
Abstract
Abstract
Background:
Patients with intra-abdominal sepsis and associated bacteremia have a high mortality rate. However, outcomes studies in this population are limited, in part because of the small numbers of such patients. The objective of this study was to describe characteristics of critically ill patients with secondary blood stream infection (BSI) of intra-abdominal origin and identify predictors of mortality.
Methods:
This retrospective, single-center study evaluated patients admitted between January 2005 and January 2011 with bacteremia because of an intra-abdominal source. Patients were included if they met criteria for severe sepsis based on International Classification of Diseases, 9th Revision (ICD 9) codes for acute organ dysfunction, had a positive blood culture, had at least one ICD 9 code indicative of an intra-abdominal process, and had a confirmed or clinically suspected intra-abdominal infection (IAI) within 72 h of the blood culture. Chart review was performed to confirm the presence of these criteria and also the absence of any other potential source of bacteremia. Data were collected on patient demographics, BSI source, source control procedure details, microorganisms isolated, and antibiotics administered. Multivariable logistic regression analysis was performed to identify independent predictors of mortality.
Results:
Three hundred six patients with BSI were identified, of which 108 episodes were deemed to be of intra-abdominal origin. Gram-negative organisms comprised 43% of blood isolates, followed by gram-positives (33%), anaerobes (14%), and yeast (9%). Appropriate antimicrobial therapy was administered in 71% of patients. The overall mortality rate was 27.8%. As compared with survivors, non-survivors were older, more likely to have underlying COPD or asthma, and have renal or metabolic failure (p<0.05 for all). Among non-survivors, adequate source control was obtained less frequently (64% vs. 91%, p=0.002) and median time to appropriate antibiotics was longer (23 h vs. 4 h, p=0.004). Logistic regression analysis revealed inadequate source control (p=0.002) and inappropriate antibiotics (p=0.016) to be independently associated with mortality.
Conclusions:
Critically ill patients with a BSI of abdominal origin are at high risk for mortality. Failure to achieve adequate source control and administration of inappropriate antibiotics were independent predictors of mortality. Thus, these represent potential opportunities to impact outcomes in patients with complicated IAI.
I
Although obtaining blood cultures in patients with IAI is not routinely recommended, such patients have a worse prognosis than those patients with IAI who do not have a complicating bacteremia. Bacteremia from a high risk source such as abdominal and lower respiratory tract has been independently associated with in-hospital mortality [4]. Furthermore, mortality rates of up to 63% have been reported in patients who develop a bacteremia of intra-abdominal origin [5]. Many patients with IAI who have an associated bacteremia present with evidence of severe sepsis or septic shock. However, current IAI guidelines [3] cannot make highly definitive statements describing optimal therapy for these severely ill patients because of a lack of prospective studies. Describing a critically ill group of patients with IAI based on an objective measurement, such as bacteremia, provides a different avenue into looking at management, outcome variables, and predictors of mortality.
There have been numerous studies published evaluating predictors of mortality in patients with IAI [6–11]. However, studies investigating predictors of mortality in patients with BSI of intra-abdominal origin are sparse. Two cohort studies have investigated a total of 1,399 patients with BSI and deemed 114 to be from an intra-abdominal source [5,12]. The reported mortality rates in these studies were 36% and 63%. Acute Physiology and Chronic Health Evaluation (APACHE) II score, the number of evolving organ dysfunctions, older age, and occurrence of acute renal failure were independent risk factors for mortality in these two studies. Interestingly, receipt of appropriate antibiotics was not identified as a predictor of outcome, but findings may be limited as a result of the small sample sizes and definitions applied. In contrast, in virtually all studies in which it has been examined, inadequate or delayed source control is a consistent risk factor for an adverse outcome in patients with cIAI [3,10,11].
Thus, many questions remain unanswered for these severely ill patients with IAI. The objective of this study is to describe the characteristics of patients with BSI of intra-abdominal origin who have severe sepsis or septic shock and determine if independent predictors of mortality can be identified in those patients.
