
Abstract
Abstract
Background:
Determining predictors of surgical site infection (SSI) in a large cohort is important for the design of accurate SSI surveillance programs. We hypothesized that additional organ resection and pelvic exenterative procedures are associated independently with a higher risk of SSI.
Methods:
Patients in the American College of Surgeons National Surgical Quality Improvement Program® (ACS NSQIP®; American College of Surgeons, Chicago, IL) database (2005–2012) were identified (n=112,282). Surgical site infection (superficial or deep SSI) at 30 d was the primary outcome. Using primary and secondary CPT® codes (American Medical Association, Chicago, IL) pelvic exenteration was defined and additional organ resection was defined as: bladder resection/repair, hysterectomy, partial vaginectomy, additional segmental colectomy, small bowel, gastric, or diaphragm resection. Univariable analysis of patient and procedure factors identified significant (p<0.05) predictors, which were modeled using stepwise logistic regression.
Results:
The rate of SSI was 9.2%. After adjusting for operative duration, predictors of SSI were body mass index (BMI) 25–29.9 (odds ratio [OR]: 1.3), BMI 30–34.9 (OR: 1.59), BMI 35–39.9 (OR: 2.11), BMI>40 (OR: 2.51), pulmonary comorbidities (OR: 1.22), smoking (OR: 1.24), bowel obstruction (OR: 1.40), wound classification 3 or 4 (OR: 1.18), and abdominoperineal resection (OR: 1.58). Laparoscopic or laparoscopically assisted procedures offered a protective effect against incision infection (OR: 0.55). Additional organ resection (OR: 1.08) was also associated independently with SSI, but the magnitude of the effect was decreased after accounting for operative duration. In the analysis that excludes operative duration, pelvic exenteration is associated with SSI (OR: 1.38), but incorporating operative duration into the model results in this variable becoming non-significant.
Conclusions:
In addition to other factors, obesity, surgery for bowel obstruction, abdominoperineal resection, and additional organ resection are independently associated with a higher risk of SSI. Surgical site infection risk in pelvic exenteration and multiple organ resection cases appears to be mediated by prolonged operative duration. In these established high-risk sub-groups of patients, aggressive interventions to prevent SSI should be implemented.
S
In addition to comorbidities, the indication for surgery and extent of surgical resection may put the patient at an increased risk of SSI that may be nearly impossible to mitigate. For example, advanced colorectal cancer stage (stage IIB and higher) was found to be associated with a higher incidence of SSI in a French case-matched study of more than 500 patients [2]. Establishing and quantifying the contribution of operative complexity, typically the result of disease complexity, to the risk of SSI will help surgeons counsel patients and interact with hospital administrators as they design realistic interventions to address SSI. Comparing hospital SSI rates may be misleading and discouraging if case mix is not considered adequately.
Prior studies have examined pre-operative patient factors, for example, comorbidities, smoking, and pre-operative serum laboratory values [3], that impact adversely SSI [4–6]. Higher rates of SSI have been reported in left-sided colectomy compared with right-sided colectomy [7,8] and after resections for rectal cancer compared with colon cancer [9]. Few studies have focused on the extent of surgical resection performed during a colorectal procedure, other than some reports of increased risk of SSI with additional concurrent procedures such as mobilization of the splenic flexure, small bowel resection [10], and concurrent pancreatectomy [11].
The purpose of our study was to investigate the impact of concurrent additional organ resection and pelvic exenterative procedures on the risk of superficial and deep SSI compared with colorectal resection alone. We chose to focus on elective cases, which are common targets for quality improvement initiatives. Concurrent organ resection and pelvic exenterations represent one form of complexity that may contribute to increased risks of SSI. Pelvic exenteration for rectal cancer is associated with SSI rates ranging from 26% [12,13] to 38% [14]. With an interest in a large sample with the highest quality data, particularly for outcome assessment with regard to 30-d surgical site infections, we used the American College of Surgeons National Surgical Quality Improvement Program® (ACS NSQIP®; American College of Surgeons, Chicago, IL) database. Because operative duration has also been found to be associated with complications in colorectal surgery [5,15] we sought to determine whether prolonged operative duration contributed to the increased risk of SSI as a secondary aim.
