
Abstract
Abstract
Introduction:
In pancreatic surgery pre-operative biliary drainage (PBD) is associated with bacteribilia, which increases the risk for surgical site infections (SSIs).
Methods:
This study is a retrospective observational cohort design that compared micro-organisms of intra-operative bile duct cultures with micro-organisms of SSIs after pancreaticoduodenectomy.
Results:
From January 2004 until December 2010, 887 patients underwent pancreaticoduodenectomy or hepaticojejunostomy for benign and malignant peri-ampullary lesions. Surgical site infections occurred in 10% (87/887). Cultures of SSIs with corresponding intra-operative bile duct cultures were available for 59 patients. Sixty-four percent (38/59) had undergone PBD. Pre-operative biliary drainage was associated with positive intra-operative bile duct cultures in 95% (36/38), versus 48% (10/21; p≤0.001). The correlation of SSIs with intra-operative bile duct cultures was 59% (35/59). There was a significant association between the micro-organisms cultured from SSIs and the corresponding bile duct cultures for Enterococcus spp., Escherichia coli, Klebsiella pneumoniae, methicillin-resistant Staphylococcus aureus (MRSA), Enterobacteriaceae with extended spectrum ß-lactamase (ESBL), and Candida spp.
Conclusion:
After pancreaticoduodenectomy, SSIs are often caused by the same micro-organisms that are present on intra-operative bile duct cultures, especially after PBD. Therefore, intra-operative bile duct cultures should be performed routinely to adjust the antibiotic prophylaxis according to the local hospital surveillance data.
I
Usually bile ducts are sterile. In biliary obstruction approximately 25% of bile ducts are colonized, and the rate increases to more than 70% after endoscopic retrograde cholangiography (ERC), whereas pre-operative biliary drainage (PBD) with an endoscopically placed bile duct stent during ERC leads to almost 100% of biliary tract colonization [4,5]. Because operations on jaundiced patients have been associated with poor outcome, the aim of PBD is to reduce post-operative morbidity and mortality in patients undergoing surgery for malignant obstructive jaundice. However, studies analyzing the benefits of PBD had conflicting results, and today, there is evidence that the rate of post-operative infectious complications is negatively affected by the use of endoscopically placed bile duct stents [6,7]. Nonetheless, PBD cannot always be avoided, especially in deeply jaundiced patients with cholangitis, or if patients have to be referred to specialized pancreatic centers.
Thirty years ago there was no microbiologic correlation between intra-operative bile duct cultures and post-operative SSIs in patients who underwent biliary surgery. Most bile duct cultures showed Escherichia coli, whereas most SSIs were caused by Staphylococcus spp. [8]. Today, bile bacteriology changed toward more opportunistic species, but so far no study correlated the bacteriology of post-operative SSIs with intra-operative bile duct cultures with a precise determination of bacteriologic data [9].
Thus, the aim of the present study was to investigate if post-operative SSIs are caused by the same micro-organisms that had been identified from intra-operative bile duct cultures that were performed routinely after bile duct transection in patients who underwent pancreaticoduodenectomy.
Patients and Methods
The study uses an observational cohort design. All patients who underwent pancreatic surgery at the Department of Surgery, St. Josef Hospital Bochum, Germany, were entered into a prospectively collected database. The charts, operative protocols, and microbiologic culture results of all patients who underwent pancreatic head resection or palliative bypass procedures both for malignant or benign diseases of the pancreatic head, the distal bile duct, the duodenum, or the ampulla of Vateri were analyzed for study purposes. Patients who underwent distal pancreatectomy, operations for acute necrotizing pancreatitis, duodenum-preserving pancreatic head resection, or all other procedures without bile duct transection were excluded from the analysis. Microbiologic cultures were screened for bile duct culture results and culture results originating from post-operative SSIs.
