
Abstract
Abstract
Background:
The number of chronic lower limb infections and their complications as venous and diabetic ulcers and chronic calf dermatitis is increasing worldwide. The clinical course and outcome in the immune responses to infection have been shown to be associated with genetic polymorphisms. The aim of study was to investigate frequencies of chosen single nucleotide polymorphisms (SNPs) in TNFα and TGFβ genes in patients with chronic lower limb infections and evaluate expression of messenger ribonucleic acid (mRNA) concentrations in chronic leg ulcers.
Methods:
Patients were divided into three groups: (group A) chronic venous leg ulcers, (group B) chronic post-traumatic non-healing wounds, and (group C) infected ischemic necrosis of the foot. Blood donors comprised the control group. Detection of polymorphisms was performed using polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) and gene expression by real-time PCR methods.
Results:
Patients in all groups showed higher frequency of TNFα gene polymorphism −308GG and lower frequency of −308GA genotypes than controls. The mutated homozygote AA was higher in groups A and B than in controls. The TGFβ74GG genotype was represented at highest values in group B. The GC genotype was found in all groups at a similar concentration lower than in controls. Genotypes TGFβ29TT and TC were represented at similar concentrations as controls. Analyses showed that the presence of the polymorphic allele −308A of TNFα gene was correlated with an increased concentration of gene expression in patients with chronic leg ulcers (group A). In the case of both TGFβ gene polymorphisms the presence of polymorphic allele C resulted in increased TGFβ gene expression.
Conclusions:
Comparison of genotypes in polymorphic sites in TNFα and TGFβ genes with their expression concentrations showed that the presence of polymorphic alleles could predispose to increased production of their proteins. Patients with prolonged non-healing wounds should have their genotypes studied, and in cases of mutation, long-term antibiotic and immune protein supply should be considered.
T
Polymorphism is the simultaneous occurrence of different allelic forms of a gene in the same locus. Mutations are responsible for the formation of new alleles or new genes in approximately 1% of the population [11]. Functional and association studies involving genetic polymorphisms of essential genes, including toll-like receptors, cytokines, and coagulation factors have provided important insights into the mechanisms involved in the pathogenesis of infection-induced organ dysfunction [3–5].
The development of molecular biologic techniques has led to the recognition of a series of polymorphic sites in different genes (e.g., single nucleotide polymorphisms [SNPs]) [12,13]. The advancement of high-throughput SNP genotyping provides valuable information on the interaction of multiple allelic variants and clinical outcome not only of sepsis but also local infective processes. Reports in the literature have shown the influence of the different allelic forms of a gene encoding a cytokine, both in its functional properties at the level of transcription [14] and susceptibility to certain diseases [15,16]. More precise categorization of patients based on genetic background might lead to individualized targeted treatment.
Our previous research on cytokine concentrations in various types of inflammation suggested that the polymorphisms of TNFα and TGFβ genes play a key role in soft tissues infections [17,18]. The purpose of the present study was to investigate frequencies of promoter's SNPs in TNFα (G-308A, rs1800629), TGFβ G74C (+915G>C, rs1800471, Arg25Pro), and TGFβ T29C (+869T>C, rs1800470, Leu10Pro) genes and evaluate the expression of messenger ribonucleic acid (mRNA) concentrations in chronic inflammatory changes in legs. Detection of mutations would be an indication for specific targeting of the inflammatory changes with antibiotics and supply of immune proteins.
Patients and Methods
One hundred forty-two patients, 18–91 years of age, with advanced inflammatory changes in the lower limbs were included in the study. They were admitted for treatment in the order in which they presented to the Department of Surgery of Central Clinical Hospital Ministry of Interior in Warsaw, Poland, during the period 2009–2013. Patients were divided into three groups: (group A) chronic venous leg ulcers (25 patients), (group B) chronic post-traumatic non-healing wounds (59 patients), and (group C) infected ischemic necrosis of a foot (58 patients). Exclusion criteria for all groups were rheumatic disease and steroid treatment. A control group of 129 blood donors, ethnically matched to the study group, was randomly selected for comparison of studied group data.
Blood samples were drawn from the antecubital vein and tissue biopsies from an ulcer edge. Bacterial flora of inflammatory changes was identified in biopsy specimens. The dominant strains were Staphylococcus aureus and Enterobacteriacae. The differentiation criteria were bacterial spectrum between the groups.
Ethics
The patients provided written consent and details of the protocol were explained fully. The study protocol was approved by the Medical University Ethics Committee and conforms to the ethical guidelines of the World Medical Association Declaration of Helsinki.
Study Design
Analysis of genetic polymorphisms of TNFα (G-308A) and TGFβ (G74C, T29C) using polymerase chain reaction-restriction fragment length polymorphism
Genomic deoxyribonucleic acid (DNA) was isolated from whole blood using the Blood Mini Kit (A&A Biotechnology, Gdynia, Poland) according to the manufacturer's instructions. Quantification of isolated DNA was performed spectrophotometrically using the NanoDrop ND-1000 spectrophotometer (Thermo Fisher Scientific Inc., Waltham, MA). Polymerase chain reaction (PCR) amplification was performed using a Thermal Cycler (MJ Research Watertown, MA). The amplification products were digested with appropriate restriction enzymes and separated and silver-stained on ultrathin 12.5% polyacrylamide gels (Multiphore II System and Silver Staining Kit, Amersham Pharmacia Biotech, Uppsala, Sweden).
Polymerase chain reaction-restriction fragment length polymorphism analysis of TNFα G-308A polymorphism
Polymerase chain reaction was performed using RedTaq polymerase (Sigma-Aldrich, St. Louis, MO). Approximately 50 ng of sample DNA was added to a final reaction volume of 25 mL containing 2.5 mL 10 × buffer with MgCl2, 0.5 mL deoxyribonucleoside triphosphate mix (Sigma-Aldrich) and 30 pmol of each primer (Genomed, Warsaw, Poland).
