
Abstract
Abstract
Background:
Intra-abdominal infection may lead to adhesion and abscess formation. An adhesion barrier can reduce these complications but also aggravate intra-peritoneal infection, causing the opposite effects. The fear of infection propagation has limited clinical adhesion barrier use in a contaminated or infected abdomen. This study evaluated both adhesion and abscess reduction and infection propagation of a new ultrapure alginate-based anti-adhesive barrier gel in a rat peritonitis model.
Methods:
In 64 male Wistar rats, bacterial peritonitis was induced via intra-abdominal injection of a mixture of sterile feces, 105 colony-forming units (CFU) of Escherichia coli, and 104 CFU of Bacteroides fragilis. Surgical debridement and peritoneal lavage were performed 1 h after inoculation. Animals were randomly allocated in equal numbers to a control group or an alginate gel group. Animals were sacrificed on day five post-operatively. Death and the presence and size of intra-abdominal abscesses were noted, and adhesions were scored. All outcomes were compared in the two groups.
Results:
Seventeen rats (27%) died prematurely without any difference between the groups. Of the surviving rats in the alginate gel group, 88% developed abscesses vs. 100% of the control group. There was no significant difference in the abscess scores or incidence rates of adhesion formation between the groups. The adhesion scores were lower for the alginate gel group compared with control animals (p=0.04).
Conclusion:
Ultrapure alginate gel reduces adhesion severity but not abscesses. The gel seemed to be safe, not aggravating intra-peritoneal infection in this abdominal infection model.
I
Anti-adhesive agents seem to be a good measure to reduce the early (e.g., intra-abdominal abscess) and long-term (e.g., small bowel obstruction, adhesiolysis-associated injury at repeat surgery) complications of adhesion formation in peritonitis [7,8]. A number of anti-adhesive barriers, including films, gels, sprays, and fluids, have been developed over the past decade. However, most are not recommended for use in the presence of gross contamination or infection [9,10].
One barrier, hyaluronic acid–carboxymethylcellulose membrane, demonstrated limited reduction of adhesion formation when used at surgery for complicated diverticulitis in a small randomized trial [11]. The same barrier was associated with worse intra-abdominal infection when wrapped around a fresh intestinal anastomosis [12]. A study in patients with benign colorectal disease investigating a modification that included glycerol was terminated after an interim analysis showed a greater number of infections [13]. Extended infection propagation also has been demonstrated for oxidized cellulose membrane in the presence of blood and bacterial contamination and for some gel formulations in both clinical and experimental studies [14–18]. These reports prompt caution in using adhesion barriers in surgical disorders characterized by gross contamination or infection of the abdominal cavity, the same disorders that would benefit most from adhesion prevention efforts in terms of their propensity for abscess development and its associated morbidity. Also, these data emphasize the necessity to demonstrate that any new adhesion barrier does not aggravate local infections.
We recently showed excellent adhesion reduction in a new ultrapure, easy to apply, alginate gel in a cecal abrasion and peritoneal sidewall excision model. The reported antibacterial capacity of ultrapure alginate gel also may contribute to a favorable effect in a contaminated environment [19].
Our group has validated an experimental model of intra-abdominal infection with early surgical intervention, performing debridement and lavage and resulting in a 20%–40% mortality rate, formation of abscesses, and adhesions. This model is suitable for investigating both the effect of anti-adhesive agents in abdominal infection and the safety of these agents regarding propagating infection with increased abscess formation and a higher mortality rate under contaminated conditions. The aim of the present study was two-fold: To assess the effect of ultrapure alginate gel on adhesions and the incidence of abscess formation, and to determine safety, as judged by the mortality rate and abscess incidence in a rat model of abdominal infection.
Materials and Methods
Animals
Sixty-four male Wistar rats (Harlan BV Horst, The Netherlands) were used. The rats weighed between 230 g and 280 g and were housed in filter-topped cages (two rats per cage) under clean, non-sterile, standardized conditions for at least five days prior to the experiment. All animals were weighed daily and had free access to water and standard rodent chow (Ssniff R/M-H, Bio Services BV, Uden, The Netherlands) during the experimental period. The study protocol was approved by the Institutional Animal Ethics Review Committee, and the study was performed in the GLP-certified animal research laboratory of the Radboud University Medical Center. Prior to the experiment, humane endpoints were defined in order to avoid unnecessary suffering by the animals.
Experimental design
In all rats, bacterial infection of the abdominal cavity was induced using a validated model [20]. Rats were allocated randomly to two groups (n=32 each). Animals in the first group received no further treatment and served as the control group. In the second group, animals received 2 mL of ultrapure alginate gel. All animals were sacrificed at post-operative day five for comprehensive analysis of abscesses and adhesions. Premature death was assessed; a group that also included rats was taken out of the experiment because they reached the humane endpoint.