Patients and Methods
This retrospective, single-center cohort study was performed at Barnes-Jewish Hospital, a 1,250-bed tertiary care academic medical center which is the major teaching hospital for the Washington University School of Medicine. This facility has an emergency department with approximately 100,000 adult patient visits per year. The Washington University School of Medicine Human Research Protection Office and the Protocol Review and Monitoring Committee approved this study. The Barnes-Jewish Hospital medical informatics system was queried to identify patients who were admitted between January 1, 2005, and January 1, 2011, and met inclusion criteria. To be included in this study, patients had to meet criteria for severe sepsis based on discharge International Classification of Diseases, 9th Revision, (ICD 9), Clinical Modification codes for acute organ dysfunction, which have been described previously [13]. Organs of interest included the heart, lungs, kidneys, bone marrow (hematologic), brain, and liver. Patients also had to have a positive blood culture and at least one ICD 9 code indicative of an intra-abdominal process. In patients with multiple episodes of bacteremia, the first occurrence was utilized for the timing of bacteremia. Patients were considered to have septic shock if vasopressors (norepinephrine, dopamine, epinephrine, phenylephrine, or vasopressin) were initiated within 24 h of the time of blood culture collection. Patients who transiently received vasopressor agents related to procedures or use of anesthesia were not considered to meet this criterion of septic shock.
Eligible patients meeting these criteria were then organized in the database according to the highest number of intra-abdominal related ICD 9 codes and assessed accordingly. In order to increase the probability of identifying a patient with a suspected IAI, patients with ≥three intra-abdominal related ICD 9 codes and were selected for further review. Each patient chart was then reviewed to confirm correct ICD 9 codes and the presence of a clinically suspected IAI within 72 h of the positive blood culture. Once a patient was deemed to have a BSI of intra-abdominal etiology, a second reviewer assessed the patient. If there was a discrepancy between the results of the first and second review, the patient was excluded. Reasons for excluding a patient included identification of an extra-abdominal source of the BSI, a failure to identify an obvious source of the BSI, if the positive blood culture was assessed as being because of a contaminant, if key documentation was unclear or missing, or if a decision was made to pursue a non-aggressive approach to treating the patient within 48 h of the positive BSI.
Electronic medical records were searched to identify demographic data, microbiology data, antimicrobial agents received, presence of health care–associated risk factors, surgical procedures, and the specific source of the IAI. Baseline characteristics collected included age, gender, race, history of congestive heart failure, pulmonary disease, diabetes mellitus, chronic liver disease, malignant disease, and end-stage renal disease requiring dialysis. A modified APACHE II score [14] was calculated to estimate the severity of illness based on clinical data present within 24 h of the positive blood culture. Additional electronic inpatient and outpatient medical records available for all patients in the BJC Healthcare System (13 hospitals and multiple community health locations) were reviewed to determine prior antimicrobial exposure and surgical history.
All definitions were chosen before initiation of the study. Community-acquired IAI was defined as infection occurring less than 48 h after hospital admission, with the absence of any health care–associated community-onset risk factors. Health care–associated community-onset was defined as an IAI in a patient with the presence of at least one of the following health care risk factors: Presence of invasive device at admission, history of methicillin-resistant Staphylococcus aureus (MRSA) infection or colonization, history of surgery, hospitalization, or dialysis in the previous 12 mo, or residence in a long-term care facility, nursing home, or rehabilitation facility. Heath-care-associated hospital-onset was defined as an IAI onset greater than 48 h after hospital admission [3].
