
Abstract
Abstract
Background:
Antimicrobial resistance results from a complex interaction between pathogenic and non-pathogenic bacteria, antimicrobial pressure, and genes, which together comprise the total body of potential resistance elements. The purpose of this study is to review and evaluate the importance of antimicrobial pressure on the development of resistance in a single surgical intensive care unit.
Methods:
We reviewed a prospectively collected dataset of all intensive care unit (ICU)-acquired infections in surgical and trauma patients over a 6-y period at a single hospital. Resistant gram-negative pathogens (rGNR) included those resistant to all aminoglycosides, quinolones, penicillins, cephalosporins, or carbapenems; resistant gram-positive infections (rGPC) included methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE). Each resistant infection was evaluated for prior or concomitant antibiotic use, previous treatment for the same (non-resistant) organism, and concurrent infection with the same organism (genus and species, although not necessarily resistant) in another ICU patient.
Results:
Three hundred and thirty resistant infections were identified: 237 rGNR and 93 rGPC. Infections with rGNR occurred frequently while receiving antibiotic therapy (65%), including the sensitive form of the subsequent resistant pathogen (42.2%). Infections with rGPC were also likely to occur on antimicrobial therapy (50.6%). Treatment of a different patient for an infection with the same resistant pathogen in the ICU at the time of diagnosis, implying potential patient-to-patient transmission occurred more frequently with rGNR infections (38.8%).
Conclusion:
Antimicrobial pressure exerts a substantial effect on the development of subsequent infection. Our data demonstrate a high estimated rate of de novo emergence of resistance after treatment, which appears to be more common than patient-to-patient transmission. These data support the concept that efforts to limit antimicrobial usage will be more efficacious than enhanced isolation procedures when trying to reduce antimicrobial resistance.
Pitted against microbial genes, we have mainly our wits.
—Joshua Lederberg, PhD
A
These advances in genetic analysis are valuable and serve as the starting point for further therapeutic advances. However, clinicians today have only one true weapon available in the fight against antimicrobial resistance: The thoughtful control of antimicrobial pressure during necessary anti-infective therapy. We therefore proposed a pragmatic evaluation of the varying degrees of antimicrobial pressure, which may contribute to the development of resistance with the intention of interpreting these data in light of the current evidence for the antimicrobial resistome.
Patients and Methods
Approval for this study was obtained from our local Institutional Review Board prior to initiation. A prospective cohort of all infectious episodes occurring in general surgery, trauma, and transplantation patients were reviewed for intensive care unit (ICU)-acquired infections caused by resistant organisms between December 2001 and November 2007. These patients are managed by two separate critical care teams (surgical and trauma) but are located in the same physical space within the hospital.
All ICU-acquired infections caused by resistant organisms were considered index infections. Resistant gram-negative pathogens (rGNR) were defined as those resistant to all aminoglycosides, all quinolones, all penicillins (including β-lactam/β-lactamase inhibitor combinations), all cephalosporins, or all carbapenems by clinical microbiology laboratory testing. Resistant gram-positive pathogens (rGPC) included methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE). These definitions are meant to represent any clinical resistance pattern (which we consider as involving at least one antimicrobial class) that may affect antimicrobial choice. We are intentionally not using the U.S. Centers for Disease Control and Prevention (CDC) definition for multi-drug–resistant pathogens because we believe this is a clinically distinct scenario from the general development of resistance [2].
Index infections were analyzed on a per infection basis. Infections caused by multiple resistant organisms were treated as a single index infection. For each index infection, the dataset was evaluated for antibiotic exposure related to treatment for an active infection including: Previous or concomitant antibiotic usage, previous treatment for the same (non-resistant) organism, and concurrent treatment of an infection with the same, resistant organism in another ICU patient. This last data element was used as a surrogate for potential patient-to-patient transmission. Data were also recorded for antibiotic usage that did not correspond to treatment for an active infection (e.g., peri-operative surgical prophylaxis or prolonged prophylaxis such as that required for open fracture management).
Classification
A hierarchical grading system ranging from least contributory to most contributory antibiotic exposure was created to evaluate each index infection. Classes of organisms for the purposes of this study included gram-positive pathogens and gram-negative pathogens. This grading system included (from least contributory to most contributory):
1. Previous systemic antibiotics with coverage for a different class than the resistant infection; 2. Previous systemic antibiotics with coverage for the same class as the resistant infection; 3. Concomitant systemic antibiotics with coverage for a different class than the resistant infection; and 4. Concomitant systemic antibiotics with coverage for the same class as the resistant infection (Fig. 1).