Experimental protocol
Each animal was prepared for surgery by shaving and cleaning the lower abdomen with 70% alcohol. For analgesia, rats were given buprenorphine (Temgesic; Schering-Plough, Houten, The Netherlands), 0.02 mg/kg subcutaneously, starting 30 min before surgery and repeating the same dose every 12 h for the next 48 h. Peritonitis was induced in all rats by a transcutaneous intra-peritoneal injection of 2 mL of fecal suspension prepared using fresh feces from Wistar rats mixed with two volumes of water. After sterilization and centrifugation (15 min at 750×g), the upper two layers were combined, sterilized, and stored at 4°C until use. For each rat, 1 mL of fecal suspension and 1 mL of saline containing 104 colony-forming units (CFU) of Bacteroides fragilis (strain 25285 from the American Type Culture Collection, Manassas, VA) and 105 CFU of Escherichia coli (strain 25922 from the ATCC) were mixed. One hour after inoculation, surgery was performed. Rats were anesthetized by inhalation of a mixture of 3% isoflurane (Abbott Laboratories, Queensborough, UK) and 1:1 oxygen:pressurized air. They underwent a midline laparotomy, and the abdominal cavity was debrided, including partial resection of the omentum in order to remove macroscopic omental contamination. The abdominal cavity was rinsed with 20 mL of sterile 0.9% NaCl at 38°C to remove any contaminated material. This treatment mimics the clinical scenario of early source control and lavage in intra-abdominal infection or heavy contamination without systemic antibiotics [20].
Control animals received no further treatment. In the second group, 2 mL of ultrapure alginate gel (Rebasol™, European Medical Contract Manufactory [EMCM], Nijmegen, The Netherlands) was applied both at the site of inoculation and in the upper left quadrant in the proximity of the liver. These areas were occupied commonly by adhesions and abscesses in previous experiments [21]. The abdomen was closed in two layers using 3-0 polyglactin 910 (Vicryl) (Ethicon Products, Amersfoort, The Netherlands) suture for the fascia/muscle layer and wound staples for the skin. Animals were resuscitated immediately after abdominal closure with 10 mL of isotonic sodium chloride (0.9%) solution administered subcutaneously. During the operation and shortly thereafter, rats were placed on a warm plate to avoid hypothermia.
Adhesion and abscess formation
Animals were euthanized by carbon dioxide asphyxiation on post-operative day five. The abdomen was reopened and inspected for adhesion formation. Adhesions were scored by an investigator who was blinded to the group assignment using grading system of Zuhlke et al. [22]. Adhesions were classified macroscopically as 0=no adhesions; 1=filmy adhesions, easy to separate by blunt dissection; no vascularization; 2=mild adhesions, blunt dissection possible but some sharp dissection required; 3=strong adhesions, lysis possible by sharp dissection only; clear vascularization; 4=very strong adhesions, lysis possible by sharp dissection only (organ strongly attached with severe adhesions). The sites of adhesions that were scored were the midline; the upper abdomen (liver); the omentum, sidewall and cecum; and the spaces between the bowel loops.
The number and size of abscesses also were noted. An abscess was defined as a walled-off collection containing purulent material [23]. Abscesses were scored using the objective size system of Rodgers et al.: 0=no abscess; 1=several small abscess; 2=medium abscess present; 3=large or several medium abscesses present; 4=one very large abscess or several large abscesses present [24].
Statistical analysis
A power calculation was performed (G* Power 3.1.2)[25] using a one-sided Fisher exact test with α=0.05 and β=0.9. The expected frequency of abscess formation was set at 80% for the control group and 32% (60% decrease) for the experimental group, yielding a group size of 22 animals. The calculated group size was increased by 10 animals in view of the maximum associated mortality rate of 30% in the control group.
Statistical analysis for adhesion and abscess incidence and scores, survival, and animal weights was performed using the non-parametric Mann-Whitney U test, Fisher exact test (two-tailed), or a two-tailed unpaired T-test, as appropriate. A p value <0.05 was considered statistically significant.
Results
All rats became severely ill after inoculation, characterized by lack of movement, erect body hair, diarrhea, ocular exudates, and anorexia. These signs usually resolved within 2 d. Body weight decreased during the first 3 d after inoculation and stabilized thereafter. The change in the body weight did not differ between the control and experimental groups (Fig. 1).

Post-operative course of body weight, shown as average weight in relation to weight prior to operation.
