
Abstract
Abstract
Background:
Implant infections represent a relevant problem after immediate breast cancer reconstruction. In addition to difficulties in distinguishing early infections from other post-surgical complications (such as hematoma, seroma, and liponecrosis) late breast implant infections still represent a grey area of our knowledge with regards to heir definition and management. To address this issue, we prospectively monitored breast cancer patients at their center.
Methods:
Between February 1, 2009, and May 31, 2013, we enrolled all patients undergoing breast implant reconstruction or expander-to-prosthesis substitution. Patients without at least 6 mo of post-operative observation were excluded. We collected data from patient records including age, days from surgery (DFS), chemotherapy/radiotherapy, infecting microorganism, type of implant, antibiotic management and eventual implant removal. Sixty days from surgery were defined as the clinical threshold between early and late infection. Infections were further classified according to a graded scale into possible, probable and microbiologically proved.
Results:
Seventy-eight infections were recorded out of 766 surgical procedures (10.2%). Fifty-three (67%) cases occurred early ≤60 DFS, and 25 (33%) occurred late (i.e., beyond 60 d). By defining infection types as possible, probable or proved, the majority of late infections were classified as proved (84%) compared with 56% of early infections (p=0.0014). Microbiological isolate distribution was similar in proved early infections compared with proved late infections. Among late infections, a delayed occurrence was observed after prosthesis placement compared with expander insertion. Late infections were fraught with lower treatment success rates (12% vs. 41%, p=0.009).
Conclusion:
Late infection represents a consistent proportion of infections after immediate breast implant reconstruction or prosthesis placement and bear lower chance of salvage after treatment. An increased attention is warranted to improve prevention and treatment strategies.
P
Within the field of breast implant infections there are at least three main areas of uncertainty in clinical practice. First, definition of breast implant infection may be at times difficult because of the presence of only minor local signs in patients undergoing chemotherapy with dampened acute phase responses, no purulent drainage, or unavailability of samples for micro-biological evaluation. Secondly, timing and incidence of infection during the months/years after surgical implantation have been variably studied so far, predominantly with retrospective studies that consider either constrained observation periods or mixed breast implant infections with other surgical infections [4–8]. Accordingly, there are good indications on the factors associated with this occurrence, particularly early after implant insertion. There is, however, still controversy in the breast reconstruction area on the definition of infection and on the observation time required to define actual implant infection. Indeed, in this regard, early reports studied implant infection using a limited time of observation more useful for surgical site infection (SSI) evaluation [3,9,10] and not for prostetic infection.
Subsequently, the U.S. Centers for Disease Control and Prevention (CDC) [11] changed the definition of early prosthetic infection based on epidemiological and reporting criteria. However, within the frame of the specific clinical aspects associated with reconstructive surgery for breast cancer (e.g., radiotherapy, chemotherapy, repeated hospital accesses, filling procedures) [6,11], this may be of limited usefulness and possibly misleading. With regard to timing of post-surgical implant infection, agreement is found in time designations for late infections in other areas of prosthetic surgery. This is, for example, the case in prosthetic joint surgery where late and very late infections are defined when occurring after 3–24 mo and >24 mo [12], heart valve surgery (2 mo to 1 y and >1 y), and vascular prosthetic surgery (>4 mo) [9,13,14].
Indeed, not all reconstructive breast implant infections, in cancer patients, occur early after surgery (i.e., <60 d) [2,15]. Late breast implant infection occurring months to years after surgery still represents a grey area of our understanding with particular regard to incidence, etiology, physiopathology, and management, and are sometimes considered rare chance events in everyday clinical practice. So far, few patients with late prosthetic infections have been specifically reported in the literature [4,15,16] of which two occurred after reconstructive surgery for breast cancer and six occurred in patients after aesthetic augmentation. Accordingly, the incidence of late prosthetic infections has been reportedly low (1:10,000) according to old retrospective reports on predominantly aesthetic procedures in non-cancer patients [16,17]. On the other hand, many other reports clearly included such patients in their analyses, but did not describe the exact number with “late” onset of infection [18–21].
