
Abstract
Abstract
Background:
Gram-positive microorganisms were the main causative organisms of orthopedic surgical site infections (SSI); however the rising incidence of multiple drug resistant Acinetobacter baumannii (MDR-AB) infections in orthopedic operations causes a great concern because of their limited array of therapeutic options.
Objective:
Our objective was to remark the changing microbiology in orthopedic SSI and to evaluate the MDR CHROMagar Acinetobacter media for screening of MDR-AB.
Methods:
Aspirated pus samples were collected from infected wounds of 100 patients in the orthopedics unit of El-Helal Hospital, samples were cultured on conventional media and MDR CHROMagar Acinetobacter media, the reveled MDR-AB colonies were subjected to polymerase chain reaction (PCR) to detect blaOXA-51 like gene.
Results:
Out of 100 infected wounds SSI cases represented 90/100 (90%) according to CDC 2013 definitions. Staphylococcus aureus was the dominant organism 40/90 (44.4%) (P value 0.038), all S. aureus isolates were methicillin-resistant Staphylococcus aureus (MRSA), followed by Klebsiella pneumoniae 22/90 (24.44%) and Acinetobacter 15/90 (16.67%). Implant was highly associated with SSI cases 80/90 (89%). Also, prolonged hospital stay >7 d was significantly associated with SSI 69/90 (77%) (p=0.001).
Conclusion:
Staphylococcus aureus was the main causative organism of orthopedic SSI (44.4%), whereas A. baumannii represented only (16.67%) of the causative organisms. MDR Acinetobacter CHROMagar reduced the turnaround time for screening of MDR-AB.
S
Surgical-site infection is defined by the U.S. Centers for Disease Control and Prevention (CDC) as a proliferation of pathogenic micro-organisms which develop in an incision site either within the skin and subcutaneous fat (superficial), musculo-facial layers (deep), or in an organ or cavity, if opened during surgery [2]. Risk factors of orthopedic SSI could be modifiable or non- modifiable, patient or procedure related factors [3].
Gram-positive organisms were the major causative organisms of surgical site infections, although the rising incidence of multiple drug resistant Acinetobacter baumannii (MDR-AB) infections in orthopedic operations causes a great concern because of their limited array of the therapeutic options [4].
“MDR CHROMagar Acinetobacter is a chromogenic media for detection and isolation of MDR Acinetobacter species by using a color-change identification method. Acinetobacter species appears as red colonies.” The growth of most gram-positive cocci and yeast is inhibited [5].
Screening of SSI risk factors and remarking the microbiology of orthopedic SSI are important to determine the proper peri-operative prophylactic antibiotic regimens. Utilization of rapid detection methods such as chromogenic media of MDR organisms may affect the outcome and guide towards the proper treatment.
Patients and Methods
This study involved 100 infected patients who were admitted in the orthopedic unit of El-Helal Hospital. All patients received antibiotic peri-operative prophylaxis regimen according to the hospital antimicrobial policy. (i) The patient's history of allergy was considered. (ii) Third-generation parenteral Cephalosporins, Gentamicin in addition to Ampicillin–Sulbactam were given, in the case of skin colonization with methicillin-resistant Staphylococci, Vancomycin was prescribed. (iii) Prophylaxis was given within 30 min to 1 h before incision. (iv) One dose was sufficient yet additional doses were given for operating procedures longer than 4 h or in case of significant blood loss, the antibiotic prophylaxis continued up to 48 h.
Aspirated pus from surgical site infections was collected aseptically (surgical or traumatic wounds) after immediate transportation all samples were processed at the Department of Medical Microbiology and Immunology of El-Helal Hospital.
All samples were cultured on blood agar, MacConkey agar (Oxoid Co. England) and MDR CHROMagarAcinetobacter™ plates (CHROMagar, France) (containing additional supplement CR102, which allows the growth of carbapenem-resistant strains) were prepared from dehydrated base media (AC092B) and supplement (AC092S) according to manufacturer's instructions. All culture plates were incubated aerobically at 35°C for 24–48 h. Multi-drug-resistant CHROMagar Acinetobacter™ plates have been reformulated to produce colonies with a distinct red color of MDR-AB, whereas other gram-negative and positive bacteria and yeast are mostly inhibited. Identification of all isolated organisms was done by conventional biochemical reactions.