Deaths
The overall mortality rate was 27% (17/64), 25% (8/32) in the experimental group and 28% (9/32) in the control group. Most of the rats died during the first 48 h after inoculation. Nine of 17 animals (six in the control group and three in the alginate gel group) that died prematurely showed extensive fibrinous adhesions and a purulent abdomen. Eight animals (three in the control group and five in the alginate gel group) had to be taken out of the experiment because of extreme weight loss and poor clinical condition. All eight animals showed signs of ileus, purulent material, and adhesions.
Adhesion formation
Eighty-three percent (20/24) of the rats in the alginate gel group displayed adhesions, compared with 91% (21/23) of the control rats (p=0.662). The overall adhesion score was significantly lower in the alginate gel group (p=0.037) than in the control group (Table 1). The median adhesion scores at the five locations are shown in Table 1. Adhesion scores were significantly lower in the area of the liver (p=0.031), the sidewall (p=0.040), and the cecum (p=0.046) in the alginate gel group than in the control animals.
p=0.05 vs. control animals.
Abscess formation
Eighty-eight percent (21/24) of the surviving rats in the alginate gel group developed abscesses compared with 100% of the control group (p=0.234; Fig. 2A). Although the number of abscesses per rat (Fig. 2B) and the abscess score (Fig. 2C) showed reduced median values in the alginate gel group, the difference from the control group was not significant.
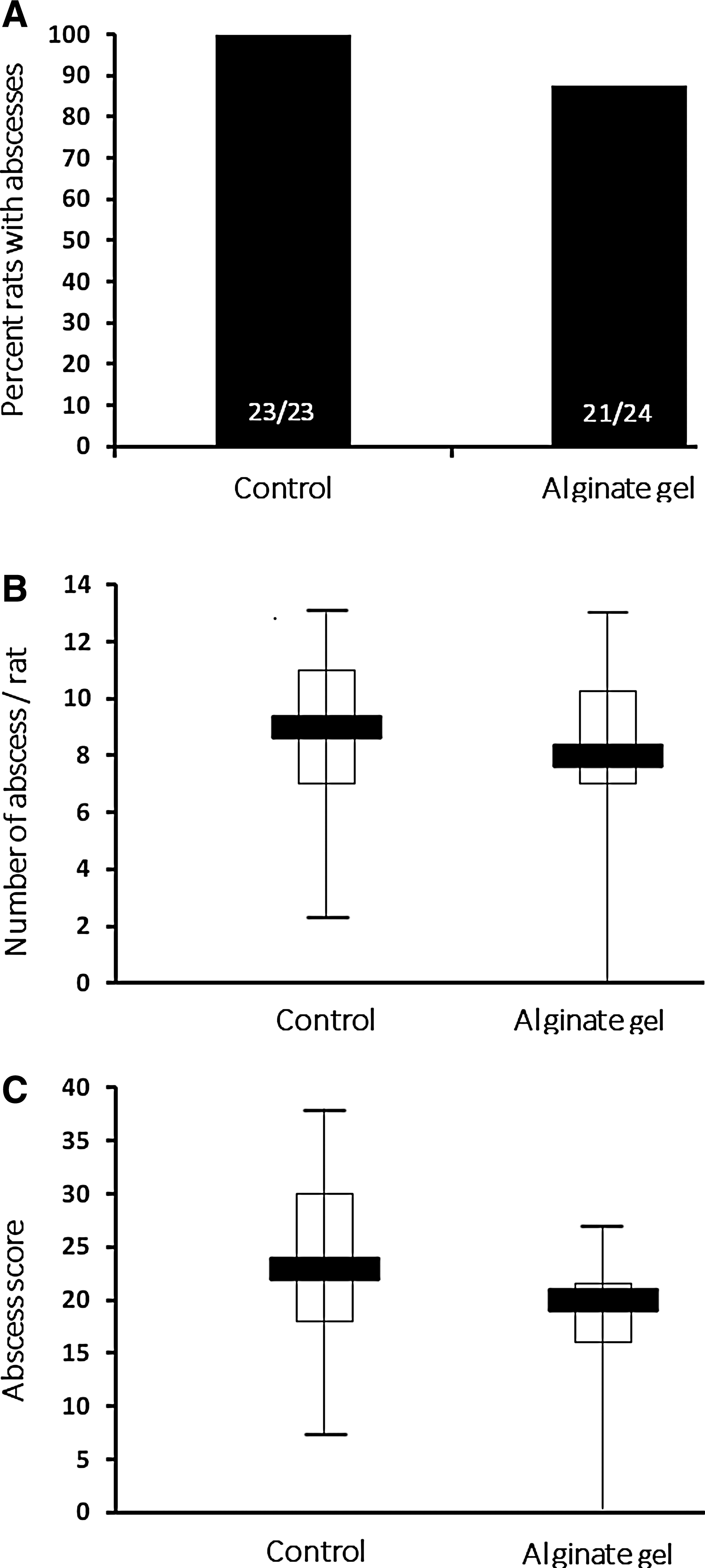
Abscess formation.