Immediately after bile duct transection intra-operative bile duct cultures were collected from all patients who had a hepaticojejunostomy after pancreatic head resection or a palliative surgical bypass procedure. Microbiologic analyses consisted of aerobic and anaerobic cultures for 72 h and 96 h at 37°C. Routine bile duct transection was performed approximately 1 cm distal to the common hepatic duct bifurcation. Reconstruction after pancreatic head resection was performed with an end-to-side pancreaticojejunostomy and an end-to-side hepaticojejunostomy into the same jejunal loop. In patients with a palliative hepaticojejunostomy bile duct transection was performed in the same fashion and patients underwent an end-to-site hepaticojejunostomy with an isolated Roux-en-Y-loop. All patients had two flat silicon drains placed near the pancreatic and the bilioenteric anastomosis. After bile duct transection all patients had a retrograde bile duct flushing with warm saline solution. All patients received routine antibiotic prophylaxis including a third-generation cephalosporin or a fluoroquinolone in case of allergy to penicillin and metronidazole intravenously at least 30 min before abdominal incision. Pre-operative biliary drainage was performed routinely with a straight plastic stent using a standard procedure. During ERC patients did not receive routine antibiotic prophylaxis.
A post-operative SSI was defined as an apparent infection with purulent discharge at the incision site within 30 d after surgery involving the skin, subcutaneous tissue, or muscle located above the fascial layer with spreading cellulitis and lymphangitis that required surgical incision opening without re-closure. The diagnosis of a post-operative SSI was based on the Guideline for Prevention of Surgical Site Infection by the U.S. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee [10]. Complications other than SSIs were defined as described previously [11]. If SSIs were accompanied by partial or complete dehiscence of the fascial layers, patients underwent re-operation for secondary fascial closure. Vacuum therapy for the treatment of post-operative SSIs was not performed routinely. After surgical incision opening a first culture from the SSI was taken in a standardized manner. Microbiologic analyses consisted of aerobic and anaerobic cultures for 72 h and 96 h at 37°C.
Isolates of micro-organisms out of SSIs and bile ducts were analyzed for their species and antibiotic susceptibility including analyses for antibiotic resistance. Antibiotic resistance was defined as growth inhibition in the presence of the antibiotic substrate tested. Post-operative SSI culture results were matched with intra-operative bile duct culture results for all patients with post-operative SSIs.
All patients had given their informed consent before interventions and abdominal surgery. The study was reviewed with respect to the ethical conduct of research by the local ethical authority.
Statistical Analyses
Univariate analyses of variables were performed with the χ2 test and with Fisher exact test. Student t-test was used for equality of means. Otherwise Wilcoxon test was used, when appropriate. A p value of≤0.05 was considered statistically significant. All statistic analyses were performed with SPSS software version 18.0 (SPSS, Chicago, IL).
Results
During a period of 84 mo, from January 2004 until December 2010, 1,705 patients underwent pancreatic surgery for both malignant and benign diseases of the pancreas, the duodenum, the distal bile duct, or the ampulla of Vateri at the Department of Surgery, St. Josef Hospital Bochum, Ruhr University, Germany. Figure 1 shows the CONSORT diagram for the group of patients who was available for the final evaluation. Eight hundred eighteen patients underwent operations without bile duct transection and were excluded. Eight hundred eighty-seven patients had bile duct transection during pancreaticoduodenectomy or palliative surgical bypass procedures. Among those, 10% (87/887) developed post-operative SSIs. Twenty-eight patients were excluded from the analysis because culture results from SSIs or bile duct culture results were not available for the final evaluation. From the remaining 59 patients with post-operative SSIs, a culture from the SSI with a corresponding intraoperative bile duct culture was available (Fig. 1).