Adequacy of source control was assessed independently by two board-certified surgeons (JEM and EH). A patient was considered to have had inadequate source control only if both surgeons concurred with that opinion; if the opinions differed, the patient was designated as having had adequate source control. Adequate source control was defined as having a timely percutaneous, endoscopic, laparoscopic, or open abdominal procedure to drain infected fluid collections, debride infected tissues, and control ongoing enteric or other drainage producing peritonitis. Procedures were considered timely if they were performed within 24 h of the discovery of the intra-abdominal source of infection eliciting the bacteremia. Patients who had temporizing procedures performed, such as damage control laparotomy or temporary abdominal drainage, were considered to have had adequate source control if widespread enteric leakage was alleviated and a plan was established for a more definitive procedure within the next 24–72 h. In patients with infected pancreatic necrosis, temporizing measures were considered adequate source control as long as further procedures to control sepsis were to be undertaken. Patients were considered to have had inadequate source control if no source control procedure was undertaken, if the procedure was delayed by more than 24 h, or if the operative procedure did not result in control of the ongoing infectious process. For instance, a patient with an intestinal leak and generalized peritonitis who was treated with drainage of the peritoneal cavity but with no plan for subsequent definitive control of the source of the leakage, would be assessed as having had inadequate source control. Subsequent recurrence or development of a further intra-abdominal infection was not utilized as a criterion for judging adequacy of the index source control procedure; the assessment was based only on the expectation that the procedure would achieve the objectives listed above. The designation that a patient had inadequate source control was not an opinion about surgical judgment or approach, because the patient's condition or technical issues may have precluded performance of a definitive source control procedure.
Appropriate antimicrobial therapy was defined as an initially prescribed antimicrobial regimen with activity against the identified pathogen based on in vitro susceptibility testing and administration within 24 h of blood culture collection. Multi-drug-resistant isolates for gram-negative bacteria were defined as a bacterial isolate with in vitro resistance to at least three or more anti-pseudomonal antibiotics, which included cefepime, piperacillin-tazobactam, ciprofloxacin, imipenem or meropenem, or an aminoglycoside (gentamicin, tobramycin, or amikacin).