Antimicrobial susceptibility testing was performed by the disc diffusion method (Modified Kirby Bauer technique) using Muller Hinton agar, aerobic incubation at 35°C for 16–18 h. Antimicrobial discs, Imipenem (10 mcg), Meropenem (10 mcg), Gentamicin (10 mcg), Ciprofloxacin (5 mcg), Amikacin (30 mcg), Cotrimoxazole (25 mcg), Cefepime (30mcg), Cefotaxime (30 mcg), Cefotaxime+Clavulanic acid (30/10 mcg), Aztreonam(30 mcg), Ceftazidime (30 mcg), Ceftazidime+Clavulanic acid (30/10 mcg), Amoxacillin-Clavulanic acid (20/10mcg), and Cefoxitin (30 mcg) were obtained from Oxoid Co. (Oxoid Limited, Basingstoke, Hampshire, England). Phenotypic screening and confirmation of extended spectrum β lactamases (ESBL) production was done according to (CLSI, 2013) using the combined disc tests. Cefoxitin (30 mcg) disc was used to detect MRSA according to (CLSI, 2013) [6].
Multidrug resistance was defined in this analysis as resistance to three or more representatives of the following classes of antibiotics: Fluoroquinolones (ciprofloxacin), extended-spectrum cephalosporins (ceftazidime), aminoglycosides (amikacin, gentamicin), and carbapenems (imipenem, meropenem) [7].
Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 Staphylococcus aureus ATCC 29213 were used as reference strains for susceptibility testing according to Clinical and Laboratory Standards Institute (CLSI.2013) guidelines and interpretations [6].
Molecular confirmation of A. baumannii was done by detection of blaOXA-51 like gene performed by PCR as described by Turton et al [8]. DNA was extracted by heating method of Vaneechoutte [9]. Briefly, strains were grown on blood or agar plates and were incubated overnight at 37°C to isolate single colonies. After incubation, four or five discrete colonies of each strain were suspended in 50 MCl of sterile distilled water in a 0.5-mL Eppendorf tube. To lyse the cells and extract DNA, the tubes were heated for 10 min at 95°C, then cooled on ice, and were centrifuged in a micro centrifuge (Microfuge Lite; Beckman) at 12,000 rpm for 30 sec to remove the cell debris. These crude DNA extracts were kept on ice for immediate use or frozen at −20°C until the rest of the PCR reagents were prepared [9].
DNA amplification was performed in 25 mcl reaction volumes with 3 mcl of extracted DNA, 12.5 pmol of each primer (blaOXA-51-like F 5'-TAA TGC TTT GAT CGG CCT TG-3', blaOXA-51-like R 5'-TGG ATT GCA CTT CAT CTT GG-3'), and 1.5 U of Taq DNA polymerase in 1 mcl PCR buffer containing 1.5 mM MgCl2 (QIAGEN Inc., Chatsworth, CA) and 200 mcM of each dTPs. Conditions of the thermal cycler (Primus 25 advanced, PEQLAB, Erlangen, Germany) for PCR was the following: 94°C for 3 min, and then 35 cycles at 94°C for 45 sec, 57°C for 45 sec, and 60°C for 1 min, followed by a final extension at 72°C for 5 min [8].
The amplified products were detected by agarose gel electrophoresis using 1.5% agarose (BIORAD), stained with ethidium bromide and examined by UV (ultraviolet) transillumination (Sigma). Positive blaOXA-51like fragment was detected at 369 bp.
Statistical analysis was done using the Statistical Package for the Social Sciences (SPSS) Version 15 (SPSS Inc., Chicago, IL). Data was presented by percentages for categorical variables. Mean±SD for quantitative data. Tests of significance were used to assess difference between two study groups; t-test was used for assessing significant difference between two study groups in quantitative variables. The chi-square test was used to test for statistical significance of categorical variables and was set at a p value≤0.05.
Results
The study included 100 infected patients admitted in El-Helal Hospital, 90/100 (90%) defined as deep surgical site infections cases according to CDC 2013 definitions, in (SSI) cases infection occurred within 30 d after the operative procedure and involved deep soft tissues of the incision (e.g., fascial and muscle layers). All SSI cases had a purulent drainage from the deep incision plus one or more of the following criteria: (i) A deep incision that spontaneously dehisced or is deliberately opened by a surgeon and was culture-positive, and (ii) the patient had at least one of the following signs or symptoms: Fever (>38°C), localized pain, or tenderness.
Risk factors associated with SSI are shown in Figure 1. Implant was highly associated with (SSI) cases 80/90 (89%). Prolonged Hospital stay>7 d was also associated with (SSI) 69/90 (77%) (p value=0.001). The prolonged hospital stay was mainly because of infections but also type of surgery and the patient general condition contributed in prolongation of the length of stay.
