GPC) and many enterobacteriaceae, this antibiotic has low protein binding and exhibits good tissue penetration [8]. In vivo efficacy has been established with ceftaroline in animal models of endocarditis, osteomyelitis, pneumonia, and meningitis and human clinical trials of pneumonia and complicated skin infections [9].
Additional studies of ceftaroline for prevention and treatment of nosocomial bacterial meningitis caused by MDR-GPC are warranted because few alternatives to vancomycin are available [2]. In this investigation, we analyzed the pharmacokinetics and pharmacodynamics of prophylactic ceftaroline in neurosurgical patients with an EVD.
Patients and Methods
This was a non-randomized study conducted in a neurointensive care unit at a community/teaching hospital affiliated with Michigan State University (MSU). The study was approved by the hospital Investigation Research Committee and written informed consent was obtained for each subject (patient or spouse). Inclusion criteria for these patients (age ≥18 y) included the presence of an indwelling EVD, the absence of infection, and eligible to receive ceftaroline prophylaxis. Exclusion criteria included patients with allergy to penicillins or cephalosporins, those receiving additional antibiotics, and pregnancy. Initial patient demographic data were collected upon enrollment into the study.
All patients received 1-h intravenous infusions of ceftaroline twice daily for the duration of EVD placement. The dose of ceftaroline was 600 mg for patients with an estimated creatinine clearance (CrCl) >50 mL/min (Cockcroft-Gault formula), 400 mg for an estimated CrCl >30 to ≤50 mL/min, and 300 mg for an estimated CrCl ≥15 to ≤30 mL/min. After at least two doses of ceftaroline, blood and CSF (3–6 mL) samples were obtained simultaneously at 2, 6, and 12 h after the initiation of an infusion. The drip chamber collecting CSF was emptied 30–60 min prior to sampling. After centrifugation, these samples were stored at −70°C until being assayed.
Quantification of ceftaroline in human serum and CSF specimens was developed and validated by Keystone Bioanalytical Corporation (North Wales, PA) using a Turbo Inospray liquid chromatography-tandem mass spectrometry (LC/MS/MS) assay [10]. This method uses protein precipitation by methanol to isolate the analytes from plasma. After protein precipitation, the supernatant is diluted further with a solution of ammonium formate in water. The entire extraction is performed rapidly (less than 90 min) and in an ice bath to minimize degradation or conversion of the analytes. A 50-mcL sample volume is used and a deuterated (d3) form of each analyte is used as the respective internal standard. Precision and accuracy of the method was established based on five batches run over at least a 3-d period. Each precision and accuracy batch contained six replicate quality control samples at four concentrations. Precision and accuracy was also established at the lower limit of quantification. The inter-assay coefficient of variation for the quality controls ranged from 2.14%–3.3%. Concentrations (9 samples) below 50 ng/mL were obtained by extrapolation of the standard curve (50–50,000 ng/mL).
The pharmacokinetic parameters of ceftaroline in the serum and CSF were calculated for individual subjects using standard non-compartmental methods with Phoenix WinNonlin Version 6.3 (Pharsight Corporation, Cary, NC). Parameters were calculated at steady state using the area under the curve (AUC) and area under the first moment curve (AUMC) from the time of dosing to the time of the last observation for both serum and CSF. Clearance (Cl) in the serum was calculated as dose/AUCserum. Volume of distribution at steady state (Vss) in the serum was calculated as (dose*AUMCserum)/AUCserum2). The elimination rate constant (k) and half-life in serum and CSF were derived using Cl/Vss and 0.693/k, respectively. The percent meningeal exposure was derived by the AUCCSF:AUCserum ratio.