The primer sequences for TNFα (G-308A) gene were as follows: 5′ AGG CAA TAG GTT TTG AGG GCC AT 3′ (forward) and 5′ TCC TCC CTG CTC CGA TTC CG 3′ (reverse). The temperature profile of PCR was as follows: 95°C for 5 min, followed by 30 cycles of 94°C for 30 sec, 64°C for 30 sec, and 72°C for 45 sec followed by one elongation step at 72°C for 10 min. Polymerase chain reaction products (10 mL) were incubated for 2 h with 1 U NcoI (Roche Applied Science, Basel, Switzerland) in a total volume of 20 mL at 37°C.
Polymerase chain reaction-restriction fragment length polymorphism analysis of TGFβ G74C and T29C polymorphisms
Polymerase chain reactions were performed using FastStart™ Taq (Roche Applied Science). Approximately 50 ng of sample DNA was added to a final reaction volume of 25 mL containing 2.5 mL 10 × buffer with MgCl2, 0.5 mL deoxyribonucleoside triphosphate mix (Sigma-Aldrich), and 30 pmol of each primer (Genomed). The primer sequences for TGFβ (G74C) gene were as follows: 5′ CGC TGC TGT GGG TAC TGG T 3′ (forward) and 5′ CTC CGG TTC TGC ACT CTC C 3′ (reverse); the primers sequences for TGFβ (T29C) gene were as follows: 5′ ACC ACA CCA GCC CTG TTC GCG C 3′ (forward) and 5′ AGC CAC AGC AGC GGT AGC AGG A 3′ (reverse). Temperature profile of PCR of TGFβ (G74C) polymorphism was as follows: 95°C for 5 min, followed by 35 cycles of 95°C for 60 sec, 56°C for 60 sec, and 72°C for 60 sec followed by one elongation step at 72°C for 10 min. Polymerase chain reaction products (10 mL) were incubated for 2 h with 1 U FseI (New England Biolabs Ltd., Ipswich, MA) in a total volume of 20 mL at 37°C. The temperature profile of PCR of TGFβ (T29C) polymorphism was as follows: 95°C for 5 min, followed by 35 cycles of 95°C for 60 sec, 66°C for 60 sec, and 74°C for 60 sec followed by one elongation step at 72°C for 10 min. Polymerase chain reaction products (10 mL) were incubated for 2 h with 1 U BsrBI (Promega, Madison, WI) in a total volume of 20 mL at 37°C.
Analysis of TNFα and TGFβ genes expression at mRNA concentration (real-time PCR)
The total RNA was isolated from tissues taken from the ulcer edge (group A) and from normal skin (control group) using the Total RNA Mini Kit (A&A Biotechnology) according to the manufacturer's instructions. Isolated RNA was reversed to complementary deoxyribonucleic acid (cDNA) using VerteKIT (Novazym, Poznan, Poland) with oligo(dT)15 primers according to the manufacturer's instructions. The concentration of cDNA was analyzed by NanoDrop ND-1000 spectrophotometer (Thermo Fisher Scientific Inc.).
Real-time PCR was performed using a LightCycler 1.5 Instrument and LightCycler®FastStart DNA Master SYBR Green I detection kit (Roche Applied Science) per the manufacturer's protocol. The final 20 mL real-time PCR reaction included 500 ng RT product, 1 mL of each primer, 0.8 mL MgCl2, and 2 mL of LightCycler®FastStart DNA Master SYBR Green I. To reach a total volume of 20 mL per capillary, sterile water was added. The thermal cycling conditions were 95°C for 10 min, followed by 45 cycles at 95°C for 15 sec for denaturation, 61°C for 10 sec for annealing, and 72°C for 15 sec for extension. After 45 cycles, a melting curve was generated by slowly increasing (0.2°C/sec) the temperature from 70°C to 99°C while the fluorescence was measured. The primer sequences for TNFα gene were as follows: 5′-TGG CCA ATG GCG TGG AGC TG-3′ (forward) and 5′-CAG CCC CCT CTG GGG TCT CC-3′ (reverse); the primer sequences for TGFβ gene were: 5′-TTC GCC TTA GCG CCC ACT GC-3′ (forward), 5′-GTT GGT GTC CAG GGC TCG GC-3′ (reverse). As a reference, the expression of GAPDH gene was quantified for each sample using 5′-GTG AAG CAG GCG TCG GAG GG-3′ (forward) and 5′-GCT CTT GCT GGG GCT GGT GG-3′ (reverse) primer set. The reactions for TNFα, TGFβ, and GAPDH were carried out in separate tubes. The control was performed using cDNA from healthy volunteers instead of cDNA from patients.
The results were analyzed by a calculation formula: folds = 2-ΔΔCt, for TNFα: ΔΔCt = [Ct TNFα – Ct GAPDH]experiment sample – [Ct TNFα − Ct GAPDH]control sample [19]. According to this formula ΔΔCt for the control group was 0 and TNFα gene expression in this group was equal to 1. In an analogous way, the conversion for TGFβ gene was performed. The results of TNFα and TGFβ gene expression for patients with chronic leg ulcers (group A) were expressed as mean ± standard deviation (SD).
Statistical analysis
Statistical analysis was performed using the StatSoft Statistica version 10.0 program (StatSoft Inc., Tulsa, OK). Differences at p < 0.05 were considered to be statistically significant. Comparison of allele and genotype frequencies for each polymorphism was analyzed by Fisher exact test. In the case of expression study, the normality of distribution of analyzed parameters was verified with the Shapiro-Wilk test. To evaluate the statistical significance in TNFα and TGFβ gene expression between patients with chronic leg ulcers and healthy volunteers, as well as the two genotypes, the Mann-Whitney test was used. Additionally, the Kruskal-Wallis test was used to compare the gene expression of three genotypes.