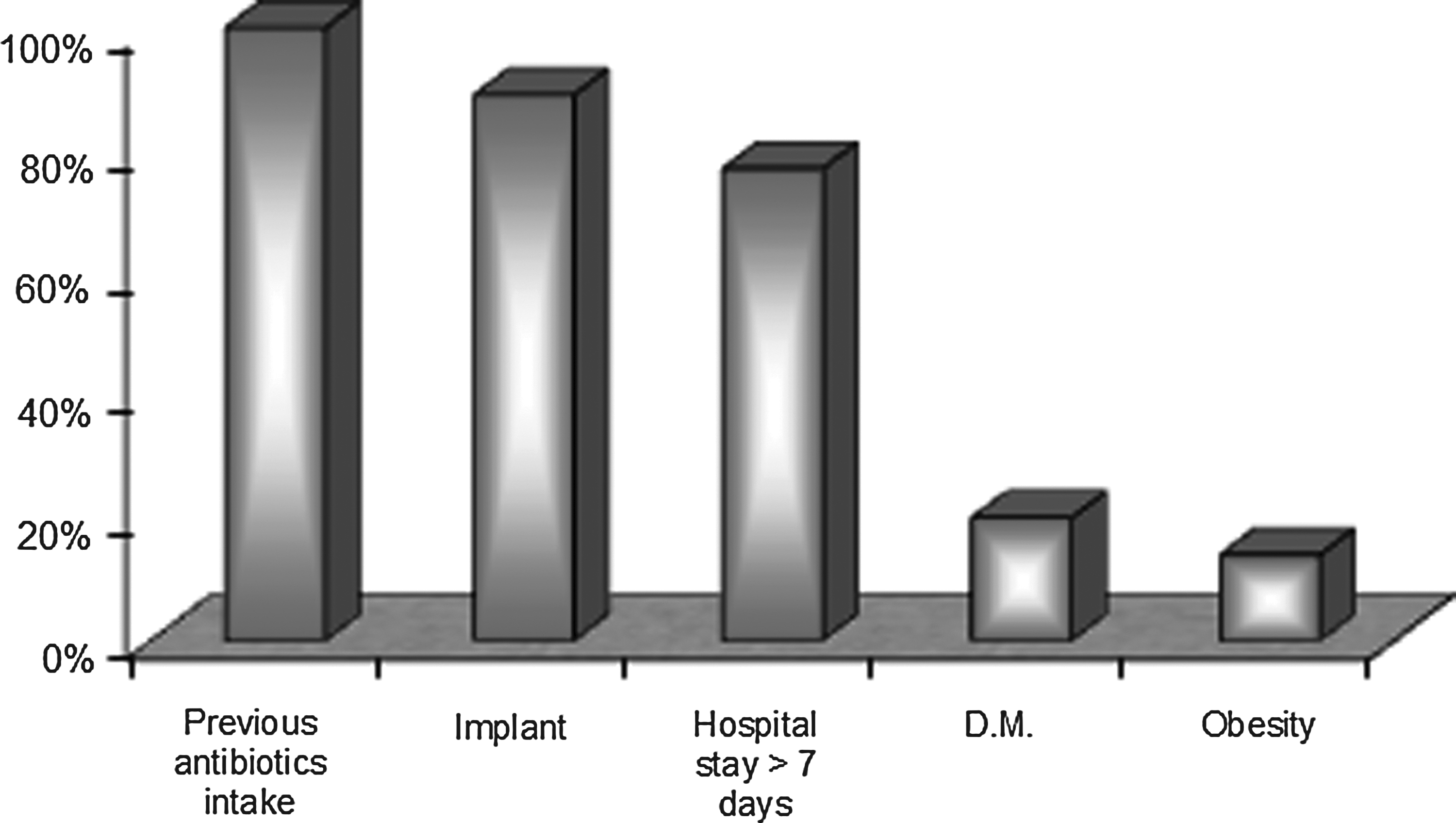
Risk factors among SSI cases.
Distribution of organisms according to types of surgery is shown in Table 1. The most common type of surgery among the SSI cases was fracture femur fixed by plate and screw 32/90 cases (35.5%), which was significantly infected by S. aureus (47.5%) (p value 0.049).
Antibiotic susceptibility testing of 119 isolates revealed from SSI cases showed 14/15 (93.33%) isolates of Acinetobacter spp. were MDR Acinetobacter, 40/40 (100%) isolates of S. aureus were MRSA, 23/57 (40.35%) were ESBL-producing Enterobacteriaceae whereas 2/57 (3.51%) of Enterobacteriaceae were carbapenams resistant. Antibiotic susceptibility testing of all A. baumannii isolates is shown in Table 2.