Clinical (MSU) and laboratory American Type Culture Collection (ATCC) isolates of staphylococcus and a laboratory strain (ATCC) of Streptococcus pneumoniae were used to analyze the anti-microbial activity of ceftaroline in serum and CSF. The minimum inhibitory concentrations (MIC) of ceftaroline for these bacteria was determined by microbroth dilution and E test methodology according to the Clinical Laboratory Standards Institute (CLSI) [11]. Each serum and CSF sample was tested against these organisms by a modification of the time-kill method described in the CLSI guidelines [12]. Two hundred twenty-five microliters of each serum sample was plated on microtiter plates and inoculated with the bacterial strains. To prepare the inoculum, staphylococcus colonies were suspended in cation-supplemented Mueller-Hinton broth and streptococcus colonies were suspended in cation-supplemented Mueller-Hinton broth with 5% lysed horse blood. Twenty-five microliters of inoculum was used to inoculate each serum sample. Viability counts of each culture were carried out at 0, 2, 6, and 24 h after inoculation. Sampling was done by removing a 5 mcL aliquot from each sample and serially diluting them 10-fold in media to minimize antibiotic carryover. Ten microliter aliquots of both the undiluted and diluted samples were plated on Mueller-Hinton plates (staphylococci) or blood agar plates (streptococci) and colonies counted after 24 h of incubation at 35°C. Time-kill assays were analyzed by determining the number of bacteria (log10 CFU/mL) at 2, 6, and 24 h, compared with counts at 0 h. The range of quantification was 20–200 CFU/mL. Growth controls were included in each experiment. Geometric means of bacterial concentrations (log10 CFU/mL) were used to determine the difference in log-kill at 24 h.
Results
Five adult neurosurgical patients (three males and two females) were enrolled in this study. Their individual demographics are listed in Table 1. These patients had a mean age of 63 y and weight of 83 kg. Two patients had traumatic brain injury, one had a subarachnoid hemorrhage, one had an intra-cerebral hemorrhage, and one a had brain metastasis. All patients enrolled required CSF drainage because of acute hydrocephalus. None of these patients were being treated for an infection during the collection of sera and CSF for this study and all tolerated ceftaroline prophylaxis (range, 2.5–9 d) without an adverse event. Moreover, none of these patients developed Clostridium difficile infection associated with ceftaroline therapy.
BMI=body mass index; CrCl, creatinine clearance.
The mean±standard deviation (SD) steady-state serum and CSF pharmacokinetic parameters for ceftaroline in these five patients are shown in Table 2. The mean (±SD) CSF-to-serum concentration penetration was 0.5%±0.5%, 2.1%±1.8%, and 4.4%±6.0% at 2, 6, and 12 h after the start of a 1-h infusion, respectively. The mean (±SD) ceftaroline exposure ratio (AUCCSF/AUCserum) was 0.011±0.01 or 1.1%±1.0%.
Cmax=concentration at 2-h after start of ceftaroline infusion; Cmin=concentration at 12-h after start of infusion; AUC=area under concentration-time curve over the dosing interval (0–12 h); Vss=volume of distribution at steady-state; T½=elimination half-life; Cl=clearance.
The serum time-kill curve analyses found that ceftaroline exhibited bactericidal (>3 log kill) activity at each sample time point (2, 6, and 12 h) against three staphylococcal isolates that included a strain of methicillin-sensitive S. aureus (MIC=0.19 mg/L), a strain of MRSA (MIC=0.5 mg/L), and a coagulase-negative staphylococcal (CNS) isolate (MIC=0.19 mg/L). The time-kill curves for these bacteria using trough (Cmin) serum concentrations of ceftaroline are shown in Figure 1. Antibacterial activity against these isolates of staphylococci was not observed with the CSF concentrations obtained from our study patients. Bactericidal activity in CSF at each sample time was observed against a strain of S. pneumoniae (MIC=0.023 mg/L). In contrast to the staphylococcal isolates, this pneumococcal isolate had a MIC below the mean concentrations of ceftaroline measured in CSF (Fig. 2).