Patients and Methods
Data source
The ACS NSQIP, previously described in other publications, is a hospital-based, standardized data collection system that inventories patients who have had elective and emergency surgery. Data are submitted to the ACS, risk adjusted, and then presented to member hospitals for the purposes of ongoing quality improvement. Thirty-day outcomes are collected by dedicated and trained surgical clinical reviewers utilizing inpatient and outpatient documentation as well as follow-up telephone calls to patients. Patient comorbidities, habits, laboratory values, and pre-operative condition (e.g., sepsis, inpatient versus outpatient status, ventilator dependence) are included in the database. A single ICD-9 post-operative diagnosis code is assigned to each patient. The database has a field for a primary CPT® code (American Medical Association, Chicago, IL) as well as multiple fields for concurrent CPT codes.
Study cohort
We identified patients from the national ACS NSQIP dataset from 2005 to 2012 who underwent elective colorectal resections for the following indications: benign lesions, colorectal cancer, diverticulitis, inflammatory bowel disease (IBD), volvulus, and bowel obstruction. Categories of age were created based on decade, and body mass index (BMI) was grouped into the following categories: underweight, normal, overweight, and obese classes I, II, and III.
Procedures were categorized using primary and secondary CPT codes. Primary procedures were stratified as colectomy, proctectomy, abdominoperineal resection, and ileal-pouch anal anastomosis. Additional major organ resection was subcategorized as: concurrent additional segmental colonic resection (CPTs: 44140-1, 44143-4,44150-1,44157-8,44160,44204-8, 44210-2, 44155-6), small bowel resection (CPTs: 44120-1, 44202-3), gastric resection (CPTs: 43610-1, 43620-1, 43631-4), diaphragm resection (CPTs: 39560, 39561), major vascular repair (CPTs: 35221, 35251, 35281), bladder resection/repair (CPTs: 51550, 51555, 51565, 51800, 51820, 51860, 51865, 51880, 51960), hysterectomy (CPTs: 58150, 58152, 58180, 58200, 58210, 58570-3, 58951-4, 58956), or partial vaginectomy (CPTs: 57106, 57109). Pelvic exenteration was defined broadly in order to be inclusive of cases. We used the following CPT codes or code combinations: rectal resection (45110, 45111, 45113, 45114, 45119, 45120, 45123, 45395, 45397) with hysterectomy (58150, 58152, 58180, 58200, 58210, 58570-3, 58951-4, 58956); rectal resection with complete cystectomy (51570, 51575, 51580, 51585, 51590, 51595, 51596); or pelvic exenteration (45126, 51597, 58240). Cases that involved a stoma (colostomy or ileostomy) were defined by CPT codes: 44141, 44143, 44144, 44146, 44151, 44155, 44156, 44206, 44208, 44211, 44212, 45110, 45111, 45119, 45123, 45395).
American Society of Anesthaesiologists (ASA) classification was not included in the analysis because of redundancy with pre-operative comorbidities and its subjective nature. The subjective nature of its assignment has been demonstrated in several studies that showed a modest lack of agreement of ASA scores between providers [16–18]. Estimated blood loss during surgery is not available in the ACS NSQIP database. Operative duration was defined as time from incision to closure. The primary outcome of SSI was defined as superficial or deep SSI detected at 30 d [19]. Surgical site infection was the dependent variable in our statistical analyses. Major complications were defined as organ/space SSI (which includes intra-abdominal abscess, pelvic abscess, or clinically evident anastomotic leaks), incision disruption, sepsis or septic shock, transfusion after surgery, post-operative pneumonia, unplanned intubation, ventilator status for longer than 48 h, pulmonary embolism, acute renal failure, progressive renal insufficiency, stroke, myocardial infarction, cardiac arrest requiring cardiopulmonary resuscitation (CPR), or post-operative coma lasting longer than 24 h.