Finally, in addition to the wide range of clinical presentations of breast implant infections, there is still debate on the best clinical management to achieve implant salvage with few randomized or controlled studies to identify best management practices [22].
In view of the relative lack of structural information on these aspects, and following the observation of a patient showing symptoms and signs of late prosthesis infection after reconstructive surgery for breast cancer, we decided to begin a prospective clinical evaluation of our case series. The present analysis indicates that late infections, using 60 d as a clinical break-point, have a consistent frequency, accounting for one third of all observed infections, are more frequently microbiologically proved compared with early infections and have different clinical outcome.
Patients and Methods
Patients (766) were followed at the Breast Cancer Surgery and Plastic Surgery Units of IRCCS San Martino-IST in Genoa, Italy, between February 1, 2009, and May 31, 2013. A total of 832 devices (expander or prosthesis) were implanted for immediate reconstruction after mastectomy or for expander-prosthesis replacement in breast cancer patients.
All patients underwent surgery by the same surgical team and in all cases the same type of expander or prosthesis was used (Allergan, Marlow International, Parkway, United Kingdom). Expanders are implants positioned at surgery for immediate breast reconstruction and may be progressively inflated. Prostheses are permanent implants that are positioned as a substitution of the expander after its scheduled volume expansion. Antibiotic prophylaxis with cefazolin was always administered [23]. Clindamycin was used for prophylaxis in patients allergic to penicillin. After discharge, all patients were followed up as outpatients every fortnight for 1 mo, every 2 mo for the first year, and yearly thereafter.
After breast reconstruction, it is at times difficult to define the presence of infection. The local aspect may be intermediate without frank purulent discharge or suture dehiscence, and sampling for microbiology may be impossible or inconclusive. In these cases clinical conduct may vary from careful observation, to administration of antibiotics, to surgical attempts at implant salvage. For this reason we decided to evaluate patients according to a graded definition of infection derived and adapted from infections in neutropenic patients [24]. Post-operative implant infections types [2] were defined as possible (fever, minimal local edema, and inflammation resolving on empiric antibiotic therapy), probable (cellulitis, leukocytosis, systemic inflammation, echographic evidence of inflammation, or peri-prosthetic liquid accumulation, without microorganism isolation on echographic needle aspiration or blood culture), and proved (criteria for probable infection with cellulitis and presence of purulent discharge and microorganism isolation). Implant infections were further defined according to the time lapse after implantation as “early” when occurring within 60 d from surgery (DFS) and “late” when occurring >60 DFS. Patients without at least 6 mo of post-operative observation were excluded from the present evaluation to avoid bias because of a too-short post-surgical follow-up. Accordingly, patients were included after a 52-mo period (2/2009–5/2013) with a 58-mo observation. The following prospectively collected data from patient records were analyzed: Age, post-surgical days, chemotherapy/radiotherapy, infecting microorganism, type of implant, and implant removal. “Previous radiotherapy” was defined as any radiotherapy administered prior to implant surgery and includes for example patients with immediate expander positioning in the case of reccurence or second breast and prior radiotherapy during the primary tumor treatment. Cultures of surgical incision tissue samples, drainage fluids peripheral blood peri-prosthetic seroma, and the prosthetic itself (if removed), were performed to identify the infecting pathogens.
All causative microorganisms were identified using routine microbiologic methods. Disk susceptibility testing was performed and interpreted according to CLSI standards [25].
Antibiotic treatment aimed at implant salvage was performed with regimens including ampicillin-sulbactam (3gtid e.v.)+clindamycin (600mg tid iv), or+levofloxacin (500mg qd i.v/os), or daptomycin (350mg qd i.v.)+ rifampicin (600mg qd i.v.). Implant salvage was considered as successful maintenance of the original implant for ≥6 mo after antibiotic treatment or successful replacement of an expander with a prosthesis after antibiotic treatment with prosthesis retention for ≥6 mo.