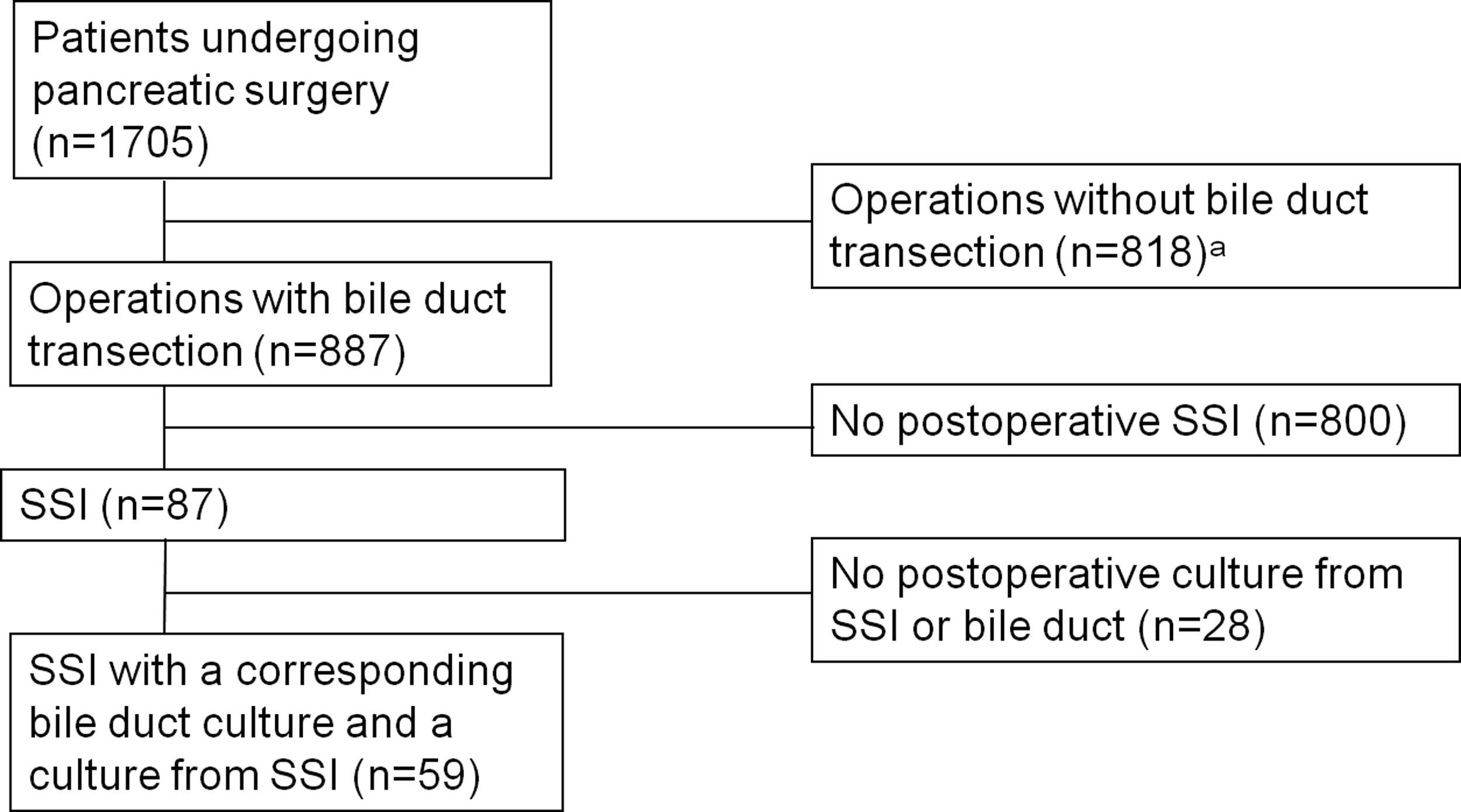
Consolidated Standards of Reporting Trials (CONSORT) diagram. The schematic illustrates the study design for patient disposition with the final collective available for evaluation. aDistal pancreatectomy (n=206), exploration (n=227), gastroenterostomy (n=85), pseudocystojejunostomy (n=39), duodenum-preserving pancreatic head resection (n=59), ampullary resection (n=16), operations for necrotizing pancreatitis (n=53), pancreatic segment resection (n=21), other operative procedures (n=112). SSI=surgical site infection.
Overall 66% (588/887) of patients underwent surgery for a malignant tumor, whereas 34% (299/887) were operated on for benign diseases. There was no significant difference in SSIs between patients with benign tumors (11%, 34/299) versus malignant tumors (9%, 53/588; p=0.313). The patient collective available for the final evaluation showed a comparable distribution with 61% (36/59) malignant tumors and 39% (23/59) benign diseases. Demographic details of the included patients are summarized in Table 1. The rate of SSIs was 9% (23/247) for patients who underwent bypass procedures and 10% (64/640) for patients who underwent resections (p=0.779).
pp=pylorus preserving; PBD=preoperative biliary drainage; SD=standard deviation.