Statistical analysis
Univariable analysis identified predictors of SSI at a p<0.05 level that were then analyzed in a multivariable regression to identify independent predictors for the model. A second multivariable analysis was performed by adding operative duration to the model. Model fit with the data was assessed using the C statistic and the Hosmer-Lemenshow test, a goodness-of-fit test that examines the model's ability to assign risk accurately. A non-significant p value for this statistic indicates that the model assigns risk adequately. Statistical analysis was performed in SAS 9.3 (SAS Institute, Cary, NC).
Patients
Use of de-identified data from a national database is exempt from review by the University of Minnesota Institutional Review Board.
Results
Among the 112,282 patients who underwent elective colorectal surgery (45.8% laparoscopically), the overall rate of SSI was 9.2% (n=10,353). Superficial SSI occurred in 7.8% of patients and deep SSI occurred in 1.5% of patients. The median time to superficial SSI was 9 d (interquartile range [IQR] 6–14 d), and to deep SSI was 7 d (IQR 6–14 d). Nearly half of superficial SSIs (41.6%) and deep SSIs (47.7%) occurred after hospital discharge.
Complex procedures
A substantial fraction (15.9%) of the cohort underwent additional organ resections. These were performed mostly in cases in which the diagnosis was diverticular disease (39.3%), colon cancer (28%), or rectal cancer (19.6%). The majority of these additional procedures were additional segmental colectomy or small bowel resection (Table 1). The vast majority of pelvic exenterations were performed for the indication of rectal cancer (88.2%).
Surgical site infections in patients undergoing pelvic exenteration and additional organ resection
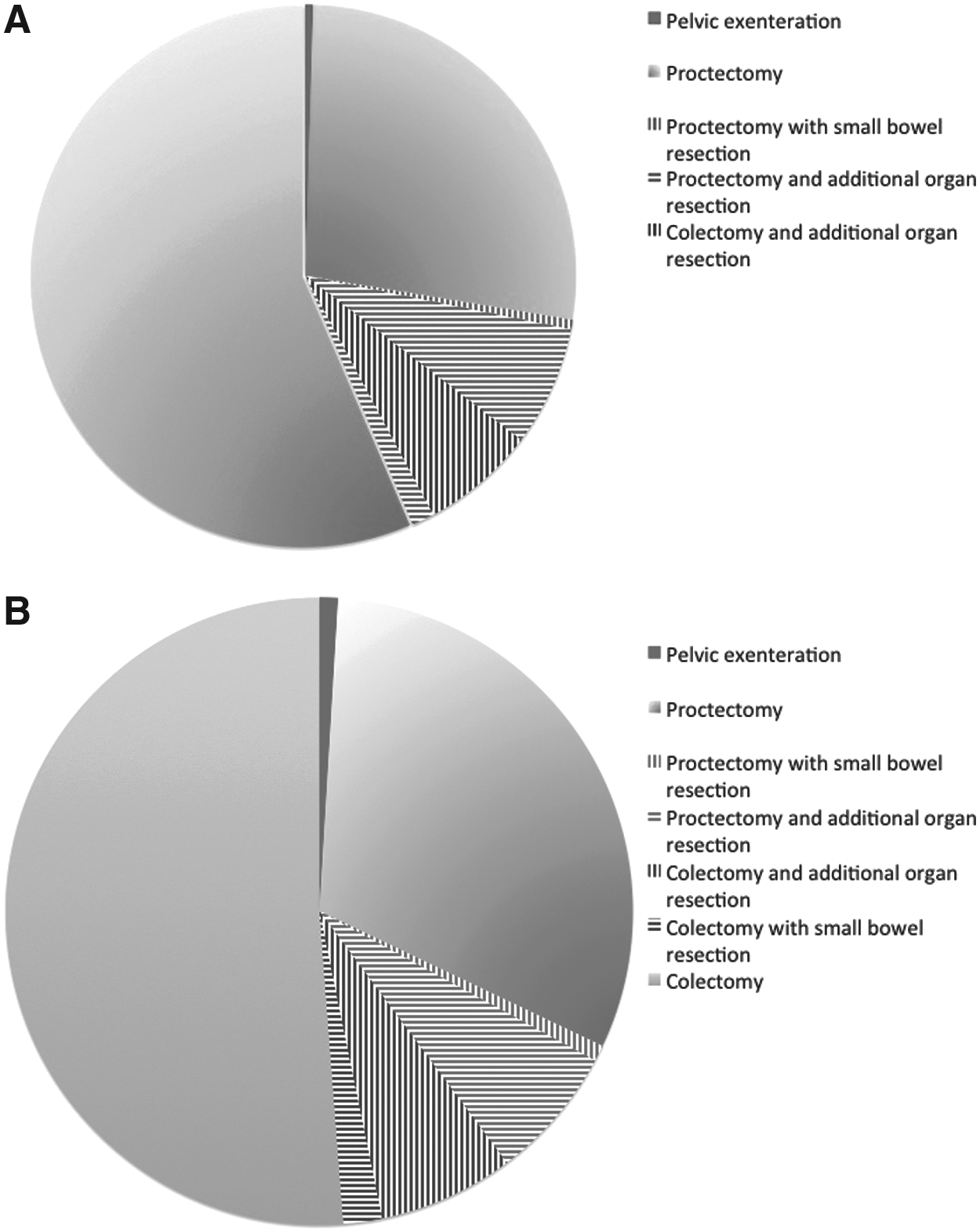
Nineteen percent of patients undergoing pelvic exenterations developed an SSI within 30 d of surgery. Compared with other patients in the cohort, patients who underwent pelvic exenteration had a higher rate of deep SSI (5.3% versus 1.4%; p<0.0001). Patients who underwent abdominoperineal resection were also more likely to have deep SSIs (4% versus 1.3%; p<0.0001). Ten percent of patients who underwent