To evaluate group differences, statistical analysis was performed employing two-sided tests as required (JMP 10.0 Statistical software, SAS Institute Inc., Cary, NC). Chi-square analysis, Fisher exact test, and Mann-Whitney test were performed as appropriate to check for differences between groups.
Results
Index case
A 67-year-old female underwent right mastectomy for breast cancer in 2004 followed by immediate reconstruction using an expander. In April 2006 the expander had been replaced by a double lumen permanent expander (Allergan Style 150 385–405 cc). No complications occurred in the following years.
On November 12, 2008, she was referred as an outpatient to our unit, following the abrupt appearance of fever, right breast pain, and general local discomfort a few days earlier.
Medications included aromatase inhibitors for breast cancer, valsartan, and metformin. Four weeks before the onset of symptoms, she underwent dental care without antibiotic prophylaxis. Clinical examination revealed cellulitis with signs of inflammation, redness, edema, and swelling extending to the nipple (Fig. 1A).
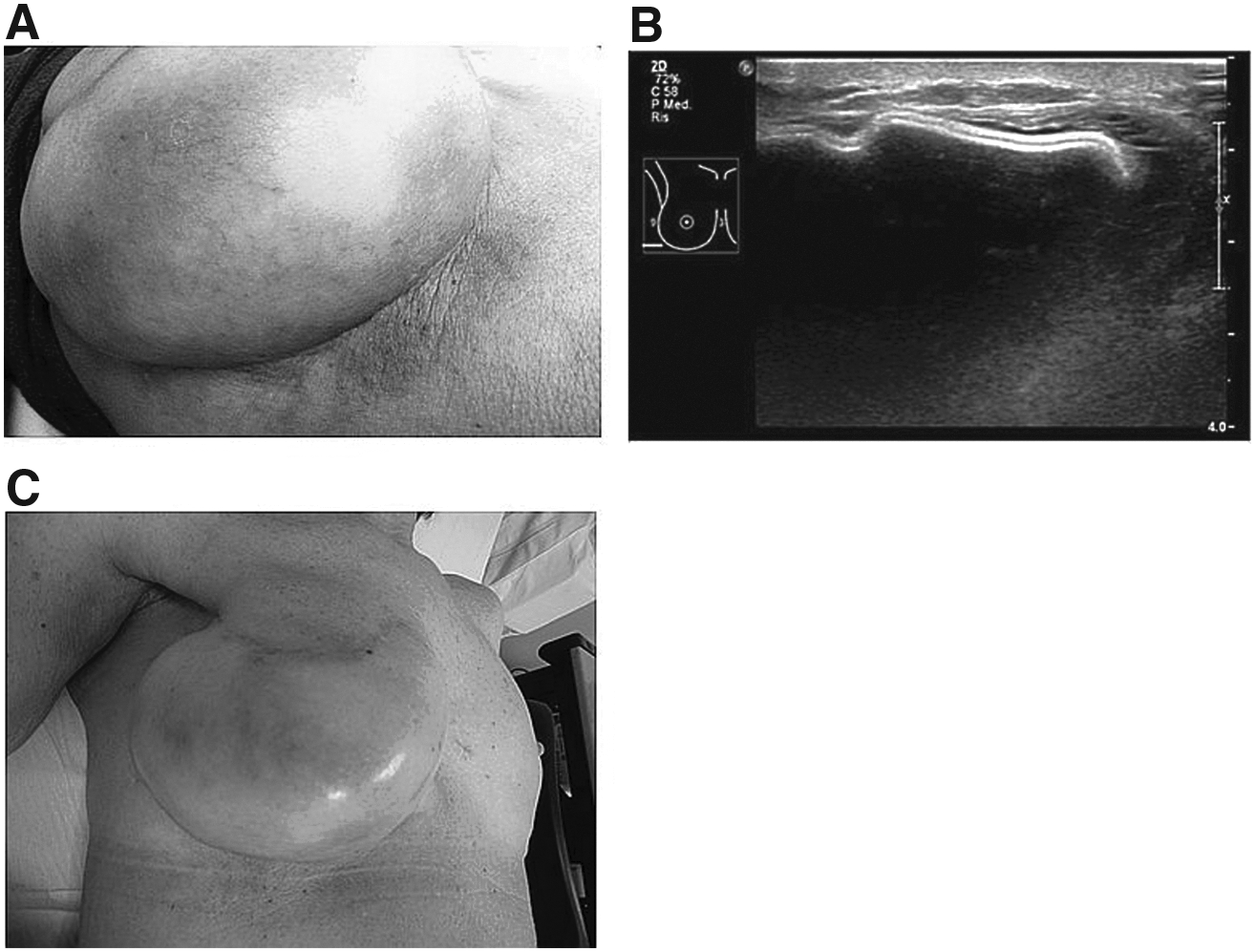
Clinical images relative to a patient with a late infection (910 d from surgery) and probable implant infection (index case).