Continuous data were analyzed using the Student t-test for parametric data and the Mann-Whitney U test for non-parametric data. Categorical data were analyzed using the Chi-square or Fisher exact test. A p value of less than 0.05 was considered to indicate a statistically significant difference. A univariate analysis was performed excluding nine patients who did not undergo a source control procedure. Logistic regression was used to identify risk factors independently associated with mortality. Variables significant at a p value ≤0.2 in the univariate analyses entered into the stepwise multivariable logistic regression model. The most prudent model for the predictors of mortality was computed and its fit was tested with the AUROC and the Hosmer-Lemeshow goodness-of-fit test. Statistical analysis was completed by using the SPSS software, version 18.0 (SPSS, Inc., Chicago, IL).
Results
A total of 1,310 patients were identified as having a positive blood culture, ICD 9 codes for severe sepsis and ≥1 ICD 9 code for an intra-abdominal process. A total of 306 patients had ≥three intra-abdominal related ICD 9 codes and were selected for further review. The most common reason for exclusion (n=104) was the likelihood that an extra-abdominal source accounted for the bacteremia. Alternative sources of infection included 64 catheter related BSI, 27 pneumonias, seven urinary tract infections, and six cardiothoracic infections. In 37 patients, no definitive source of the BSI was identified. Thirty patients were excluded because of missing data and 17 were excluded because of suspected contaminated blood culture. Finally, 10 patients were excluded because a non-aggressive course of treatment was selected within 48 h of the positive blood culture. The final analysis included 108 patients with BSI from an intra-abdominal source (Fig. 1).
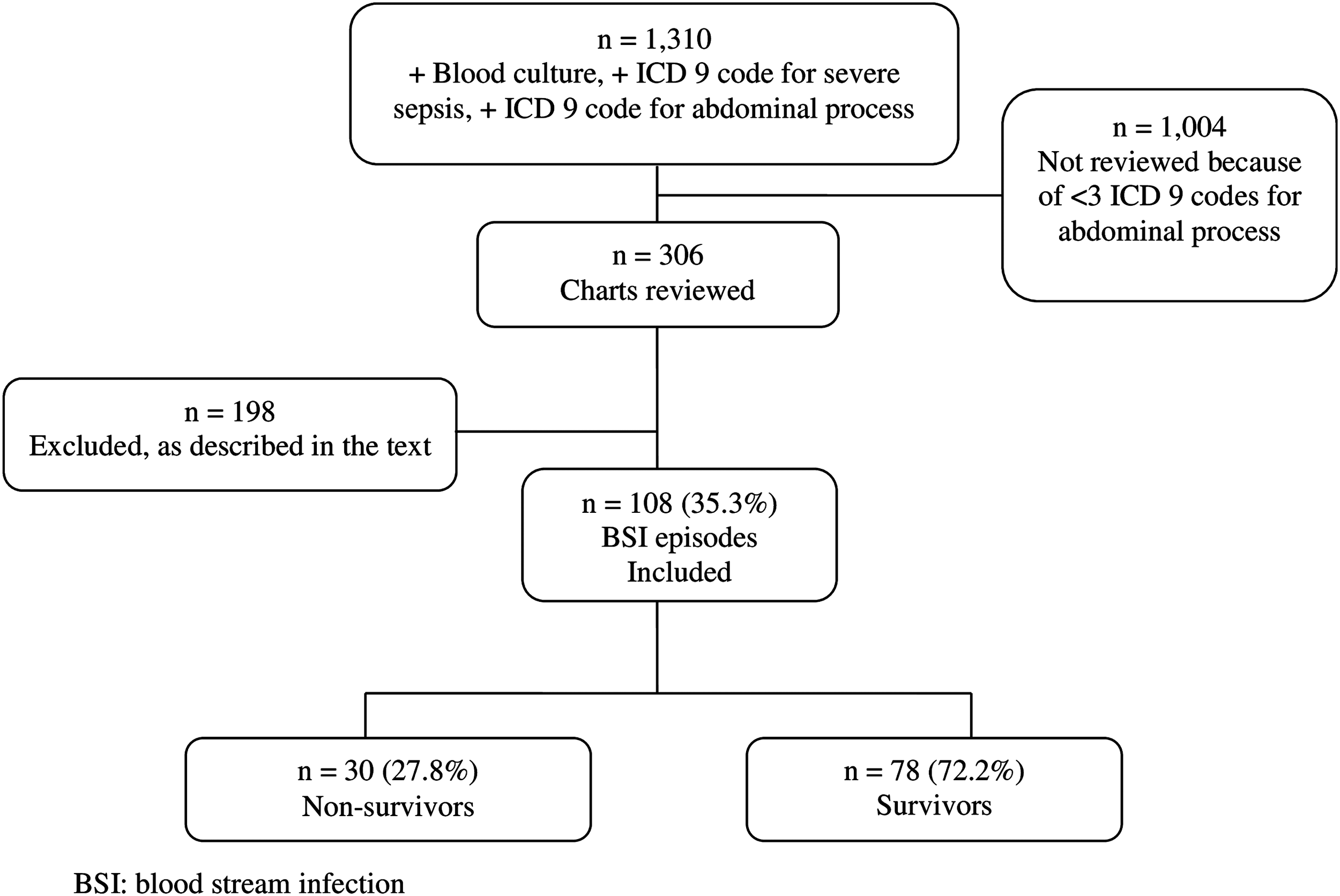
Study profile.
The study patients had a median age of 60 y, with 56% being male and 44% being female. The majority of patients were Caucasian (74%). The median modified APACHE II score for the patients was 20. Seventy-two percent of patients were mechanically ventilated and 94% were admitted to the ICU during their hospital stay. Most patients had at least one documented organ failure. IAI was confirmed by computed tomography in 83% of patients. Of the 108 patients, 82 (76%) had an intra-abdominal culture obtained during admission. Forty-seven patients had an intra-abdominal culture obtained within 72 h of their positive blood culture, with 43 (52.4%) being positive and four being negative (4.8%). The median overall hospital length of stay was 27.5 d (Table 1).
values reported as n (%) unless otherwise specified.
value reported as median (inter-quartile range).
APACHE=Acute Physiology and Chronic Health Evaluation; IAI=Intra-abdominal infection; ICU=Intensive care unit; CT=computerized tomography.
Eight percent of patients had an IAI acquired in the community, 25% had a health care–associated, community onset IAI, and 67% had health care–associated hospital-onset IAI. The frequencies of various health care–associated risk factors are detailed in Table 2. Overall, 43% of patients had received antimicrobials in the previous 90 d (Table 2). Forty-eight patients underwent an operative procedure before developing an IAI, as detailed in Table 3.
values reported as n (%) unless otherwise specified.
value reported as median inter-quartile range.
MRSA=methicillin-resistant Staphylococcus aureus; VRE=vancomycin-resistant Enterococcus.