Discussion
The present study provides no evidence that ultrapure alginate adhesion barrier gel is efficacious in reducing abscess formation in a clinically relevant abdominal infection model. Adhesion formation was reduced at three relevant locations. At the same time, there was no evidence of infection propagation, as reflected by comparable residual infection and mortality rates in the experimental and control rats. Thus, unlike the results with some other adhesion barriers, there seems to be no safety concern associated with intra-peritoneal application of alginate gel in abdominal bacterial peritonitis or contamination.
We expected a decrease of adhesion and abscess formation based on the barrier function and antibacterial and anti-inflammatory activity of the alginate gel [26,27]. Alginates significantly inhibit the expression of various pro-inflammatory cytokines such as interleukin-1β and tumor necrosis factor-α, which promote adhesion formation and residual infection [21,28,29]. Alginate gel has a pH ranging from 7.1 to 7.5, which might play a role in maintaining intra-abdominal conditions favorable for host defense cells and unfavorable for bacterial growth and abscess formation [16,30]. Despite the absence of a significant reduction in the number of rats with adhesions, significantly fewer adhesions were observed in the liver and sidewall areas, sites where the gel was applied. The high viscosity of the gel might have limited diffusion through the abdominal cavity, preventing a more remote and broader action [19]. The better and broader effect of more liquid adhesion barriers compared with viscous solutions has been demonstrated by our group for carboxymethylcellulose and low-viscosity hyaluronan and tissue plasminogen activator solutions [8,16,31]. Further, bowel paralysis during peritonitis and compartmentalization of the abdominal cavity secondary to rapid fibrin formation may have contributed to limited distribution of the gel. We were unable to locate remnants of the gel at sacrifice to gain insight into its dispersion through the abdominal cavity. Possibly, there is a large adhesion formation potential in peritonitis models that cannot be counteracted sufficiently by a site-specific adhesion barrier. Notably, overwhelming fibrin formation was present in 50% of the animals that died within 48 h. In retrospect, multiple deposits of gel at adhesion and abscess predilection areas might have improved the anti-adhesive action.
The peritonitis model used in the current study has been validated in a series of experiments in our department as a way to induce generalized peritionitis, characterized by a mortality rate approximating 30%, high peritoneal pro-inflammatory cytokine concentrations, and multiple abscess locations, as observed in the clinical situation [20,21,32]. It mimics the surgical approach in secondary peritonitis with source control and debridement by saline lavage, as well as the condition of severe contamination at elective colorectal surgery but without antibiotic use. Antibiotics were not used deliberately in this experiment, as they would have decreased the mortality rate, which might have masked infection potentiation (e.g., bacteremia and death), by the alginate gel [7]. Previous studies using similar models showed that systemic antibiotics do not affect abscess formation [33].
The new ultrapure alginate gel did not aggravate abdominal infection, as reflected by similar mortality and abscess formation rates. We recently found safety in an anastomotic leak model based on the mortality rate and abscess formation (unpublished data). Taking the findings in both models together, evidence is provided that ultrapure alginate gel meets the relevant safety criteria of an anti-adhesive barrier.
A potential drawback of this study design is the necessity to assess adhesion and abscess formation simultaneously at sacrifice, 5 d after induction of abdominal infection. Post-operative day 14 is a more common time point for adhesion assessment [19]. Intra-abdominal abscess numbers tend to decrease after 1 wk, probably as a result of the innate peritoneal defense mechanisms in the rat. Nevertheless, we believe that the fibrinous adhesions at day five may represent “mature” adhesions at 14 d because peritonitis is a potent accelerator of fibrinous adhesion formation and peritoneal fibrinolytic activity, dissolving fibrin within 5–7 d is depressed significantly in peritonitis [4]. It should be kept in mind that adhesions are dynamic stuctures, so that the accuracy of adhesion scoring at any time after an insult may be questioned. Nevertheless, it generally is accepted that fibrinous attachments not resolved in the first week will develop into fibrous attachments [5].
Despite promising characteristics, ultrapure alginate did not reduce abscess formation in experimental peritonitis and had only site-specific anti-adhesive action. Contrary to many other compunds, the gel did not propagate infection, which holds promise for its use in (clean) contaminated gastrointestinal surgery.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest. The research leading to these results received funding from the European Community's Seventh Framework Programme; MultiTERM, grant agreement no. 238551.