Blood tests (complete blood count, c-reactive protein, fibrinogen) confirmed severe inflammation and leukocytosis and a poor control of diabetes mellitus (glycemia >180). On ultrasound scan, no peri-prosthetic collection nor subcutaneous involvement were detected, thus preventing echo-guided fluid sampling for microbiologic investigation (Fig. 1B). Empiric treatment with oral amoxicillin-clavulanate 875/125mg tid plus clindamycin 300mg tid was administered at home for 15 d. [16,18]. The patient subsequently improved and was monitored at outpatient visits 5, 21, 60 and 90 d thereafter (Fig. 1C). On the last evaluation in November 2013, Baker III capsular contracture was present without further signs of infection.
Consistent detection of late prosthesis infections during prospective patient follow-up/case series and time of infection after surgery
Following the observation of the index case, we decided to start a prospective observation. The present analysis regards the observed infection series between February 1, 2009, and May 31, 2013. During this observation period, 78 infections were recorded out of 766 surgical procedures (832 implants), (10.2%). No patient had more than one infectious episode or more than one implant infected. Among the 78 patients with infection, 53 (67%) cases occurred ≤60 DFS (early prosthetic infections), and 25 (33%) (age 56.36±10.80 yrs) occurred beyond 60 d and were defined as late prosthetic infections (Fig. 2).
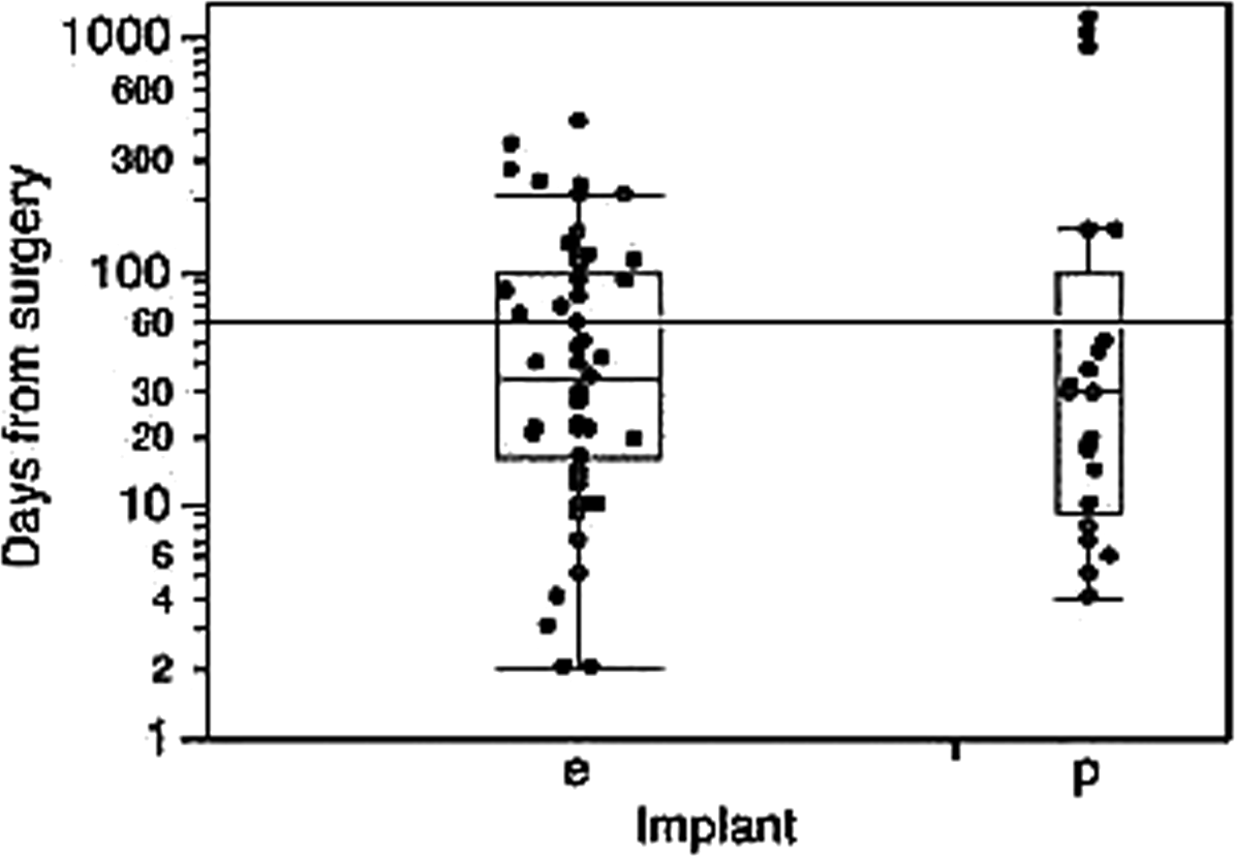
Timing of infection (days from surgery) in all implants (expanders=e; prostheses=p). All prospectively detected sequential cases, both early and late, are shown. The black line indicates the threshold between early and late infections (60 DFS).
Late infections occurred after a median 145±313.721 DFS. Among them, 10 of 25 (40%) cases occurred beyond 182 DFS (>6 mo), and in three (12%) patients this occurred >2 y after surgery (very late infections) (Tables 1–2).
DFS=days from surgery.
DFS=Days from surgery; Early infection=(0–60 DFS); Late infection=(>60 DFS).