Complications other than SSIs
Fourteen percent (8/59) of patients developed fascial dehiscence requiring operative revision with secondary fascial closure. Five percent (3/59) of patients had an intra-abdominal abscess that required interventional drainage; 5% (3/59) of patients developed delayed visceral hemorrhage that required a re-laparotomy; 3% (2/59) of patients had a grade B pancreatic fistula that was managed conservatively; and one patient (2%; 1/59) had a grade C bile leak that required a re-laparotomy. General complications that required intensive care unit re-admission included one patient (2%; 1/59) with sepsis syndrome, another patient had myocardial infarction (2%; 1/59), and another patient had pneumonia (2%; 1/59). Overall the mortality was 8% (5/59), including all three patients with delayed visceral hemorrhage, the patient with pneumonia, and the patient with a post-operative bile leak.
Pre-operative biliary drainage
The mean time for biliary drainage was 4 wks (range, 1–10 wks). The mean pre-operative bilirubin serum concentration in patients with a post-operative SSI was 1.1±0.9 mg/dL in patients with PBD, whereas it was 1.5±3.0 mg/dL for patients without PBD (p=0.674). The mean serum bilirubin serum concentration before endoscopic retrograde cholangiopancreatography (ERCP) and drainage in patients with a post-operative SSI was 6.8±6.7 mg/dL. There was a significant association between PBD and bacteribilia. Ninety-five percent (36/38) of patients who had undergone PBD had colonized bile ducts, whereas the rate was 48% (10/21) without PBD (p≤0.001).
Intra-operative bile duct culture results
In 78% (46/59) bile duct cultures were positive, whereas 22% (13/59) of bile duct cultures remained sterile. In 29% (17/59) one species could be identified, whereas polymicrobial colonization was found in 49% (29/59). The most frequent micro-organisms in intra-operative bile duct cultures were Enterococcus spp. in 53% (31/59), Escherichia coli in 27% (16/59) and Enterobacter cloacae in 14% (8/59). Bile duct cultures with methicillin-resistant Staphylococcus aureus (MRSA) were found in 5% (3/59), Pseudomonas aeruginosa was found in 5% (3/59), and Candida spp. in 7% (4/59), whereas there were no patients with coagulase-negative Staphylococcus spp. or Staphylococcus epidermidis. In 7% (4/59) bile duct cultures showed Enterobacteriaceae (Escherichia coli and Klebsiella pneumoniae) with extended spectrum ß-lactamase (ESBL).
Post-operative culture results of SSIs
Overall 83% (49/59) had positive cultures from post-operative SSIs, whereas in 17% (10/59) the cultures remained sterile. In 44% (26/59) cultures of SSIs showed one species, whereas 39% (23/59) of cultures from SSIs were polymicrobial, growing two or more different micro-organisms. The most frequent micro-organisms in post-operative SSIs were Enterococcus spp. in 41% (24/59), Escherichia coli in 17% (10/59), and MRSA in 12% (7/59). In 7% (4/59) of SSIs Enterobacter cloacae was found, Klebsiella pneumoniae was found in 4% (2/59), Pseudomonas aeruginosa in 7% (4/59), Candida spp. in 5% (3/59), coagulase-negative Staphylococcus spp. in 9% (5/59), and Staphylococcus epidermidis in 7% (4/59). In 7% (4/59) SSIs showed Enterobacteriaceae with ESBL (Escherichia coli and Klebsiella pneumoniae).
Correlation of bile duct cultures with post-operative SSIs
Figure 2 illustrates the frequency of the different micro-organisms in intra-operative bile duct cultures and in post-operative SSIs for each patient. The overall correlation of post-operative SSIs with intra-operative bile duct cultures showed that in 59% (35/59) at least one species isolated from the SSI was also present in the intra-operative bile duct culture. There was a significant association between the micro-organisms cultured from SSIs and the corresponding bile duct cultures for Enterococcus spp., Escherichia coli, Klebsiella pneumoniae, MRSA, and Candida spp., whereas there was no association for Pseudomonas aeruginosa, Enterobacter cloacae, coagulase-negative Staphylococcus spp. and Staphyloccocus epidermidis. There were four patients with Enterobacteriaceae with ESBL in SSIs: two patients with Escherichia coli and two patients with Klebsiella pneumoniae. Bile duct cultures of all four patients showed that the same species with ESBL had already been cultured from the intra-operative bile duct cultures (Fig. 2).
