
Abstract
Abstract
Background:
Silicone embolization syndrome, a serious adverse effect of illicit silicone injections by laypersons, occurs when silicone particles enter the circulation and shower the lungs and other vital organs.
Methods:
We review the literature on silicone embolization syndrome and describe a unique case of the syndrome that developed after a latent period of several months, upon surgical debridement of an injection site abscess.
Results:
In the scientific literature, silicone embolization syndrome has been well described and multiple presentations have been delineated. Immediate presentation with a rapidly fatal course occurs in cases of erroneous intra-vascular injection, in which large volumes of silicone occlude pulmonary arteries and cause cor pulmonale. Insidious presentation of progressive respiratory distress and systemic inflammatory response syndrome occurs in cases of peri-vascular injection, caused by gradual vascular infiltration by smaller silicone emboli that shower pulmonary capillaries diffusely, causing alveolar hemorrhage and inflammation. Rarely, latent cases have presented months to years later upon trauma to the original site, which disrupts the sequestered siliconoma, allowing re-exposure to the immune system and the opportunity for vascular infiltration.
Conclusions:
To the best of our knowledge, this is the first description of silicone embolization syndrome that occurred after surgical manipulation of the site. It has important management implications for patients with a history of prior silicone injections at a site being considered for surgical intervention. Strategies for managing this potential complication include adding a regimen of daily debridement, aggressive ventilator support, and maintaining close observation in an intensive care unit (ICU) or progressive care unit (PCU) during the high-risk post-operative period. Alternatively, when possible, surgeons may avoid disruption of the siliconoma by trialing medical management of localized inflammation or using alternative procedures such as image-guided wide local excision or liposuction with fat transfer.
T
Case Report
A 47-year-old female Jehovah's Witness presented to the hospital with a 3-d history of sharp, intermittent epigastric pain associated with nausea, vomiting, diarrhea, fever and chills, weakness, and headache. She also complained of pain and swelling over her buttocks for several weeks. She had a history of subcutaneous silicone injections into the buttocks 5 mo prior, by a non-licensed person who brought the material to the patient's home; and a subsequent incision and drainage (I&D) of an associated gluteal abscess at another hospital, 1 mo prior to this presentation. From that admission, a magnetic resonance image (MRI) demonstrated multiple pockets of foreign body material deposits and associated edema throughout the subcutaneous tissue bilaterally along the medial gluteal folds and in the left gluteus maximus muscle with associated myositis (Fig. 1). Cultures at that time showed no micro-organism growth. The patient had been discharged on linezolid, but was switched to trimethoprim-sulfamethoxazole because of complaints of stomach upset.
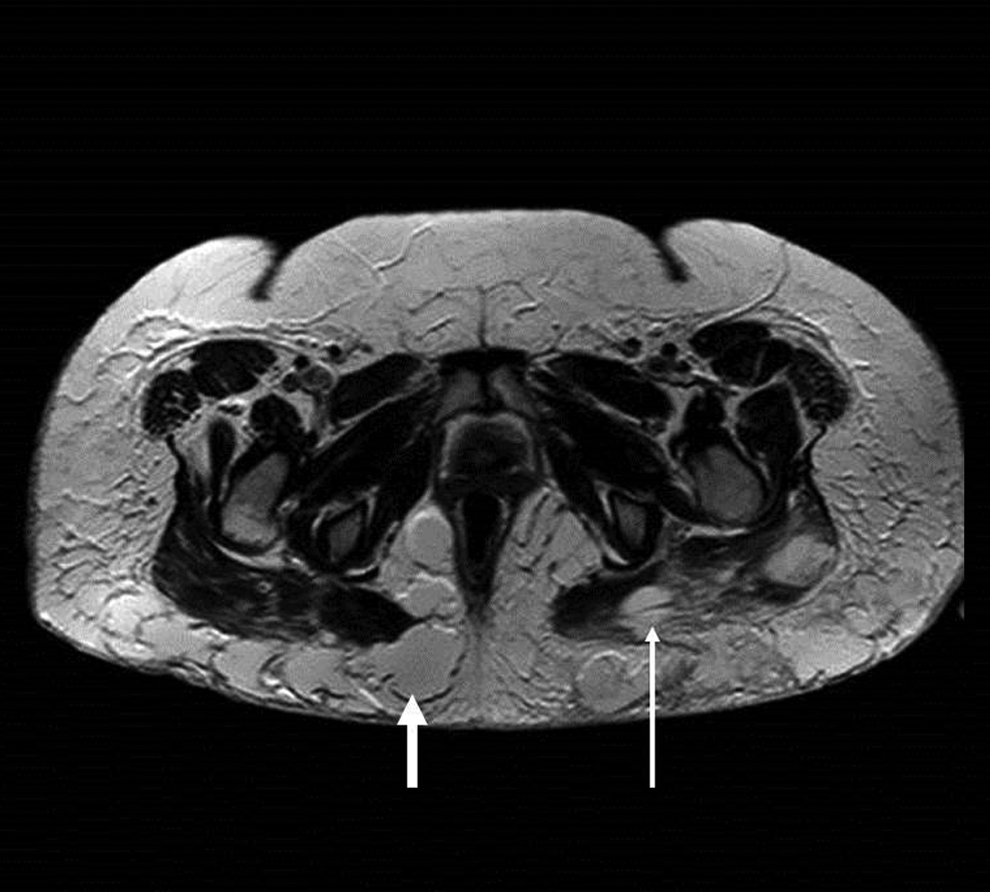
Magnetic resonance imaging of the pelvis demonstrating pockets of foreign body deposits and associated edema throughout subcutaneous tissue of buttocks bilaterally (short, thick arrow) and within left gluteus maximus muscle with associated myositis (long, fine arrow).