When adopting this grading system, the majority of late implant infections were classified as proved (Fig. 3A). The proportion of proved late infections (21/25, 84%) was substantially greater when compared with the proportion of proved early infections observed during the same time frame in the same patient cohort (34/53, 56%, p=0.0144, Fisher exact test) (Fig. 3B).
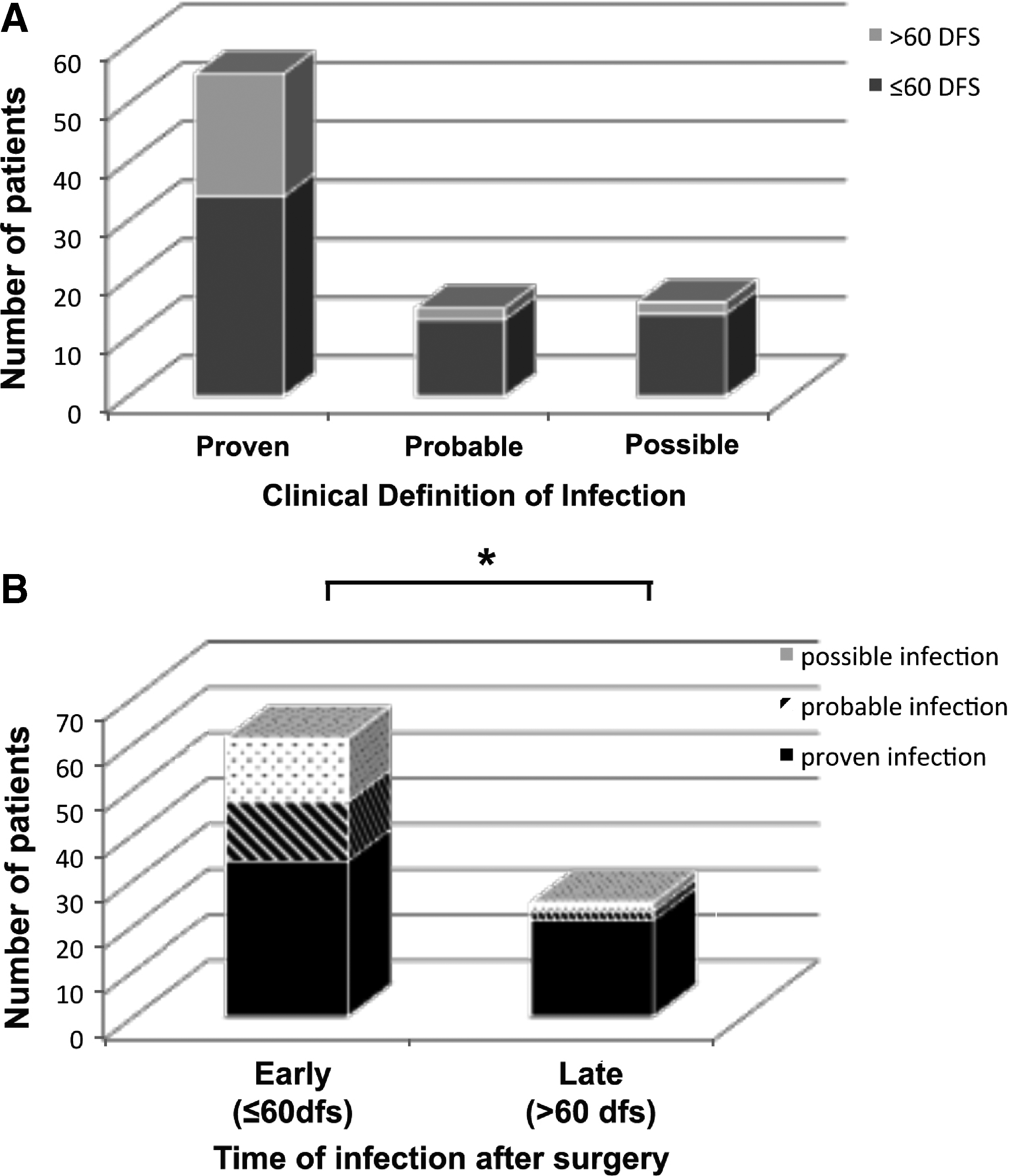
Microbiologically proved implant infections prevail among late implant infections.
Infecting microorganisms and host factors associated with late infections
With regard to the microorganisms responsible for the 25 late implant infections, microbiological evaluation of prosthetic material, peri-prosthetic fluid/tissues, or both, resulted in the isolation of staphylococci in 20 cases, with one infection sustained by Pseudomonas aeruginosa (Fig. 4). Intra-operative microbiologic sampling (implant or capsule) was negative or not done in four patients. Among gram-positive cocci, Staphyloccus aureus was prevalent (13/20, 65%) with a wide majority of isolated strains being methicillin susceptible (13/20, 84,6%, Fig. 3). Staphyloccus epidermidis was isolated less frequently (7/20, 35%) and was exclusively represented by methicillin-resistant strains.