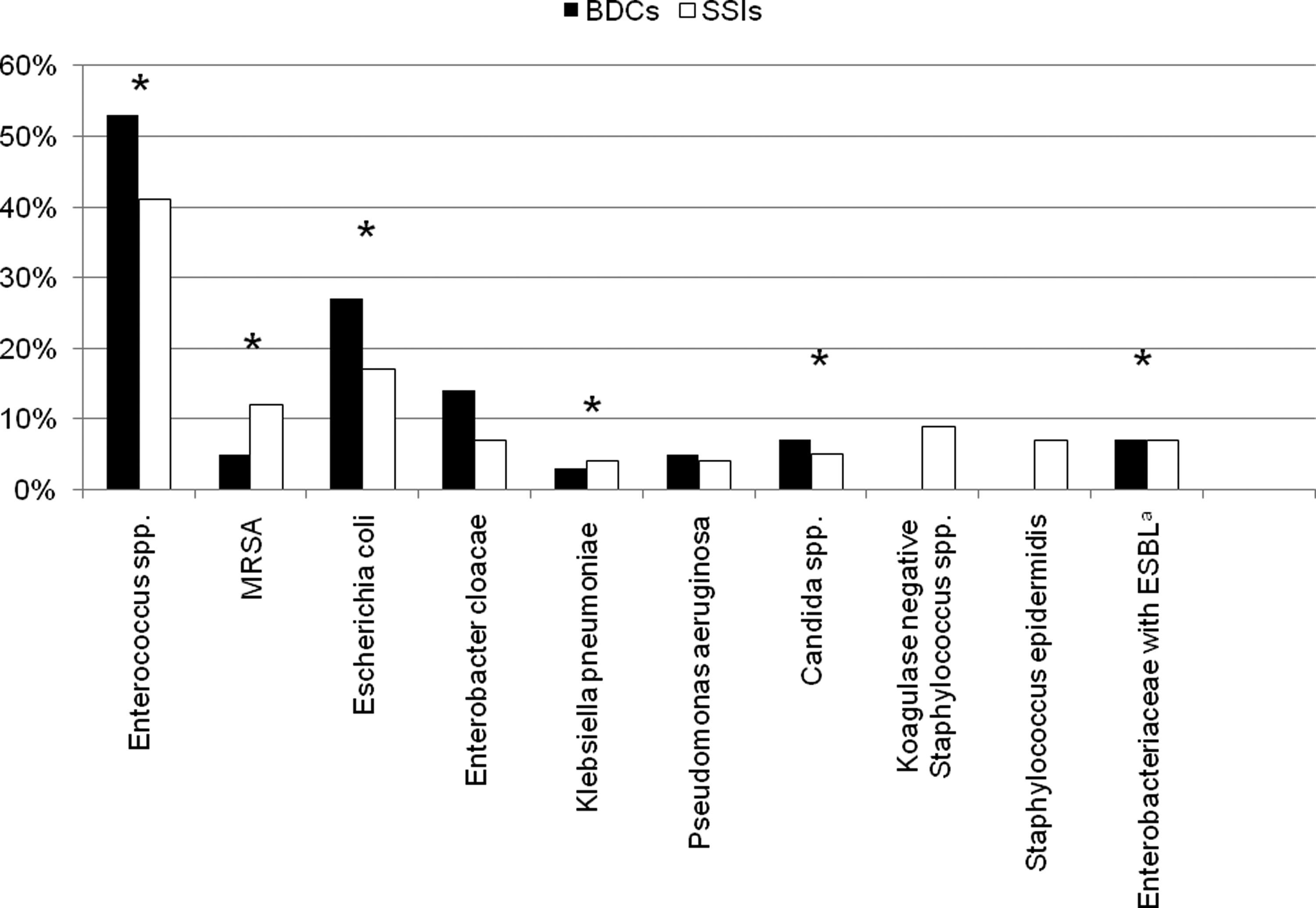
Micro-organisms in intra-operative bile duct cultures (BDCs) and in post-operative surgical site infections (SSIs). The figure results show the correlation between the micro-organisms of SSIs and bile duct cultures of each individual patient. *Significant association between the micro-organisms cultured from SSIs and the corresponding bile duct culture for the different micro-organisms (p≤0.05). aEscherichia coli (n=2), Klebsiella pneumoniae (n=2).