Patients may have had ≥one initial surgical or invasive procedure
Values reported as n (%).
other: one exploratory laparoscopy, one gastric bypass, one gastrojejunostomy, one oophorectomy and cystotomy repair, one percutaneous gastrostomy, one splenectomy.
The most common presumed source of infection were gastrointestinal perforations (30%), gastrointestinal necrosis or ischemia (19%), and intra-abdominal abscess (18%) (Table 4). All but nine patients had secondary peritonitis and underwent a source control procedure. Among these nine patients, four had SBP, one had cholangitis, one had a suspected anastomotic leak, one had a small bowel obstruction managed non-operatively, one had infected ascites of unknown origin, and one had a suspected peritoneal dialysis (PD) catheter infection. The most common source control procedures were placement of a percutaneous drain (32%) and large bowel resection (26%). An adequate source control procedure was considered to have been performed in 83 of the 99 patients who underwent such a procedure (84%) (Table 5).
Values reported as n (%)
Note: Some patients had ≥one BSI infection source.
Other perforation: one gallbladder, one gastric.
Other infection: two infected hepatic infarcts, one PD catheter, one toxic megacolon, one infected ascites with unidentified source, one pelvic infection, one bladder perforation.
BSI=blood stream infection; PD=peritoneal dialysis.
Values reported as n (%)
Patients may have undergone more than one source control surgical or invasive procedure
Others: one ulcer closure with omental patch, one diverting loop ileostomy, one transverse colotomy repair, one liver abscess aspiration, one resection of ischemic omentum, one anastomotic repair
ERCP=Endoscopic retrograde cholangio-pancreatography.
Gram-negative organisms were the most commonly isolated organisms, (61/141, 43%) with Escherichia coli being the most common microorganism cultured (25/141, 18%). Enterococcus spp. was the most common gram-positive organism isolated (26/141, 18%). Anaerobes were present in 14% of the BSIs and fungal isolates were found in 9%. A polymicrobial BSI was noted in 20% of patients (Table 6). VRE was isolated in 9% of the BSI episodes, MDR gram-negative bacilli in 4%, and MRSA in 4%.
Values reported as n (%), *p=0.005
BSI=bloodstream infection; VRE=vancomycin resistant Enterococcus; MDR=multi-drug resistant; MRSA=methicillin-resistant Staphylococcus aureus.
Appropriate antibiotic therapy was administered to 71% of the patients. The most common initial antimicrobials prescribed were vancomycin (71%) and piperacillin-tazobactam (44%), followed by metronidazole (32%), and cefepime (25%). Of note, 8/13 (62%) of bacteremias because of VRE and 9/13 (69%) because of Candida sp. received inappropriate antibiotics (Table 7).
values reported as n (%),*p value<0.05
MDR=multi-drug resistant; MRSA=methicillin-resistant Staphylococcus aureus; VRE=vancomycin resistant Enterococcus.
The overall mortality rate was 27.8%. The non-survivors were older, more likely to have underlying chronic obstructive pulmonary disease (COPD) or asthma, and have renal or metabolic failure. Survivors more frequently had E. coli BSI, had an adequate initial source control procedure, and had a shorter time to receipt of appropriate antimicrobial therapy (median 4 h versus 23 h) (Table 8). Stepwise logistic regression analysis revealed that inadequate source control (p=0.002) and inappropriate antibiotics (p=0.016) were independently associated with mortality (Hosmer-Lemeshow p=0.943, AUROC=0.776.) (Table 9).
Values reported as n (%) unless otherwise noted.
Values reported as median inter-quartile range.
BSI=blood stream infection; VRE=vancomycin resistant Enterococcus; MRSA=methicillin-resistant Staphylococcus aureus; APACHE=Acute Physiology and Chronic Health Evaluation; ICU=intensive care unit.
Hosmer-Lemeshow p=0.943, AUROC=0.776.
AOR=adjusted odds ratio; CI=confidence interval; APACHE=Acute Physiology and Chronic Health Evaluation.
Discussion
The aim of this study was to describe characteristics of patients with IAI who have concomitant BSI, and identify predictors of mortality in this critically ill population. To our knowledge, this is the first study to date that has assessed the timing and appropriateness of antimicrobial therapy as well as the contribution of inadequate source control in a group of critically ill patients with an IAI and an associated bacteremia.