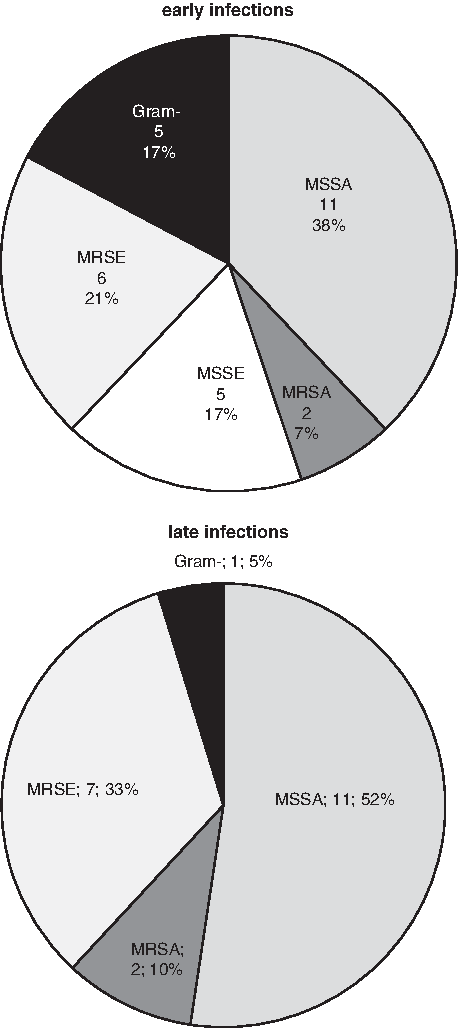
Distribution of microbiological isolates from clinical samples in patients with early and late implant infections. No difference is observed in the relative proportion of isolates from proved early (n=29) and late (n=21) infections. Gram-negative rods (G -); Methicillin-resistant Staphylococcus epidermidis (MRSE); Methicillin-sensitive Staphylococcus epidermidis (MSSE); Methicillin-resistant Staphylococcus aureus (MRSA); Methicillin-sensitive Staphylococcus aureus (MSSA);
Among the microorganisms isolated from proved early implant infections (Fig. 4), a greater frequency of gram-negatives was observed (five isolates, five implants; three P. aeruginosa, one Morganella morganii, one Serratia marcesens) compared with late infections. In addition, differences in the frequency of MSSE (five isolates), Methicillin-sensitive Staphylococcus aureus (MSSA) (11 isolates) and of Methicillin-resistant Staphylococcus epidermidis (MRSE) (six isolates) were observed in early infections (Fig. 4). Overall the distribution of isolates was different in late infections compared with early infections (χ2=2969.827, p<0.001, chi-test). We next analyzed host and implant factors associated with late infection. Among patients undergoing radiotherapy in this group, (i.e. either before and after implant surgery), late infection occurred substantially later when radiotherapy was administered after surgery and before implant infection compared with any radiotherapy administered at any time before implantation (p=0.0325 Mann-Whitney U-test) (Fig. 5A). With regard to type of implant, infections occurred later in patients undergoing replacement of expanders with a prosthesis, compared with those who had infections following positioning of expanders (Fig. 5B, p=0.0042 Mann-Whitney test). No effects were observed for chemotherapy or for patient age.

Distribution of late infections according to timing of radiotherapy and type of implant.
Following the diagnosis of infection (either possible, probable, or proved) all the patients were treated with antibiotics in the attempt to preserve the implant pocket. The numbers and proportions of saved and removed implants are shown in Table 3. Among 22 patients with early infections, in six cases (27%) implant salvage was obtained associating implant replacement (expander - >prosthesis) with antibiotic treatment. Treatment was successful in a greater proportion of patients with early infections compared with late infections (41.5% vs. 12%, respectively, p=0.009, Fisher exact test) (Table 3). This greater proportion of success in implant salvage was not because of greater proportions of possible or probable infections cured among early infections (p=n.s), but rather to a greater success in treating proved early infections (Table 3).
Saved=Retaining of the implant following antibiotic treatment, 6 prosthesis-implant substitutions; Stats=Fisher exact test, two-tailed; n.s.=not significant.
Discussion
The present work describes a prospectively collected single-center case series evaluation and shows that, when based on clinical definition, late breast implant infection after reconstruction for breast cancer has high frequency. Indeed, 33% of all implant infections at our center occurred beyond 2 mo from surgery (i.e., late implant infections). Among these late infections, 40% occurred >6 mo from surgery with 12% occurring very late (>24 mo).
Until recently, a relevant proportion of the literature on infection of prosthetic devices for breast reconstruction focuses attention to a short observation time (<30 d) corresponding to the standard period for the definition of SSI [3,6,9,10]. A subsequent epidemiological definition suggested in order to avoid underreporting, to extend the “early” period up to 1 y after surgery thus encompassing distinct clinical stages in the case of breast reconstruction. In other areas of prosthetic surgery including cardio-thoracic or orthopedic surgery, 60–90 d are routinely considered the threshold to define early versus late prosthetic device infection [26–28].