Results
TNFα G-308A, TGFβ G74C, and T29C polymorphism analysis
The obtained data are presented in Figures 1–3. There were differences in genotypes of TNFα G-308A of patients and control subjects.
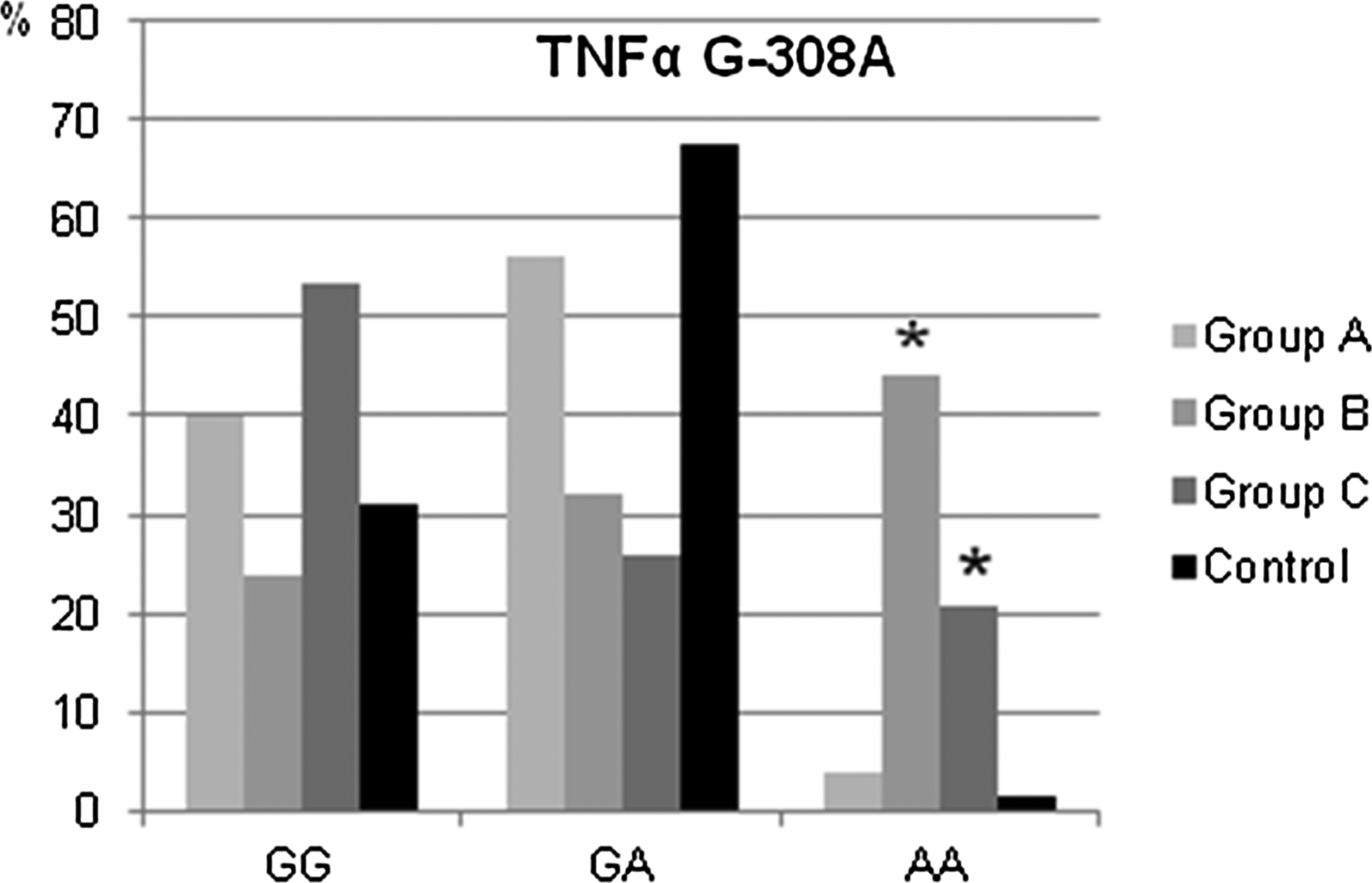
Percentage of genotypes of TNFα G-308A polymorphism in subgroups (A–C) compared with controls, *p < 0.0001.