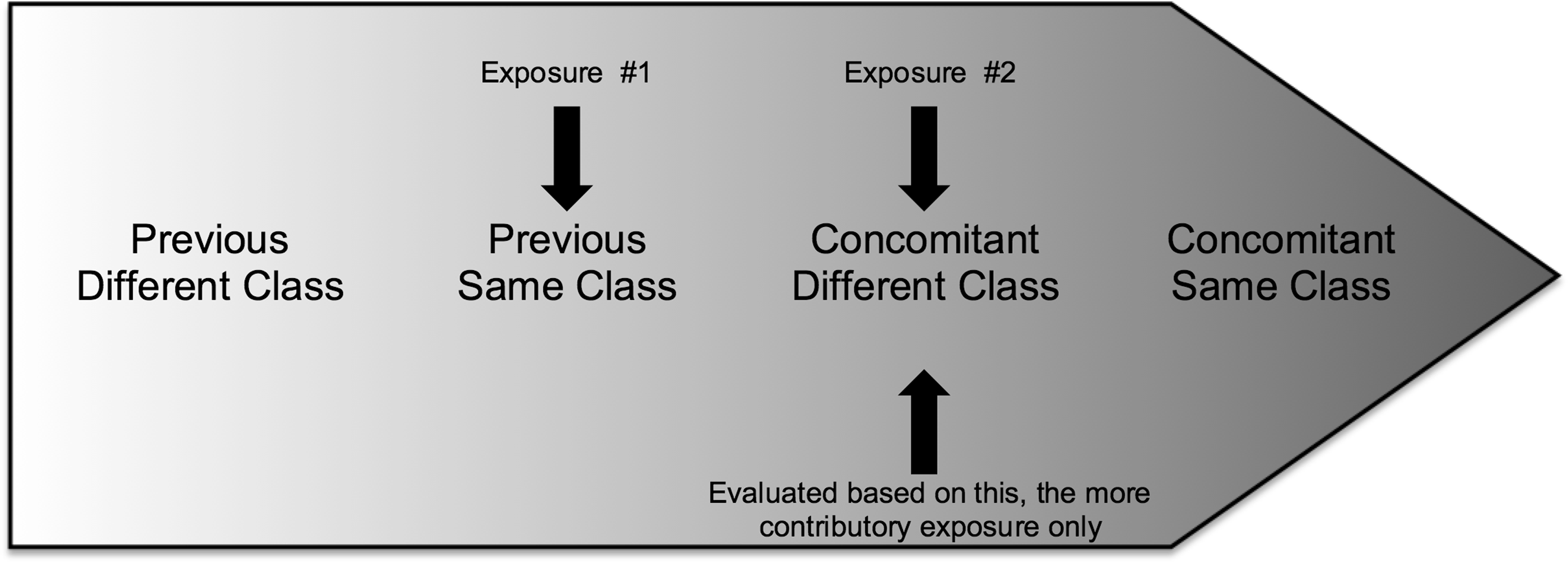
Hierarchical grading scheme of antibiotic exposure. Arrows indicate direction of theoretical contribution of antibiotic exposure to each index infection. Index infections with more than one exposure were labeled as having been exposed to only the most contributory category.
Previous antibiotic exposure was evaluated by considering all antibiotics given prior to development of each index infection, including those given for infections occurring outside the ICU. Concomitant systemic antibiotics were those being administered at the time of diagnosis of an index infection. “Different class” was assigned to antibiotics that covered classes of organisms other than that of the index infection. “Same class” was assigned to antibiotics that included coverage for the same class of organism as the index infection. These categories were mutually exclusive and each index infection was categorized according to the “most contributory” antibiotic exposure classification. Only the most contributory category was recorded.
Previous treatment for the same, non-resistant organism (genus and species) in each patient with an index infection was also evaluated. This included infections occurring before and after ICU admission but before acquisition of the index infection. Last, presence of concurrent infection with the same, resistant organism in another ICU patient was determined for each index infection. Unlike the antibiotic exposure hierarchy described above, these categories were not mutually exclusive.
Statistical analysis
Data manipulation and statistical analysis were performed with SAS 9.1.3 (SAS Institute Inc., Cary, NC). Proportion of sites and organisms within each class of index infections were calculated. Demographics and pre-infection risk factors were tabulated and reported. Binary categorical variables were compared with χ2 analysis or Fisher exact test; continuous variables were compared using Student t test. Significance was considered p≤0.05.