Altogether, these points inspired the present analysis with definition of late and very late infection also in breast implant surgery. The present prospective finding that a substantially greater proportion of late implant infections (>60 DFS) was microbiologically proved when compared with early infections (0–60 DFS) supports the need to set a clinical threshold at or around 60 DFS for defining breast implant infections. This difference may be because of an increased occurrence in early infections of possible confounding factors (hematoma, seroma, liponecrosis) that are more frequently associated with the immediate post-surgical course.
Further support for a clinical defined threshold at 60 DFS between early and late infection is provided by the detection of a substantial difference in implant salvage with antibiotics alone or combined treatment with greater success rates in early implant infection.
Among late implant infections, those occurring after prosthetic reconstruction presented later compared with expander implant. This may be attributable to inherent management differences between implant types. First, expanders have a shorter mean survival, because they are eventually substituted with definitive prostheses. It is therefore expected that their late infection risk does not exceed the time of their replacement with a definitive prostheses. Secondly, patients with breast reconstruction and implanted expanders, opposite to those with definitive prosthesis, undergo periodic repeated percutaneous implant inflations or other medical or surgical procedures, which may at times increase the risk of infection. Finally, timing of radiation therapy in patients with expanders or prosthesis may contribute to the observed difference [29,30]. Patients requiring radiotherapy are irradiated after chemotherapy, thus accounting for late expander infection. On the contrary, radiotherapy on a definitive prosthesis is uncommonly administered and may be required only in some cases of very late cancer disease recurrences.
In the present analysis, a wide majority of gram-positive cocci was isolated, in agreement with previous observations suggesting a skin origin of infections. Overall, a balanced presence of methicillin-susceptible and -resistant strains (11 MSSA versus seven MRSE+two MRSA) was observed. The relatively low prevalence of MRSA is in agreement with data from late orthopedic prosthetic infections [31], and with their lower prevalence in late (as compared with early) implantable cardiac device infections [32]. The frequency of MRSE in the present work is in line with findings from late implant infections in cardiac and orthopedic surgery series [32–34]. Although methicillin resistance is increasing in the community, healthcare-associated acquisition of these pathogens cannot be completely ruled out here during repeated post-surgical outpatient visits in patients who may need chemotherapy or expander inflation. Medical procedures at locations far from the implanted sites may cause bacteremia and hematogenous seeding of infection and at times represent a risk for bacterial infection of implants [4,13,34–37].
The microorganisms identified in the present study represent prevalent seeding from cutaneous locations and suggest staphylococcal bacteremia as a seeding mechanism, whereas origin from other colonized districts (e.g., oral or enteric sources) seems less likely. With regard to the possible prevention of late breast implant infection after surgical reconstruction, unlike other areas covering cardiac and orthopedic implants [38,39], there is so far insufficient evidence to recommend any prophylactic strategy. This area of clinical uncertainty may determine management difficulties, including advising patients on how to care for the expanders/prostheses and counseling for procedures that may cause skin trauma and bacteremia even months to years after implant surgery.
In conclusion, prospective monitoring reveals that late implant infections after breast cancer reconstruction are far from being rare, representing up to one third of implant infections and may be salvaged less frequently compared with early infections. Thus, an increased attention is warranted towards surveillance programs for late and very late breast implant infections and for their prevention using 60 DFS as time threshold. The increasing number of women living with permanent prosthetic breast implants after reconstructive surgery for breast cancer would thus allow for the planning of multi-center studies addressing risk, prevention, and treatment.
Footnotes
Acknowledgments
The authors are indebted to Dr. Michela Adami, Dr. Stella Leone for providing help and for patient referral, and to Dr. Giuseppe Canavese, Dr. Alessandra Catturich, Dr. Carlo Vecchio, and Prof. D. Friedman—all at our institution—for help with the patients.
Author Disclosure Statement
All authors concurred to the work and approved the manuscript. There are no conflicts of interest for all authors actual or potential. No outside funding was received.