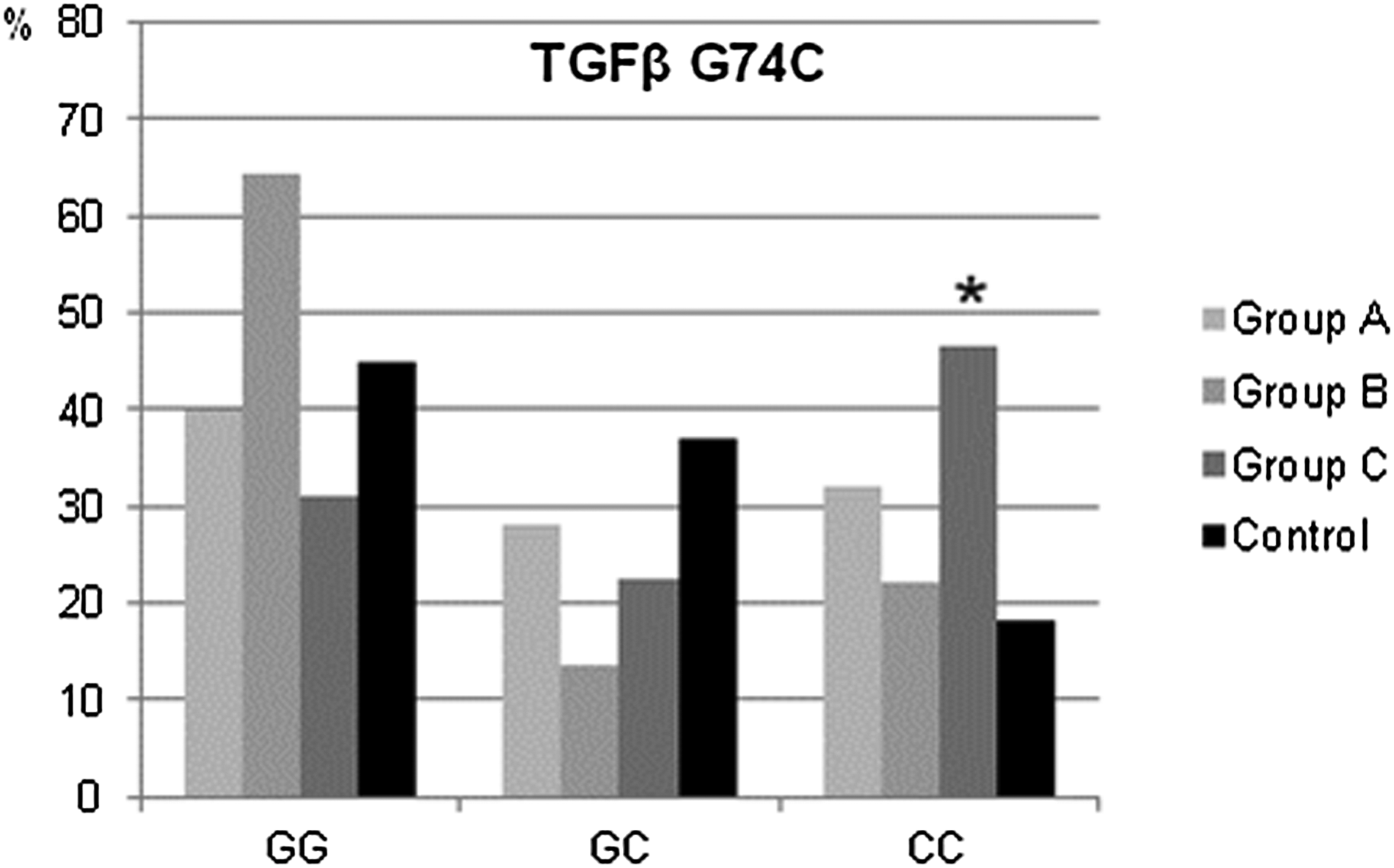
Percentage of genotypes of TGFβ G74C polymorphism in subgroups (A–C) compared with controls, *p = 0.0001.
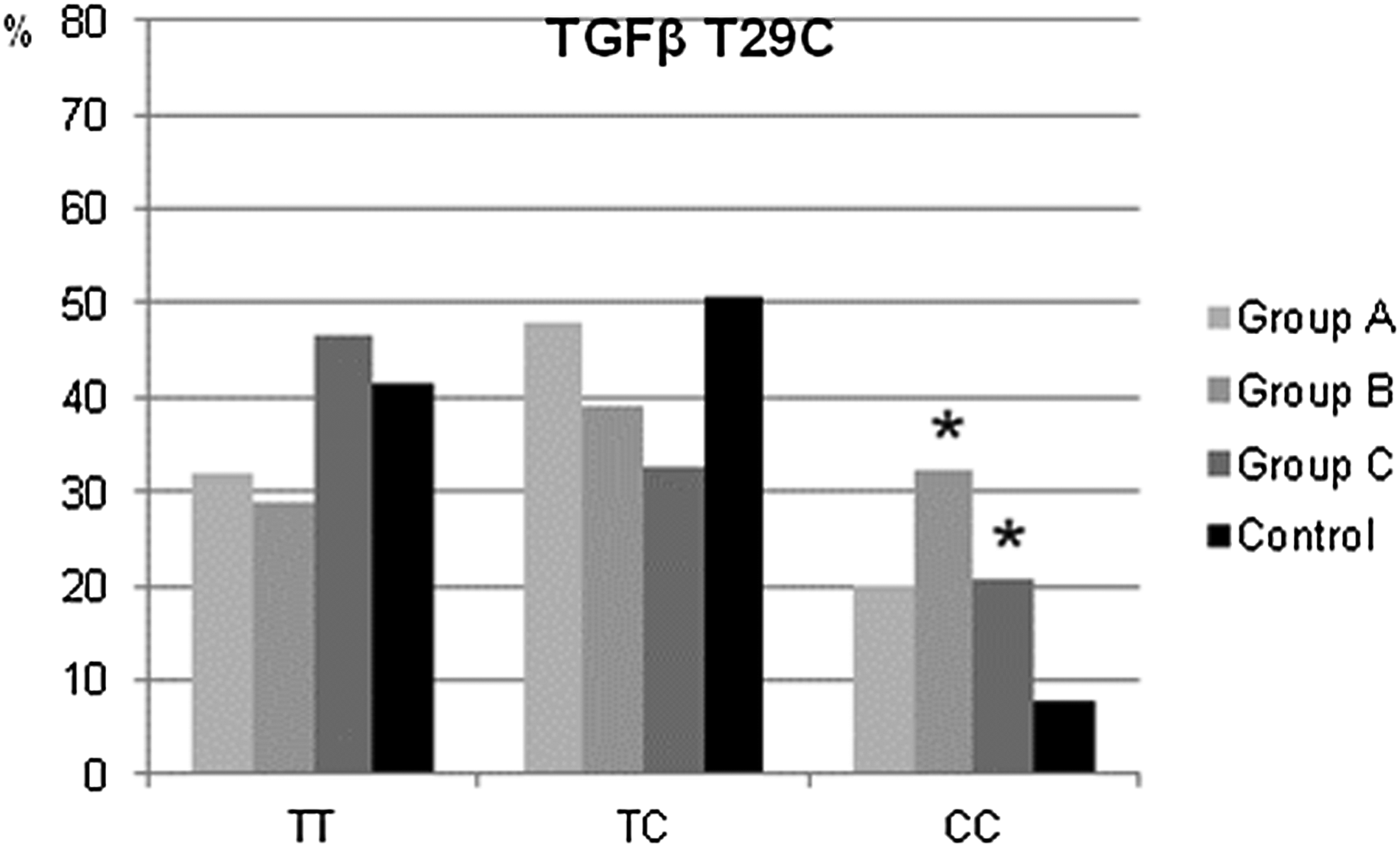
Percentage of genotypes of TGFβ T29C polymorphism in subgroups (A–C) compared with controls *p < 0.0001 (group B), p = 0,0249 (group C).