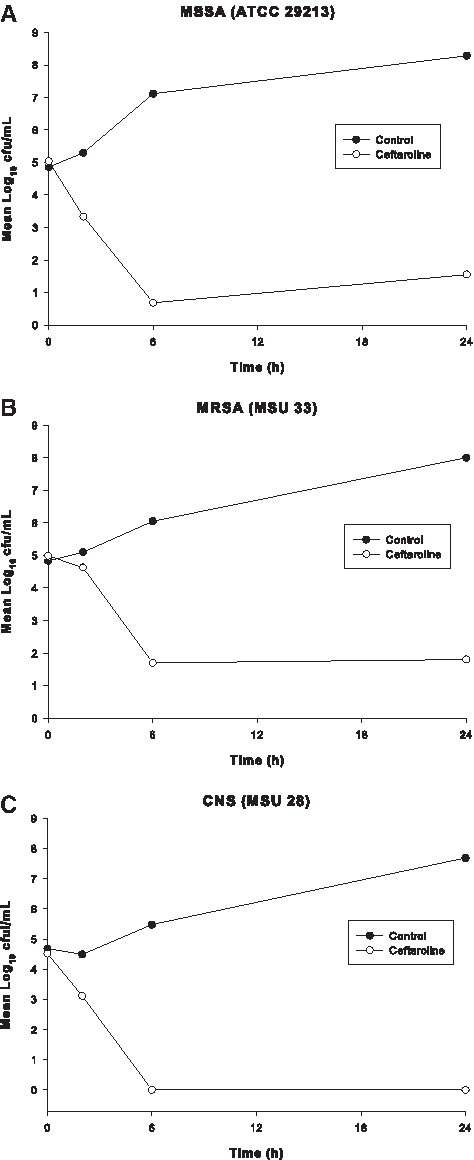
Time-kill curves with trough (12 h) concentrations of ceftaroline in serum against staphylococcal isolates.
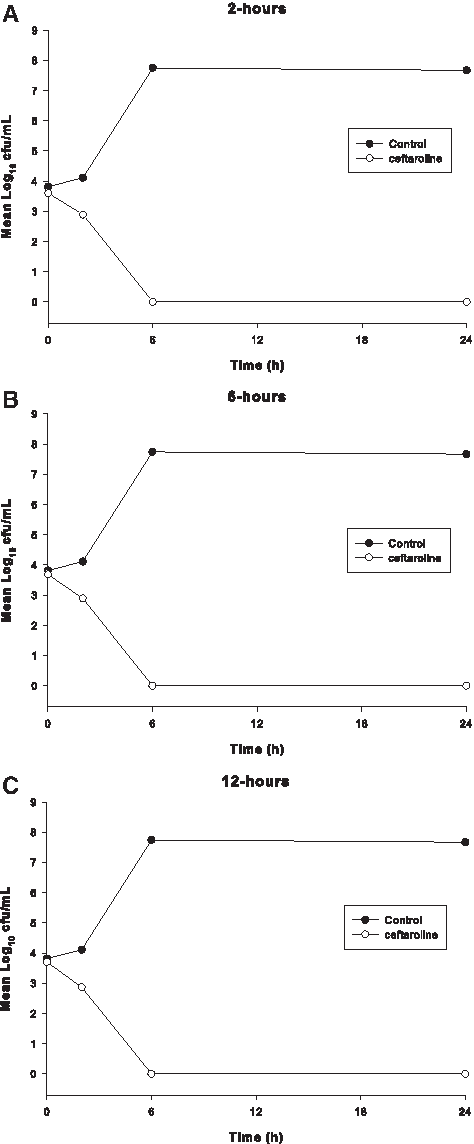
Time-kill curves with ceftaroline in cerebrospinal fluid (CSF) against a strain of Streptococcus pneumoniae (ATCC 49619) at each collection time.
Discussion
Although the incidence of infection after EVD placement is low, this complication is an important cause of patient morbidity. In addition to being associated with a poor outcome, these infections lead to increased length of stay in the neurosurgical intensive care unit and increased overall hospital costs. Antibiotics have been used extensively for many years to prevent VRIs, although unequivocal support for the efficacy of this tactic does not exist [3]. If used for prophylaxis, the choice of an antimicrobial agent should be directed against the most likely infecting organisms. For neurosurgical procedures, antibiotics with good activity against staphylococci (e.g., cefazolin, vancomycin) are usually recommended [6]. If vancomycin is chosen for a procedure in which gram-negative bacteria are also likely pathogens, an additional agent with activity against these organisms should be added [13].