From all samples that were inoculated directly onto the CHROMagar, 14 Acinetobacter isolates showed the typical red colonies morphology of MDR Acinetobacter spp. Molecular confirmation of identification was done by PCR by detecting the bla OXA-51 like gene which was positive in 13/14 (93%) meaning that they were A. baumannii.
Statistical evaluation of CHROMagar inoculation against the disc diffusion method as a reference method to detect MDR-AB was: Sensitivity 92.85%, specificity 100%, positive predictive value 100%, negative predictive value 98.7% and accuracy 98.88%.
Discussion
The purpose of this study was to study the changing microbiology of orthopedic SSI, and to evaluate the MDR CHROMagar Acinetobacter media. Out of 100 infected patients; implant contributes to 80/90 (89%) of SSI cases, which coincides with a study performed at Massachusetts General Hospital, Boston, MA, in 2008, which found a significant association between SSI and the use of temporary external fixation (p<0.001) [10].
In our study, prolonged hospital stay>7 d was significantly associated with SSI 69/90 (77%) (p value=0.001). This coincided with a study performed by NHS hospitals in England, April 2006–March 2011, which found that the trends in rate of SSI in orthopedic surgery between 2004–2005 and 2010–2011 inpatients rates for SSI in hip and knee replacement surgery have been in decline since 2004–2005 because of the decreasing length of hospital stay [11].
Staphylococcus aureus was the dominant organism 40/90 (44.4%) (P=0.038). All S. aureus isolates were methicillin-resistant S. aureus (MRSA), followed by K. pneumonia 22/90 (24.44%) and Acinetobacter 15/90 (16.67%), in concordance with a study performed by NHS hospitals in England, April 2006–March 2011, which found that S. aureus continuing to account for the majority of SSIs in the mandatory orthopedic categories (37%) [11].
On the contrary, Singh et al. in 2010 in India showed that gram-negative infections continue to be a major threat because gram-negative pathogens were isolated from 75.6% of cases. E. coli was the most common pathogen (28.5%), followed by K. pneumoniae (25%), whereas A. baumannii represented (7%) [12].
Antibiotic susceptibility testing showed that 23/57 (40.3%) of Enterobacteriaceae isolates were ESBL producers. A study performed by Seni et al. in Kampala, Uganda, showed that ESBL producers were more than three quarters of Enterobacteriaceae. Another study performed by Stephen et al. in 2010 showed low rates (14% to 22%) of ESBL producers among Enterobacteriaceae in hospitalized surgical patients [13,14].
The increased ESBL-producing Enterobacteriaceae can be attributed to the empirical use of third-generation cephalosporin, usually in combination with another drug, such as gentamicin, in almost all hospitalized patients. Another factor is the lack of antimicrobial resistance surveillance in surgical wards in developing countries.
Our antibiotic susceptibility results by disc diffusion method concerning Acinetobacter isolates showed that 93% were found to be MDR Acinetobacter. In King Saud University, Shehata in 2012 found that all Acinetobacter spp. (100%) clinical isolates were multi-drug resistant [15]. Before 2005 the rate of carbapenams-resistant A. baumannii in Europe, North America, South America, and Asia ranged between 0% and 40%. But in most studies after 2005, the rate of resistance was greater than 50%. The higher rates of resistance were found in Iran (63%), Italy (62, 5%), China (55, 6%), Turkey (53, 7%), and Korea (51%) [16].
MDR Acinetobacter CHROMagar was 92.85% sensitive and 100% specific for MDR A. baumannii when compared with the disc diffusion method. Also, in 2010 Akers et al. showed that CHROMagar Acinetobacter was 75% sensitive and 100% specific for A. baumannii [17].
A study performed in the Department of Epidemiology and Public Health, University of Maryland School of Medicine, by Ajao et al. in 2011 showed that CHROMagar Acinetobacter was 100% sensitive for Acinetobacter isolates; compared with MacConkey agar, which was 89% sensitive for Acinetobacter spp. and 91% sensitive for MDR-A. baumannii [5]. Another study by Wareham et al. in 2011 for identification of MDR-Acinetobacter reported that the addition of the MDR supplement to CHROMagar Acinetobacter prevented the growth of carbapenams susceptible A. baumannii [18].
Conclusion
Infection control measures are mandatory to decrease orthopedic SSIs. Restricted antibiotic policy should be applied to control the bacterial resistance spread. Pre-admission screening of MRSA may be helpful for proper application of the isolation policies. MDR CHROMagar Acinetobacter may save time when the absence of a red color indicates the absence of MDR Acinetobacter spp. in a patient sample for screening and improving infection control strategies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.