Discussion
Outcome of patients with post-operative SSIs
Post-operative SSIs are classified as minor surgical complications, but in patients with malignancies, especially pancreatic adenocarcinoma, the majority of patients require adjuvant or palliative chemotherapy, which is often delayed by post-operative SSIs. Post-operative SSIs predispose for a longer hospital stay with higher morbidity and mortality, a higher probability for hospital readmission and ICU stay, leading to higher health care costs [1].
Bile bacteriology and post-operative SSIs
Although the finding that colonized bile is associated with post-operative SSIs is not new, the present study has several important implications [12,13]. First, there was a clear association between the micro-organisms of SSIs with the corresponding intra-operative bile duct cultures. Earlier studies mostly documented the presence of micro-organisms in bile duct cultures and the presence of SSIs without differentiation of the micro-organisms responsible for post-operative SSIs or found no association between SSIs and intra-operative bile duct cultures [8,14]. Furthermore, in the present study, both cultures from SSIs and intra-operative bile duct cultures showed a high frequency of resistant opportunistic micro-organisms, especially Enterococcus spp.
In earlier studies investigating the predominant micro-organisms in bile duct cultures Escherichia coli and Klebsiella spp. were found to be the most common species, whereas most SSIs were caused by Staphylococcus spp. [15,16]. In recent years there has been a change in bile microbiology and antibiotic susceptibilities for patients with colonized bile toward more Enterococcus spp. and other opportunistic micro-organisms among patients with benign and malignant biliary tract diseases [9,17].
Positive intra-operative bile duct cultures have been associated with post-operative complications [18]. This is shown by the high rate of positive intra-operative bile duct cultures in patients without PBD, which was almost 50%, whereas the rate is usually less than 5% without ERC and ranges between 15% and 20% after ERC [5,13,18]. This finding emphasizes the effects of positive intra-operative bile duct cultures, especially if resistant opportunistic micro-organisms are present, whereas bile duct stenting does not necessarily increase the rate of surgical site infections [11].
Post-operative complications
In the present study, the rate of SSIs was 10%. The rate of SSIs after simple cholecystectomy is less than 5%, whereas the rate varies between 8% and 10% after biliary tract surgery and can be even 25% in patients undergoing surgery for cholangitis [3,19]. The rate of SSIs after pancreaticoduodenectomy is 17% for patients without PBD and 20% for patients who underwent PBD [20]. Thus, the overall rate of SSIs in the present study was low, whereas there was a high rate of patients with fascial dehiscence.
The highest risk for the development of a post-operative fascial dehiscence has been associated with deep post-operative SSIs [21]. In the present study, 14% (8/59) of patients required operative revision for secondary fascial closure, whereas usually the rate of post-operative fascial dehiscence is less than 1% [22].
Other typical infectious complications after pancreaticoduodenectomy such as cholangitis or intra-abdominal abscesses from a pancreatic or a bile leak were not compared with the bile duct microbiology, because often blood cultures remained sterile and most patients with an intra-abdominal abscess already received an antibiotic treatment before infectious material could be sent for culture after CT drainage [23,24].
Post-operative complications other than SSIs were within the range of studies for specialized pancreatic units, whereas the overall mortality was higher than recent results from the literature would suggest [25,26]. Thus, it is important to remind that this is the effect of a selection bias, because only patients with SSIs were included in the study. These patients have a higher mortality than patients without SSIs [1]. This is confirmed by recently published data originating from our institution that have shown mortality clearly below 5% [5,11].