Patients in subgroups (group A and C) showed a higher frequency of TNFα gene G-308A polymorphism GG and lower GA genotypes in all study groups than in controls. The mutated homozygote AA was higher in chronic non-healing wounds (group B) and infected ischemic necrosis of a foot (group C) than in controls (p < 0.0001) (Fig. 1). TGFβ 74 GG genotype was represented at highest values in patients with chronic non-healing wounds (group B). The GC genotype was found in all groups at a similar concentration that was lower than in controls. No significant differences were found at TGFβ 74 CC genotype in groups (group A and B) of both patients and controls. Patients with infected ischemic necrosis of a foot (group C) showed a higher frequency of CC genotype (46.6%) than controls (18.1%; p = 0.0001) (Fig. 2).
TGFβ 29 TT genotype was represented in 28.8%–46.6% in all three groups and TC genotype in 32.7%–48.0% at a concentration similar to controls (41.4% and 50.8%, respectively). There were more TGFβ mutated homozygote CC patients in all three groups (20.0% [NS]), 32.2% (p < 0.0001), 20.7% (p = 0.0249) than in healthy subjects (7.8%) (Fig. 3).
Genotypes of TNFα and TGFβ and their relative expression in patients with chronic venous leg ulcers (group A)
The second part of the study compared the expression concentration of TNFα and TGFβ genes in patients with chronic leg ulcers (group A). The results obtained as a mean of gene expression relative to the internal control glyceraldehyde phosphate dehydrogenase (GAPDH) is shown in Figures 4 and 5.
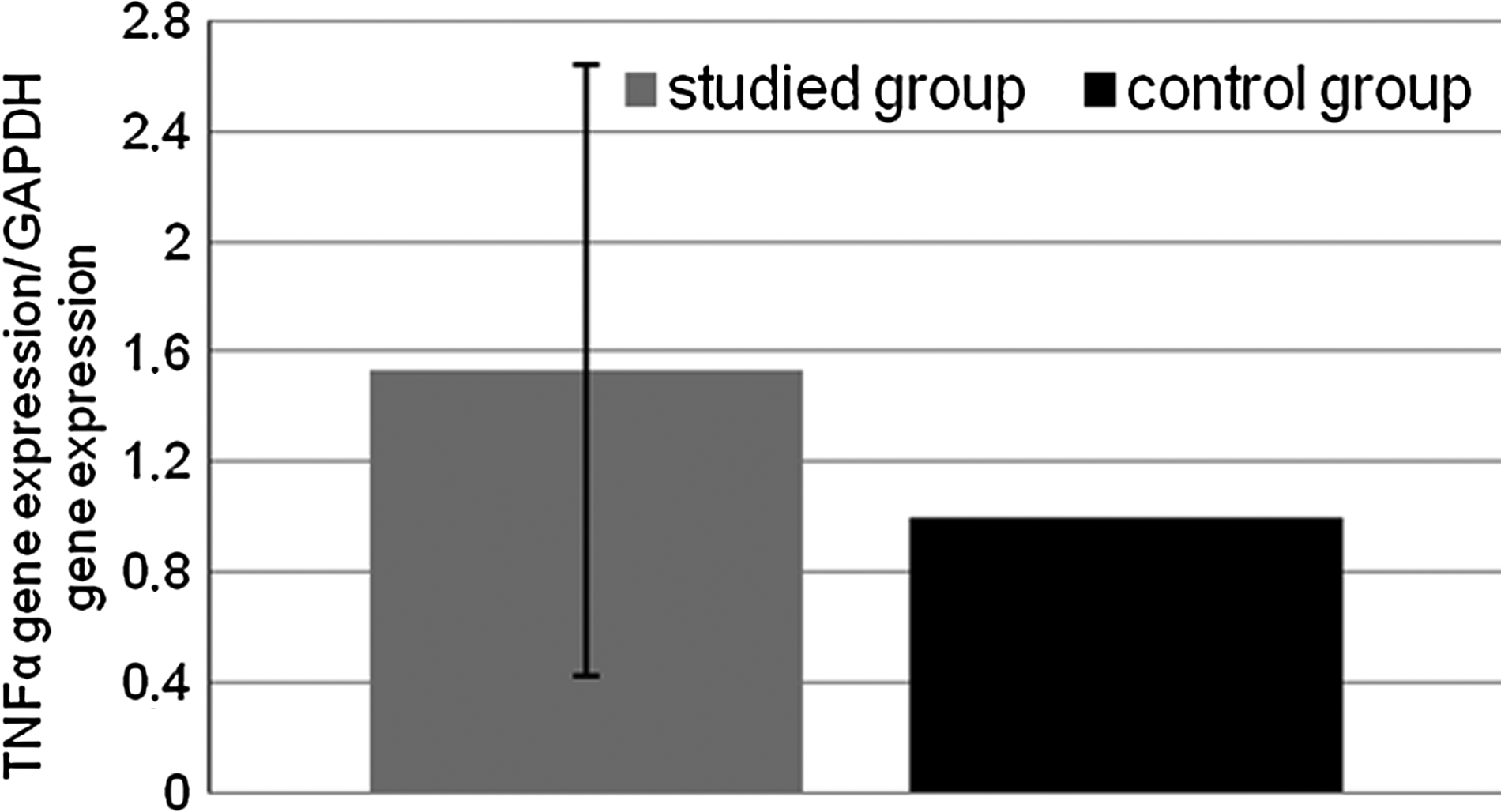
TNFα gene expression in tissues of patients with chronic venous leg ulcers.