Results
Three hundred thirty ICU-acquired infections were identified over the study period: 237 gram-negative and 93 gram-positive infections. The most common resistant isolates and infectious sites for rGNR and rGPC are listed in Table 1. A full list of rGNR isolates and infectious sites are included in Supplementary Table S1 (Supplementary Date are available online at www.liebert.pub/sur).
Total infections for each listed organism class may be lower than the total number of resistant organisms present at each infectious site. The unit of measure for this study is at the infectious site, not organism level.
Only the most common organisms (≥10% of recovered rGNR organisms) are listed. A complete list is included in Supplementary Table S1.
VRE=vancomycin-resistant enterococci; MRSA=methicillin-resistant Staphylococcus aureus; SSI=surgical site infection; rGPC=resistant gram-positive infections; rGNR=resistant gram-negative infections.
Patient demographics, pre-infection comorbidities, and associated illness severity scores are listed in Table 2. The distribution of resistant pathogens was uneven across many characteristics in a generally predictable manner, e.g., the predominance of rGNR among patients with ventilator dependence where ventilator-associated pneumonia was more common.
Baseline serum creatinine≥2.0 mg/dL.
Before infection.
Packed red blood cells or platelets transfused before initiation of treatment for infection.
rGNR=resistant gram-negative infections; rGPC=resistant gram-positive infections; SD=standard deviation; WBC=white blood cell count.
Patients who received no pre-infection antibiotic exposure of any kind but developed rGPC or rGNR subsequently were 6.5% and 1.3%, respectively. For patients who developed rGPC infections, 14% received only peri-operative prophylactic antibiotics, whereas 8.6% received only prolonged prophylactic exposure. Peri-operative antibiotics were the only exposure in 3.8% of subsequent rGNR infections. Eleven percent of rGNR infections followed prolonged prophylaxis.
Results for the possible origins of the infection with resistant pathogens are listed in Table 3. Whereas this table includes overall results of our antibiotic classification schema, these categories are not mutually exclusive. The majority of patients developed infection with resistant pathogens while actively receiving antimicrobial therapy. The presence of an infection with the same pathogen in a different patient, i.e., implying potential for patient-to-patient transmission, was less common.
Only the most common organisms (≥10% of recovered rGNR organisms) are listed.
ICU=intensive care unit; rGPC=resistant gram-positive infections; VRE=vancomycin-resistant enterococci; MRSA=methicillin-resistant Staphylococcus aureus; rGNR=resistant gram-negative infections.
The results of our hierarchical classification schema are listed in Table 4, further broken down by antibiotic exposure. Resistant gram-positive and gram-negative infections occurred most frequently during treatment with the same class of antibiotic that would be used to treat the subsequent resistant infection. Resistance appears to have arisen through selective pressure in the individual patient.
rGPC=resistant gram-positive infections; rGNR=resistant gram-negative infections.
Discussion
There are more bacteria on the planet than any other form of life combined. Whereas pathogenic bacteria make up only a small fraction, their ability to generate, acquire, and transmit genetic elements responsible for antimicrobial resistance is astonishing. As clinicians, we are able to track the development and spread of these resistance elements, yet knowledge is of little consolation to our patients. We are left fighting infections with tools that the effectiveness of which is being eroded actively. At the moment, however, the thoughtful use of antimicrobial agents remains the only tool we have to fight infection.
Resistant pathogens that cause infections in the ICU originate in a limited number of ways. First, they might be transmitted from another patient. Second, they might be selected due to treatment of a non-resistant form of the same pathogen. Third, they may be selected during treatment for other pathogens. Finally, they may have been brought into the ICU already present in the patient microbiome and unable to be classified. Our study is an attempt to describe the roles of these different resistance pathways on the development of infection in a single surgical ICU. To accomplish this, we developed a novel hierarchical classification system, which was created for this study and that has not been described previously, to categorize the degree of antimicrobial pressure that may have been present at the time a resistant infection was identified.
Many of our current antimicrobial agents are actually derived from those naturally produced by non-pathogenic bacteria [3]. These resistance mechanisms are particularly important, in fact essential for self-protection in the very organisms that produce these antimicrobial agents [1]. These resistance mechanisms may “escape” and be subsequently “captured” by pathogenic bacteria through horizontal gene transfer [1,3].