Post-operative SSIs without corresponding bile duct cultures
In 41% of patients there was no correlation between SSIs and intra-operative bile duct cultures. Especially among patients with SSIs with susceptible Staphylococcus spp. these species could not be identified in intra-operative bile duct cultures. Furthermore, there were four patients with post-operative SSIs with MRSA without a corresponding bile duct culture. Obviously SSIs with these micro-organisms originated from an exogenous source, whereas most other species, especially Enterococcus spp., Escherichia coli, and Klebsiella spp. matched bile duct culture results [16].
Enterococcus spp. in post-operative SSIs
In the literature, the virulence of Enterococcus spp. is often questioned, because Enterococcus spp. are often found in polymicrobial cultures in combination with other micro-organisms. However, in the last decade it became clear that these species cause severe opportunistic infections, not only in patients with immune deficiency [27,28].
In the present study there was a clear association between post-operative SSIs and resistant micro-organisms in intra-operative bile duct cultures for patients with Enterococcus spp. Thus, pre-operative identification of patients with Enterococcus spp. would be helpful, because there is evidence that intra-operative coverage of Enterococcus spp. can reduce the rate of SSIs with Enterococcus spp., especially in a setting in which the incidence of Enterococcus spp. infections is high [29].
Antibiotic prophylaxis for patients after PBD
Surgeons should therefore question whether antibiotic prophylaxis for patients undergoing pancreatoduodenectomy should be adjusted according to local hospital surveillance data. For this purpose bile duct cultures should be taken during ERC or intra-operatively immediately after bile duct transaction.
In the present study and during earlier surveys we could show that patients who undergo PBD have a high rate of opportunistic micro-organisms and Enterococcus spp. [5,11]. Thus, opportunistic micro-organisms and Enterococcus spp. should be anticipated in patients who underwent PBD, whereas these micro-organisms are less frequent in patients without PBD. The question of whether adjusted antibiotic prophylaxis for patients who underwent PBD is able to reduce the rate of post-operative SSIs cannot be answered by the present study, however, the present data imply that such a study is needed.
Limitations
The present study has several limitations. First, this was a retrospective study that compared the micro-organisms of post-operative SSIs with the micro-organisms from the corresponding intra-operative bile duct cultures. A prospective study investigating bile duct cultures and the immediate patient outcome would be more powerful to demonstrate a correlation between the micro-organisms of bile duct cultures and SSIs, but a prospective study would need a vast number of patients and a long period for patient recruitment. An additional DNA fingerprinting of the micro-organisms from bile duct cultures with the culture results of SSIs may rule out doubts that these micro-organisms were identical, but unfortunately cultures were not preserved.
There was no correlation between post-operative SSIs and intra-operative bile duct culture results among several patients. Thus, bacteribilia cannot explain 100% of post-operative SSIs, because other risk factors also influence the risk for the development of a post-operative SSI [19]. Nonetheless, the majority of bile duct cultures matched post-operative SSIs and there is evidence that adjustment of antibiotic prophylaxis according to bile duct culture results can reduce the rate of post-operative SSIs [30].
In patients with polymicrobial colonization it is difficult to identify the micro-organism responsible for a post-operative SSIs, but polymicrobial colonization is the rule, especially after PBD and in patients with cholangitis [31]. Thus, the antibiotic prophylaxis should be broad enough to cover the most frequently isolated micro-organisms, including Enterococcus spp. in patients who underwent PBD.
Conclusion
Micro-organisms of post-operative SSIs in patients undergoing pancreaticoduodenectomy often match micro-organisms from colonized bile ducts, especially after PBD. Among both bile duct cultures and SSIs, there is an increasing number of opportunistic antibiotic-resistant species that are not covered by a routine antibiotic prophylaxis. Therefore, routine bile duct cultures should be taken during ERC or intra-operatively after bile duct transaction. The antibiotic prophylaxis should be adjusted according to the culture results. For patients with PBD coverage of opportunistic micro-organisms and Enterococcus spp. is required, whereas the antibiotic prophylaxis for patients without PBD needs no modification. Although we cannot answer the question of whether a modification of the antibiotic prophylaxis is able to reduce the rate of post-operative SSIs, the study results imply that a prospective study is needed.
Footnotes
Author Disclosure Statement
All authors certify that they do not have any conflict of interest or financial association conflicting with the presented manuscript. There are no founding sources associated with this article.