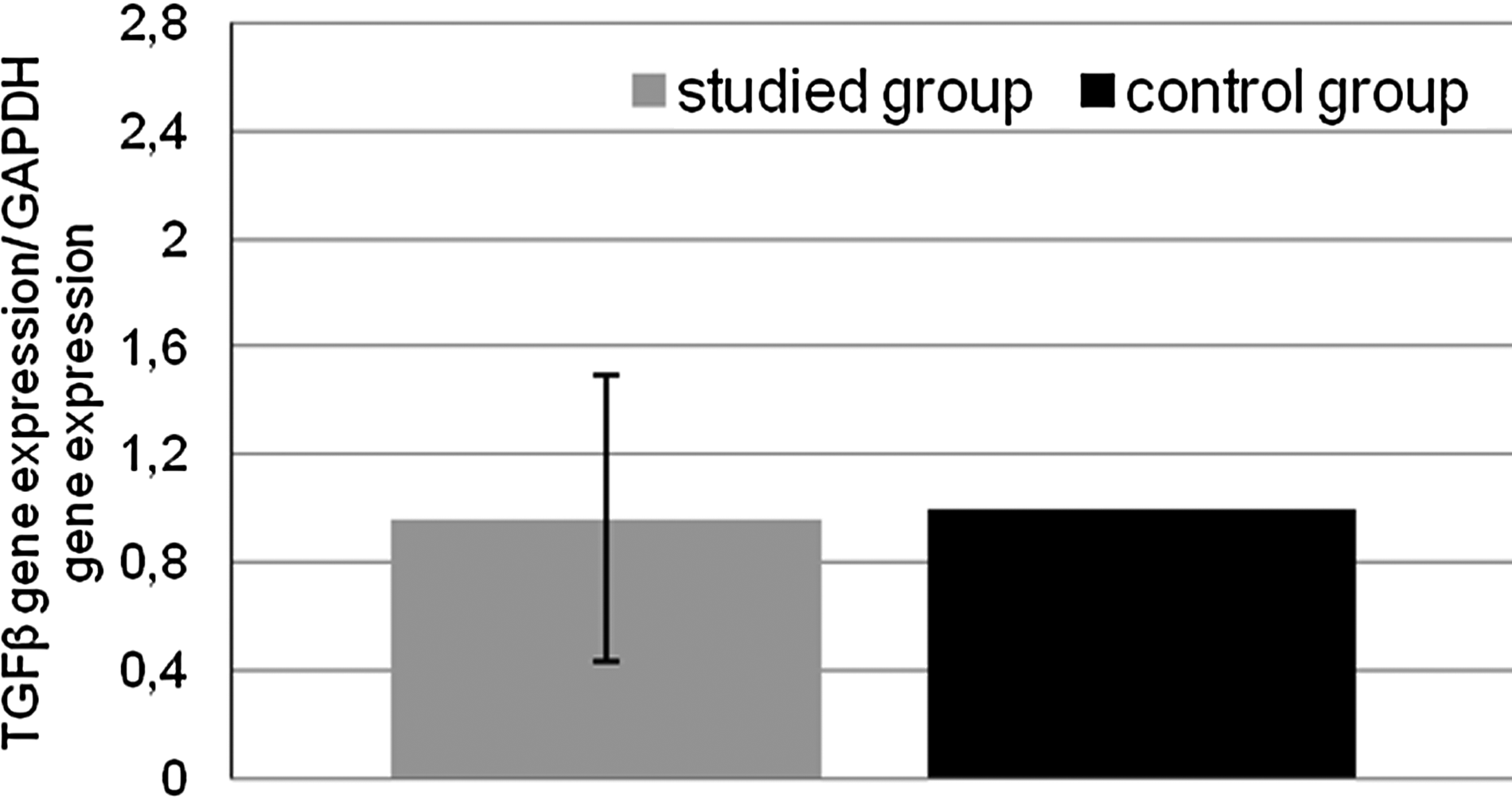
TGFβ gene expression in tissues of patients with chronic venous leg ulcers.
There was no difference between the level of expression of the TGFβ gene in patients with chronic leg ulcers and the reference group. The results of the study showed higher relative expression of the TNFα gene in studied groups compared with healthy volunteers but differences were not statistically significant (p = 0.3879).
The impact of the three polymorphisms of TNFα and TGFβ genes on the relative expression of these genes illustrate Figures 6–8. Analyzes showed that the presence of the polymorphic allele −308A of TNFα gene was correlated with an increased level of gene expression in patients with chronic leg ulcers (group A). In the case of both TGFβ gene missense polymorphisms T29C and G74C, we also observed that the presence of a polymorphic allele C resulted in increased TGFβ gene expression. Comparing the average level of gene expression between the three genotypes showed no statistically significant difference. The obtained results are as follows: G-308A polymorphism TNFα gene (p = 0.6155), T29C and G74C TGFβ gene (p = 0.5987 and p = 0.0787, respectively). However, comparison of the mean of expression between genotypes 74GG and 74GC of TGFβ gene found a statistically significant difference (p = 0.0359).