additional organ resection developed an SSI and these patients were no more likely to develop a deep SSI than other patients. Proportions of patients in the cohort who underwent proctectomy, colectomy, additional organ resection, and pelvic exenteration are displayed in Figure 1A and proportions of those patients who developed SSIs are shown in Figure 1B.
(
Independent risk factors for superficial and deep SSI
The rates of superficial and deep SSIs in patients with various risk factors are shown in Table 2. Two adjusted multivariable models to examine risk factors for SSIs are shown in Table 3. In model 1, all significant risk factors on univariable analysis, except operative duration, are included. In model 2, operative duration (time from incision to closure) is added to model 1. The median operative duration for the cohort was 157 min (IQR: 112–220). Important independent risk factors for SSI, as determined by the magnitude of the odds ratio are BMI 30–34.9, BMI 35–39.9, BMI >40, abdominoperineal resection, and pelvic exenteration. Multiple other significant risk factors, including additional organ resection, are shown in Table 3. To demonstrate the impact of prolonged operative time as an explanatory factor, this variable was added to the multivariable model. Between the two models, the magnitudes of odds ratios did not change by >0.1 for most risk factors. However, the following risk factors showed an attenuation in the odds ratio of >0.1 after adjusting for operative duration:pelvic exenteration (OR decrease: 1.38 to 1.07), additional organ resection (OR decrease: 1.19 to 1.08), inflammatory bowel disease (OR decrease: 1.24 to 1.12), BMI 35–39.9 (OR decrease 2.24 to 2.11), and BMI >40 (OR decrease: 2.72 to 2.51). Laparoscopic surgery showed the same magnitude of protection against SSI even after adjusting for operative duration. Multivariable models had modest predictive ability with C statistics of 0.645 for model 1, and 0.654 for model 2. Hosmer-Lemeshow statistics showed significant p values (p=0.0273 and p=0.0099). However, using large databases such as ACS NSQIP presents the problem that smaller deviations from perfect calibration will appear statistically significant [20,21].