The antimicrobial spectrum of ceftaroline is comparable to a combination of cefazolin and vancomycin [8]. Furthermore, this bactericidal cephalosporin has a steady-state elimination half-life of almost 3 h and is well tolerated [9]. These attributes make this agent a viable choice for surgical prophylaxis of neurosurgical procedures such as placement of an EVD [6]. Because EVDs are often in place for several days, it would be preferable to have therapeutic concentrations of the prophylactic antibiotic present in serum and tissue throughout its placement. Our study of time-kill curves revealed that serum from patients, after standard doses of ceftaroline, produced bactericidal activity against different strains of staphylococci. Moreover, this anti-microbial activity was observed throughout the 12-h dosing interval (Fig. 1).
Treatment of VRIs requires antimicrobial agents that are active against likely organisms associated with these infections as well as have the ability to achieve therapeutic concentrations in CSF. The CSF penetration of hydrophilic agents, such as cephalosporins, depends upon the opening of tight junctions in the blood brain barrier (BBB). During meningitis, there is a separation of these tight junctions and increased permeability of the BBB. These changes result in a significant increase (∼5 times) in the CSF penetration of ß-lactam antibiotics [14]. In a rabbit meningitis model, the CSF exposure (AUCCSF/AUCserum) of ceftaroline was approximately 15% into inflamed meninges and approximately 3% into uninflamed meninges [15]. In our study of patients with uninflamed meninges, CSF exposure was approximately 1%. The diminished CSF penetration of ceftaroline observed in our patients compared with other cephalosporins with low protein binding, such as cefotaxime, may be the result of its greater molecular weight (ceftaroline, 681 Da; cefotaxime, 455 Da) [16].
The relative lack of CSF immunoglobulin, combined with local complement deficiency, contributes to a regional host immunodeficiency during bacterial meningitis [17]. These conditions result in inefficient phagocytosis and rapid bacterial multiplication. Therefore, optimal antibiotic treatment requires that the drug have a bactericidal effect in CSF [18]. The bactericidal activity of ß-lactam antibiotics is dependent on the time their concentrations exceed the MIC (T>MIC) for the infecting organism [19]. In a pneumococcal meningitis model in rabbits, sterilization of CSF was achieved only when the T>MIC was 95%–100% of the ceftriaxone dosing interval [20]. Ceftaroline has also been shown to provide bactericidal activity against S. pneumoniae isolates in an experimental rabbit meningitis model [21]. Ceftaroline was slightly superior to ceftriaxone against a penicillin-sensitive strain and superior to the combination of ceftriaxone and vancomycin against a penicillin-resistant strain. We also observed bactericidal activity in CSF for the entire 12-h dosing interval of ceftaroline against a penicillin-sensitive strain of S. pneumoniae (Fig. 2). Bactericidal activity in CSF was not observed against staphylococcal isolates in our study.
Conclusion
In summary, standard dosing of ceftaroline in patients with EVDs provided sustained serum bactericidal activity against staphylococcal isolates. These findings suggest that this cephalosporin could have clinical utility to prevent VRIs and warrant further clinical trials. Conversely, the concentrations in CSF did not kill Staphylococcus species and greater concentrations of ceftaroline would be required to treat ventriculomeningitis due to Staphylococcus. This is conceivable because the daily dose of most ß-lactam antibiotics can be increased without a high rate of serious side effects [13]. At present, ceftaroline doses of 900 mg every 12 h for 10 d and a single dose of 1,500 mg have been shown to be well tolerated in healthy subjects [10,22].
Footnotes
Acknowledgments
The authors wish to thank the physician assistants and nurses in the Neuro-ICU at Sparrow Hospital for their assistance in conducting this study and Keystone Bioanalytical, Inc. for quantitative analysis of ceftaroline. This study was supported by the Michigan State University/Sparrow Hospital Infectious Diseases Fellowship Program. No additional funding was obtained.
Author Disclosure Statement
No competing financial interests exist.