Considering that non-pathogenic organisms harbor the bulk of the resistome, local environmental factors, including those of the host microbiome, may be vital to the development of subsequent resistance in pathogenic species [4]. The ICU environment has been demonstrated to serve as a secondary reservoir for resistant pathogens. Reservoirs (such as ICU sinks) may also contaminate health care workers who then serve as a vector for new patient contamination, transmission of resistance elements though horizontal gene transfer, and ultimately infection [5]. Clearly there is a complex interplay between patient microbes, health care workers, and the environment, which serves as a mechanism for the storage and transmission of resistance genes. In fact, we discovered that our ICU sinks might be a substantial secondary reservoir for resistant pathogens, including carbapenem-resistant Enterobacteriaceae, and have since taken steps to eradicate these reservoirs.
Our data suggest a rate of patient-to-patient transmission that is greater than that reported by Grundmann et al. [6], Cepeda et al. [7], and Halwani et al. [7]. Moreover, estimates for individual isolates may be greater [9]. Our estimated rate of cross-transmission appears higher in spite of aggressive mandatory screening for VRE and MRSA coupled with isolation of patients testing positive for either organism. However, there is some evidence that isolation alone may not reduce rates of infection because of cross-transmission [7,10]. Given greater estimated rates of cross-transmission we may have expected greater mortality rates. Although not designed with this end point in mind, our crude mortality for both resistant infections in our study was between 32% and 35%. These rates are similar to those ranges reported in the literature [8,11,12]. These findings are somewhat conflicting and suggest that perhaps our grading scale overestimates the degree of cross-transmission. Without confirmatory genetic testing, our data on this matter should be treated with caution, because they are only estimates.
Mutations acquired during antimicrobial treatment represent the major source of all clinically relevant resistance [13]. De novo resistance may be acquired via spontaneous mutagenesis or activation of latent resistance mechanisms. For example, given that the error rate for deoxyribonucleic acid (DNA) polymerase is approximately 1 base pair in every 109 base pairs, the expected mutation rate for Escherichia coli is 1 mutant per every 200 cell divisions [1]. Therefore, in an active infection the number of potential mutant strains may be substantial. Whereas the majority of these mutations are silent or fatal, a small number may confer some selective advantage [1,4]. Furthermore, environmental factors including oxidative stress from antimicrobial exposure, starvation, or induction of the SOS response may actually accelerate the mutation rate [1,13,14]. These mutations may be particularly damaging when they occur in so-called proto-resistance genes: Namely, genes responsible for metabolic processes that may confer antimicrobial resistance when altered [1]. These represent the microbiologic parallel to proto-oncogenes in oncology. Latent resistance mechanisms may also be activated in the setting of antimicrobial pressure, such as those observed in the response of some Pseudomonas aeruginosa strains to ciprofloxacin exposure [13,15]. Indeed, our data demonstrate that in all cases at least 50% of resistant pathogens were isolated after periods of antimicrobial stress active against the same species that was isolated. In the case of rGNRs at our institution, it appears that these cases mostly arise as de novo resistance within the same organism rather than transfer from other infected patients, although this may be exaggerated. The pattern for rGPC's is less clear.
There are several limitations to our study. First, these data reflect practice and resistance patterns at a single tertiary-care institution, therefore, our results may not be generalizable broadly. Second, as a retrospective analysis, our results are additionally subject to the standard observation bias inherent in this type of study. Third, antibiotic use strategies were variable during the study period and include some periods of antibiotic cycling. It is unclear to what extent these patterns may have influenced our findings. Fourth, because of the hierarchical ranking system used to evaluate antibiotic therapy, patients who fit the previous and current antibiotic treatment categories were treated as current antibiotic treatment only, thus underestimating the contribution of prior antibiotic therapies to resistance. In patients who received both, it is unclear which may have been more contributory; the high rates seen among those occurring during antibiotic treatment may be because of an effect from those in the group who had also received previous treatment. Finally, because this was a retrospective dataset analysis, no genotyping strategies were used and our estimation of patient-to-patient transmission is exaggerated at best.
Conclusion
We have categorized the emergence of resistant infections based upon the degree of associated antimicrobial pressure and have reflected upon these patterns in light of the antimicrobial resistome. Overall our data demonstrate that antimicrobial pressure appears to have a substantial influence on the development of antimicrobial resistance resulting in high rates of de novo resistance. We support efforts to limit the use of all antimicrobials unless there is objective evidence of infection or in life-threatening scenarios.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.