Chi square test.
Logistic regression.
CI=confidence interval; BMI=body mass index.
Model 1 C statistic: 0.645; Hosmer and Lemshow χ2 17.28, goodness-of-fit p=0.0273.
Model 2 C statistic: 0.654; Hosmer and Lemshow χ2 20.1, goodness-of-fit p=0.0099.
NS=not statistically significant; BMI=body mass index.
For each hour of surgical operative time, the incision infection rate increased by 1%–2% (Table 4). Patients undergoing an abdominoperineal resection or pelvic exenteration were likely to have prolonged procedures. More than half of patients undergoing abdominoperineal resection were in the operating room for more than 4 h, and more than half of patients undergoing pelvic exenteration were in the operating room for more than 6 h (Table 4).
The impact of SSI on length of stay
The median length of stay (LOS) for patients with SSIs was longer (p<0.0001) than for patients without SSIs (7 d [IQR=5–11] versus 5 d [IQR=4–7]). Even among patients who suffered no major complications (n=94,343; 84%), post-operative LOS was longer (p<0.0001) in patients who developed an SSI prior to hospital discharge (n=2,564; mean, 11.3 d; median, 10; IQR=7–13) compared with patients without an SSI (n=91,770; mean, 5.8 d; median, 5; IQR=4–7). Among patients with only superficial but not a deep SSI who had no major complications, the median length of stay was significantly longer (mean, 7.5 d; median, 6; IQR 5–9) than patients without major complications or any SSI (p<0.0001).
Discussion
We sought to determine whether the complexity of colorectal resection, defined as the requirement for additional major organ resections, is associated with an independently higher risk of SSI. The results of our multivariable analysis suggest that this is the case. However, in a further analysis, we found that adjusting for operative duration (time from incision to closure) in the model decreased the effect size for pelvic exenteration, with a decrease in the odds ratio from 1.38 to 1.07 between the two models. Additional organ resection also has a lesser impact on SSI after accounting for operative duration, with a decrease in the odds ratio from 1.19 to 1.08. Abdominoperineal resections remained at high risk for SSI even after incorporating operative duration, suggesting that other factors such as cancer diagnosis and incision at the abdomen and perineum may play a larger role. Of note, the use of a soft tissue flap for perineal incision reconstruction after an abdominoperineal resection or pelvic exenteration, was not protective against SSI in our analysis. Overall, our findings suggest that a substantial contribution to the risk of SSI after complex procedures comes from prolonged operative time.
More than half of pelvic exenterations lasted longer than 7 h. Whether this is a parameter that can be modified is unclear. A prolonged complex case typically involves time-consuming technical challenges such as defining anatomy in obliterated planes or controlling bleeding. However, an understanding of why certain procedures take so long is poorly studied and other modifiable factors such as multi-specialty team planning, surgeon availability, surgeon sequencing during a case, critical assessment the role of a trainee, equipment procurement, and operating room staff proficiency may contribute to prolonged operative duration.
Our study also found that abdominoperineal resection alone was also strongly associated with SSI. In the ACS NSQIP database, an infection at either the abdominal or perineal incision would be coded as an SSI. Perineal incision complications are known to be common in these patients. Most prior literature reports composite rates of perineal complications without distinguishing between infections and dehiscence [22,23]. Recently reported rates of perineal incision infection rates are 13.6% [24], 14.7% [25], 15.2% [26], and 30% [27]. Perineal SSIs in these patients may be associated more strongly with contamination in the setting of untoward tissue properties such as ischemia, radiation, and tension.