Our study findings were similar to De Waele et al. [5], in that approximately 20% of patients had a polymicrobial BSI secondary to an intra-abdominal source. Fewer patients received appropriate antimicrobial therapy in this current investigation compared with the study of De Waele et al. (70% versus 91%). This is likely because of the differences in the appropriate antimicrobial therapy definition, for which we required administration within 24 h of blood culture collection, compared with 48 h in the previous study. We did not require a positive intra-abdominal culture in addition to a positive blood culture for inclusion, as was done in the study by De Waele et al., because intra-abdominal cultures were not obtained at our institution in all cases and are not necessary for the clinical diagnosis of an IAI. However, to ensure that the BSI was most likely because of an intra-abdominal source, all clinical information was reviewed by at least two separate investigators to exclude any cases where the BSI was potentially related to an alternative source.
The mortality rate was substantially lower in the current study compared with that observed in the study by DeWaele et al. (28% versus 63%). This may have been because of differences in baseline comorbidities and slight differences in the severity of acute illness. In addition, widespread dissemination and implementation of the Surviving Sepsis Campaign guidelines because the previous study may have contributed to the lower mortality rate noted in our study. De Waele et al. found age and renal failure to be associated with a greater mortality rate. Although these factors were both statistically significantly different in our univariate analysis, they were not shown to be independent predictors of mortality in the multivariable analysis. In a study by Raymond et al. [15], the mortality rate for surgical patients with IAI complicated by BSI was 20%, although measures of severity of illness in this subgroup (n=46) were much lower than those observed in the present study. The objective of this analysis by Raymond et al. was to assess the importance of BSI among infected surgical patients, and included both IAI and pneumonia. The presence of a BSI was not shown to be an independent predictor of death in surgical patients, but they noted that patients with BSI had a greater severity of illness and mortality rate.
Inadequate source control and administration of inappropriate antibiotics were independent predictors of mortality in this analysis. Lack of adequate source control was the strongest predictor of mortality, which is consistent with other analyses of complicated IAIs, [3,10–11]. However, what actually represents “adequate” source control is controversial. In general, we considered the goal of source control to be drainage of infected fluid collections, debridement of infected tissue, and definitive measures to avoid further contamination, as outlined by Marshall [16]. However, it has been increasingly recognized in recent years that less invasive techniques can constitute adequate source control. For instance, percutaneous drainage of an infected fluid collection is well accepted as a means of source control, as long as the goal of elimination of a substantial amount of the microbial inoculum and prevention of ongoing contamination can be achieved [3]. Indeed, some less invasive techniques now being utilized, such as laparoscopic drainage without resection for Hinchey Class III and IV diverticulitis [17] might have been considered to be inadequate source control just a few years ago. There is also an appreciation that damage control laparotomy is an acceptable measure for initial management of many critically ill patients with intra-abdominal sepsis, even though this obligates further procedures for definitive management [18].
For this study, therefore, we attempted to restrict the definition of inadequate source control. We only applied this determination to those cases in which there was a clear failure to perform a timely source control procedure (defined as within 24 h of discovery of an intra-abdominal process for which source control was needed), or the use of a temporizing procedure without any apparent plan to carry out a definitive procedure (e.g., initial percutaneous drainage of an abscess in a patient with bowel necrosis with no subsequent bowel resection). We also required the independent concurrence of two board-certified general surgeons that there was inadequate source control. It is likely that this led to an underestimate of the degree to which inadequate source control was present in these critically ill patients. Nonetheless, most patients did undergo procedures that seemed in accordance with contemporary surgical practice, so it is unlikely that the narrowness of this definition resulted in major skewing of the results.