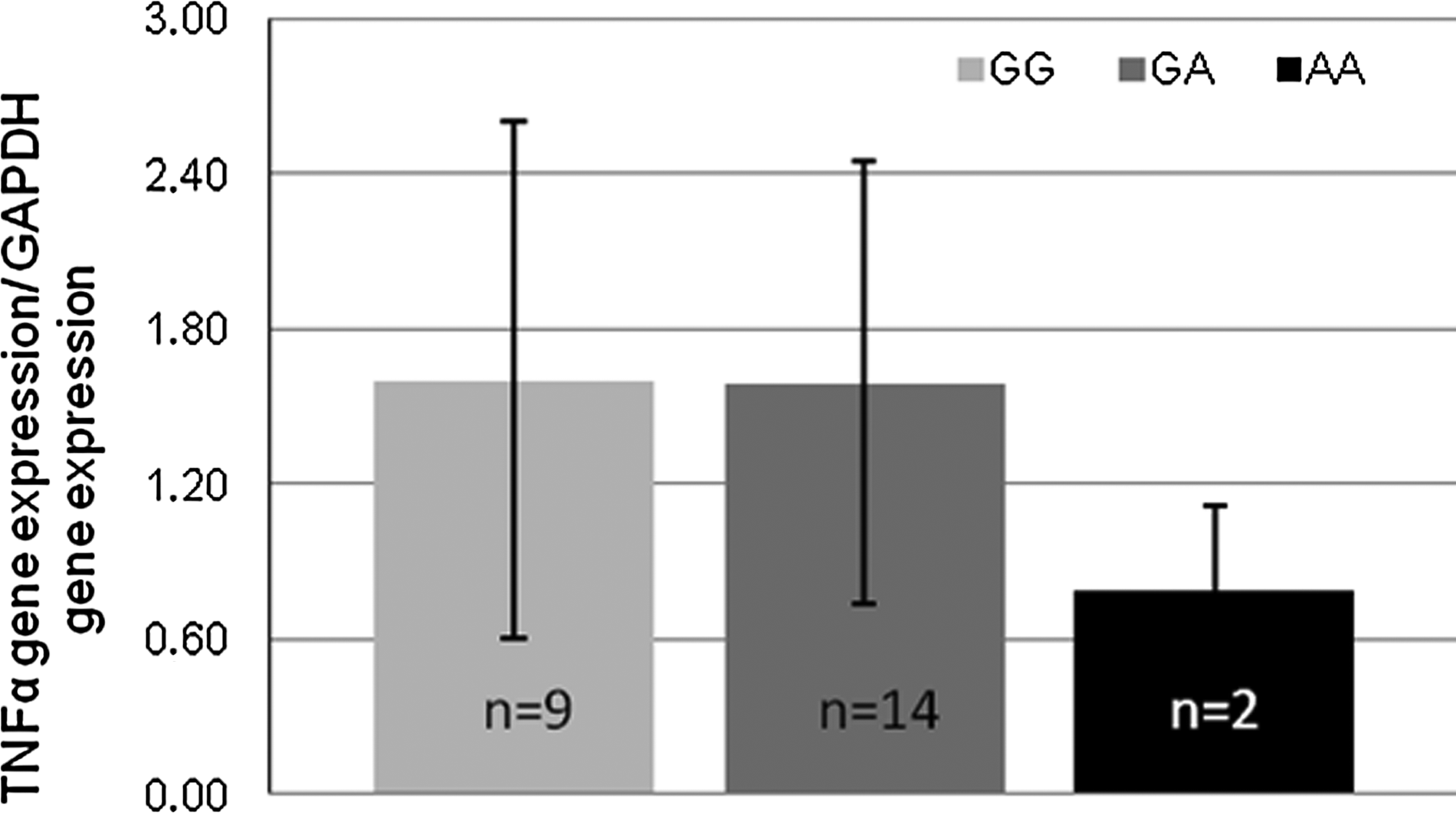
TNFα mRNA expression in relation to G-308A polymorphism.

TGFβ mRNA expression in relation to T29C polymorphism.

TGFβ mRNA expression in relation to G74C polymorphism.
Discussion
This study provided the following information: comparison of genotypes in G-308A and T29C and G74C polymorphic sites in the TNFα and TGFβ genes with their expression levels showed that the presence of polymorphic alleles could predispose to increased production of their proteins. A special role in the development of inflammatory mechanisms is played by cascade of pro- and anti-inflammatory cytokines. Single nucleotide polymorphisms in regulatory regions of cytokine genes have been associated with susceptibility to a number of complex disorders [20]. Variation in the TNFα gene promoter region have been found to be associated with susceptibility to several diseases including sepsis [18,21], rheumatic fever [22], and venous leg ulcers [23,24]. The relation of disease susceptibility of different genotypes of TNFα gene are important both at the position −308 SNP and the microsatellite polymorphism [25,26]. In rheumatoid arthritis, the relation between the polymorphism of the gene encoding TNFα −308 position and susceptibility to the disease was demonstrated [27,28]. Additionally, TNFα polymorphism has been demonstrated to effect the occurrence of multiple sclerosis [29] and insulin-dependent diabetes mellitus [30].
Tumor necrosis factor-α is a potent pleiotropic, pro-inflammatory cytokine that belongs to the TNF superfamily. Tumor necrosis factor-α mediates a number of biologic processes, including lipid metabolism, coagulation, insulin resistance, endothelial functions, and wound healing [31]. Moreover, it plays a crucial role in the inflammation phase of normal wound healing and also in the healing of pathologic wounds such as venous leg ulcers. Wallace and Stacey [32] found that the concentration of TNFα is downregulated in wound fluid from non-healing venous leg ulcers compared with healing ones. Wallace et al. [23] reported previously that the −308 A/G SNP of the promoter region of the TNFα gene is a predisposing factor for venous leg ulcer development. Nagy et al. [24] observed that the association between −308 TNFα SNP and venous leg ulcer susceptibility might depend on the body mass index of the Hungarian individuals enrolled in the study.