Our study did not show an independent association between stoma formation and SSIs on multivariable analysis. This finding has been observed in other studies using institutional data [28,29] and our study has a large enough sample size to exclude the presence of such an association. Elective cases that included a stoma had a 12.2% rate of SSIs, which is higher than the overall rate for our cohort, but likely associated confounding risk factors such as inflammatory bowel disease, abdominoperineal resections, and surgery for bowel obstruction.
As has been shown in other studies, SSIs are associated with increased LOS. Our study describes this relation further first by confining this analysis to patients who develop an SSI prior to hospital discharge, and second by examining patients who only had an SSI but no other ACS NSQIP-reported complications that may have contributed to increased LOS. Despite these adjustments, an SSI continues to be associated strongly with more hospital resources, with a twofold difference in post-operative length of stay, and is a worthwhile outcome to examine.
Nearly half of SSIs that result from colorectal surgery are diagnosed after the initial hospitalization. Our analysis confirms this, showing that 41.6% of superficial SSIs and 47.7% of deep SSIs were diagnosed after hospital discharge. Mandated SSI surveillance systems that do not ensure outpatient follow-up will lead to unfair comparisons that merely reflect an institution's connectedness to its patient population rather than true differences in infection rates.
The purpose of this study was to establish high-risk groups of patients undergoing colorectal surgery who would be the target of quality improvement initiatives. A large number of studies looking at single or bundled approaches to reduce colorectal SSI, but few studies have suggested techniques to be used on high-risk patients that would be inappropriate for average-risk patients. A classic approach to the incision with devitalized tissue or heavy contamination is to leave it open to heal by secondary intention. In our study, the unadjusted rate of SSI in contaminated or dirty cases (12%) was lower than the rate in morbidly obese patients (16.8%) and patients undergoing pelvic exenteration (19.4%). It stands to reason that leaving incisions open in these patients could reduce the rate of SSI, however, further studies would be required to assess the impact of such an intervention on LOS, health care costs, impact on ostomy pouching, and patient experience. In patients with colorectal cancer, incision complications can delay chemotherapy, but leaving incisions open after high-risk surgery may have the same effect.
Despite the large numbers of patients included in the ACS NSQIP database, our study has a number of limitations. Although data are collected by trained reviewers, it is possible that additional concurrent procedures are not entered into the database because only a primary CPT code is required by the system. Another difficulty with using CPT codes to portray the nature of a procedure is that it is impossible to determine which of the procedures were unavoidable versus avoidable events. This distinction is important for quality improvement endeavors. For example, a concurrent partial cystectomy may have occurred as a result of accidental or inadvertent laceration of the bladder. With better pre-operative planning or intra-operative skills this resection and its associated SSI risk could be avoided. Similarly, the fact that bowel obstructions were observed in this cohort of elective, as opposed to urgent/emergency cases suggest that this finding was unexpected, raising the question of whether surgical intervention at an earlier stage could have decreased the risk of infection. The concept of prolonged surgery is also another component of the procedure that could be inherent to the planned procedure as opposed to potentially mitigated by better technical skills, operative planning, or better trained assistants. Therefore, our data should not be interpreted to “explain away” increased risks of SSIs in prolonged cases.
Our statistical models only showed moderate predictive abilities based on the C statistic, despite the high number of patients. This has been observed in other studies of SSI and likely reflects the fact that other unidentified or uncollected variables contribute to SSI, such as processes of care (skin preparation, pre-operative antibiotics, oral antibiotic bowel preparation) or technical aspects during surgery with regard to managing potential contamination. In addition, the Hosmer-Lemeshow test also shows our models to be sub-optimal in its predicative abilities, however, this is far more likely to occur in a database of more than 100,000 patients, such as ours.
Conclusion
Pelvic exenterations, colorectal surgery with additional organ resections, and abdominoperineal resections are procedures with a high risk of SSI. Future studies of SSI reduction programs should make special note of these cases and address whether successful SSI interventions have equally protective effects on this challenging sub-group of patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.