Inappropriate antibiotics were administered more commonly in non-survivors and remained as an independent predictor of mortality in the multivariable analysis. This finding is consistent with multiple studies that have demonstrated an association between inappropriate antibiotic use and increased risk of therapeutic failure and mortality in the context of IAI [19–22]. This finding emphasizes the need to tailor empiric therapy utilizing patient specific factors in order to optimize outcomes for patients with IAI. The time to appropriate antimicrobial therapy was shorter amongst survivors in the univariate analysis, this but was not independently associated with mortality in the multivariable analysis. The inability to demonstrate such a finding in this cohort of patients with secondary BSI related to an IAI may have been because of the relatively small sample size particularly if the major effect of inadequate source control overwhelmed the opportunity of seeing a smaller difference related to timing of antimicrobial therapy in this relatively small study. Indeed, in a large study of septic shock patients performed by Kumar et al., an ∼8% increased risk of death for every 1 h delay in the administration of appropriate antibiotics relative to the onset of hypotension was observed [23]. Approximately 30% of patients included in this study had an intra-abdominal source of infection and subgroup analysis of this population was consistent with the overall findings.
The majority of patients in this study had health care–associated hospital onset infections (67%) followed by health care–associated community onset infections (25%). Gram-negative bacilli (most commonly E. coli and K. pneumoniae) and gram-positive cocci (most commonly Enterococcus spp.) caused the majority of the BSIs in our study, followed by anaerobes and yeast; these are also the common pathogens reported in most studies of IAIs. Although Pseudomonas is an organism associated with many hospital-acquired infections, it was only present in 3.5% of the BSIs in our study; this is consistent with its low incidence (<15%) in cIAI in general [3]. Regardless, most patients in our study were initially started on an anti-pseudomonal agent (piperacillin-tazobactam, cefepime, meropenem). Similarly, MRSA isolation was rare (4%) and consistent with previous studies, and yet the majority of patients in this cohort received an agent with MRSA activity. Multi-drug resistant gram-negative organisms were also isolated infrequently (4.3%), with no differences found between survivors and non-survivors.
Although Candida spp. and VRE collectively accounted for only 18% of the microorganisms isolated, they were responsible for more than half [n=17/31 (55%)] of the occurrences of inappropriate antimicrobial therapy. It is also noteworthy that 9/13 (69%) Candida isolates were non–Candida albicans spp. Intra-abdominal infections because of Candida and enterococci have previously been associated with increased morbidity and mortality [8,24,25] although debate exists as to whether this relation is causal or simply an association [26]. However, when considering these findings in conjunction with data demonstrating reduced survival when inappropriate antibiotics are administered, it would appear that empiric therapy against these potential pathogens should be considered in the appropriate patient populations in order to optimize outcomes. However, empiric therapy is not recommended in all patients with cIAI, and should only be utilized in patients with substantial risk factors for these pathogens, as suggested in the SIS/IDSA guidelines [3].
There are several limitations worth noting. The retrospective design of this study is one such limitation. Interpretation of diagnoses, infection sources, and surgical procedures depends on the accuracy of documentation; thus, some data of the data collected may have been incorrect. Reliance on ICD 9 codes to identify patients initially may have led to the unintentional exclusion of some patients because of the potential for incorrect coding. The majority of the included patients were healthcare-associated hospital-onset, limiting the less well represented populations. The observational design also limits the opportunity to determine why certain antimicrobial regimens were prescribed initially. Because this study was conducted at a single center institution, the results may not be applicable to other institutions. Finally, as with any observational study, it is not possible to infer a causal relation between mortality and the patient, microbial, and management data obtained in this study.
Overall, however, we believe that this study provides important information about critically ill patients with IAI and an associated bacteremia. Despite improvements in therapy, mortality was still high in these patients, with nearly three of 10 critically ill patients succumbing to an intra-abdominal infection associated with BSI. Although we identified several differences between survivors and non-survivors, including differences in age, underlying organ failure, and time to appropriate antibiotic delivery, the major finding was that inadequate source control and inappropriate antibiotics were major independent risk factors associated with increased mortality in these patients. We would conclude that despite the critically ill nature of these patients, performance of a timely source control procedure and administration of appropriate antibiotics is still of primary importance in managing patients with IAI, and potentially of even greater importance in these severely-ill patients. Source control should not be delayed in the false hope that prolonged medical management alone will somehow improve the patient's physiological condition such that overall risk of mortality because of this disease will be lessened.
Footnotes
Author Disclosure Statement
No competing financial interests exist.