In patients with chronic lower limb infections, the expression of TNFα and TGFβ genes in tissues and correlation with the polymorphisms of these genes has not been investigated. In our previous study, we demonstrated that the polymorphisms of both TNFα and TGFβ genes may be responsible for the predilection to inflammatory processes manifested by sepsis and acute local tissue infections. We found a high percentage of TNFα −308 GG genotype in all patients but TNFα protein remained at a concentration similar to control levels. The highest values of TNFα were observed in −308 GA genotype for sepsis and acute rather than chronic infections groups [18].
Both cytokines are expressed during the wound healing process, however, their effect is antagonistic. TGFβ is known as a pro-fibrotic protein initiating the response of extracellular matrix components [33,34]. Previous analysis of animal models proved that deficiency of TGFβ1 protein impairs wound repair because of collagen deposition, etc. On the other hand, TNFα, an anti-fibrotic protein, could suppress the expression of the extracorporeal membrane (ECM) genes as well as TGFβ and its further pro-healing activity [33] by interfering with the TGFβ signaling pathway [35]. It is clear that the balance between both cytokines is crucial for proper healing processes [35].
Current research related to TNFα G-308A polymorphism showed a higher frequency of GG and lower GA genotypes in patients with chronic leg ulcers and infected ischemic necrosis of the foot than in controls (p < 0.0001). We also found higher relative expression of TNFα gene in patients with chronic leg ulcers compared with healthy volunteers but these differences were not statistically significant. We also observed a higher relative TNFα mRNA expression in homozygote wild-type GG and heterozygote GA genotypes compared with homozygote mutant AA genotype in patients with chronic leg ulcers. Therefore, we suggest that the A allele is associated with a higher TNFα mRNA expression compared with the G allele of TNFα −308 polymorphism. Others studies indicate the rare −308A allele of TNFα gene is often suggested to be associated with enhanced TNFα protein production [36,37] and with higher risk of severe sepsis [38]. Additionally, the presence of increased expression in patients (group A) with genotype AA could have influence on lower healing activity because of collagen formation.
Transforming growth factor-β1 is a multi-functional cytokine that plays a key role in the regulation of cellular proliferation and differentiation, embryonic development, wound healing, and angiogenesis [39]. Transforming growth factor-β suppresses the immune system and induces the generation of extracellular matrix components, thus playing an essential role in wound healing and tissue repair. Transforming growth factor-β is fundamental to wound healing, however, overproduction of TGF-β can result in excessive deposition of scar tissue and fibrosis [40]. The published results indicate that polymorphisms within the TGFβ1 gene may have a role in determining the development or severity of various diseases such as rheumatoid arthritis [41] and idiopathic pulmonary fibrosis [42].
The results obtained by Mattey et al. [41] indicate that patients with rheumatoid arthritis carrying a T allele of the T869C polymorphism may have increased inflammatory activity over the long term. The poor outcome and earlier mortality in these patients possibly can be explained by reduced production of TGFβ1, leading to impaired control of inflammation [41]. Son et al. [42] also showed that 869 TT genotype of TGFβ1 gene may affect the susceptibility and disease severity of idiopathic pulmonary fibrosis in Koreans. Inherent production of a high concentration of TGF-β1 was associated with severe lung fibrosis and rapid deterioration in lung function [43,44].
To date, less attention has been paid to the study of TGFβ gene polymorphisms in patients with chronic lower limb infections. We have shown previously that concentrations of TGFβ protein was higher for CC genotype for patients with sepsis and acute infections than chronic infected wounds [18]. In a studied group of patients, including a large number of gastric, pancreatic, and colon cancer cases, we found that the TGFβ CC mutated homozygote genotype was represented only in patients but not in control patients [18].
Our study found no significant differences in TGFβ 74CC genotype in patients with chronic leg ulcers, chronic non-healing wounds, and controls. Patients with infected ischemic necrosis of a foot showed a higher frequency of CC genotype in this polymorphic site than control patients (p = 0.0001). There was no significant difference between the level of expression of the TGFβ gene in patients with chronic leg ulcers and a reference group. In the case of both polymorphisms T29C and G74C, we also observed that the presence of a polymorphic allele C resulted in increased TGFβ gene expression. The comparison of the mean of expression between genotypes GG and GC polymorphism G74C TGFβ gene found a statistically significant difference.
As a result, substitution G to C in TGFβ G74C changes the amino acid sequence in codon 25 from polar and basic arginine to non-polar and neutral proline. Such changes may affect the functions and conformation of protein. Taking this into consideration, this polymorphism is defined as benign variant clinically relevant. In TGFβ T29C substitution results in a change from leucine to proline. Both amino acids are non-polar and neutral. Noticeable change in amino acid sequence is this from exogenic leucine to endogenic proline. This polymorphic variant belongs to other variants in clinically relevant classification.
Polymorphisms in the promoter region of gene TNFα and TGFβ seem to correlate with the level of expression of these genes in patients with lower leg ulcers. In order to substantiate the results, we propose increasing the number of patients in the study group. It would also be of interest to trace the binding sites of the transcription apparatus and analysis of the results obtained in this aspect.
In conclusion, this study suggests that the TNFα and TGFβ gene polymorphisms predispose to a development of chronic lower limb infections in the Polish population. Patients with long-term non-healing limb wounds should undergo genetic polymorphism testing of genes for pro- and anti-inflammatory cytokines. The results may be important for evaluation of prognosis of healing. Determined by a routine blood test, the presence of a polymorphisms could help in optimizing wound healing treatment. Moreover, detection of mutations may be an indication for targeted long-term antibiotic therapy depending on the type of flora and simultaneous supply of gamma-globulins.
Footnotes
Acknowledgments
This work was supported by project number NN 404 077136, founded by Ministry of Science and Higher Education.
Author Disclosure Statement
The authors declare no conflict of interest.