On the current presentation, physical findings included mild distress, axillary temperature of 100.9°F, heart rate of 117 beats/min with otherwise normal vital signs, a petechial rash over the legs and chest (Fig. 2), and tender, erythematous indurated areas on the buttocks, measuring up to 10 cm×6 cm on the right and 7 cm×5 cm on the left. Laboratory results were notable for [Na+] 130, [Cl-] 92, serum creatinine 1.15. C-reactive protein was 108.5 mg/L and [hemoglobin] (Hb) was 11.2 g/dL. She was admitted on broad-spectrum antibiotics and supportive care, with a plan for I&D the following morning. She declined consent to peri-operative blood products because of her religious affiliation. On hospital day two, an ultrasound-guided I&D of the buttocks was performed. Copious amounts of silicone beads, turbid pus, and serous fluid were drained. Spectrographic analysis revealed the material to be medical-grade polymethylsiloxane. The area was irrigated, Penrose drains were placed, and the wounds were packed with gauze. Cultures from this procedure demonstrated no growth.

Clinical photographs demonstrating petechial rash over the patient's legs and chest at the time of admission.
The post-operative course was complicated by wound bleeding and severe anemia (Hb 5 g/dL) on day four, for which the patient declined blood products and was initiated on iron supplementation and Epogen® (Amgen, Thousand Oaks, CA). On the morning of hospital day five, she was found profoundly anemic (Hb of 4.5 g/dL), hypotensive at 72/47 mmHg, febrile at 103.8°F, tachycardic at 140 beats/min, with altered mental status. She was admitted to the intensive care unit (ICU), where she was volume resuscitated and placed on multiple vasopressors. When her mental status improved, and in the presence of family, she consented to a blood transfusion and received 3 units of red blood cells concentrates. The buttocks remained erythematous and indurated, therefore, another I&D was performed at the bedside and the patient was started on a regimen of daily dressing changes and bedside debridements.
On hospital day six, the patient developed progressive respiratory distress with severe hypoxemia and was intubated. Chest radiographs demonstrated bilateral infiltrates and a clinical picture consistent with acute respiratory distress syndrome (ARDS; Fig. 3). She remained intubated in the ICU for nine days. Soft tissue cultures eventually grew Candida tropicalis. She would complete a 28-d course of doxycycline and ciprofloxacin and a 60-d course of fluconazole. With gradual improvement on these regimens, she was eventually weaned off vasopressors, extubated, and discharged in stable condition with home wound care, after a 21-d hospitalization.
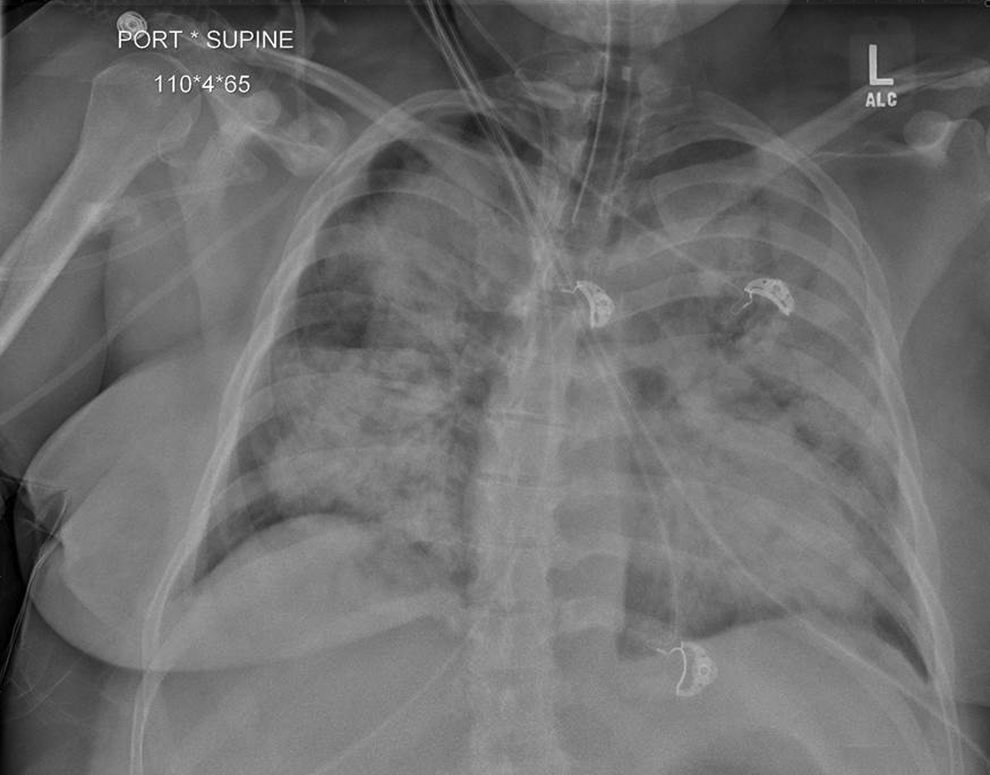
Portable chest radiograph demonstrating bilateral dense interstitial infiltrates which indicate the development of acute respiratory distress syndrome.
Literature Review and Discussion
Medical-grade silicone (polydimethylsiloxane) has a history of utilization in the medical field for a variety of purposes, including joint and heart valve implants, intra-ocular procedures, and cosmetic and reconstructive procedures. Its popularity and versatility for medical use are the result of its favorable properties as a relatively inert material with high temperature stability. In addition, it has not been believed to undergo biochemical transformation or initiate inflammatory reactions [1]. However, when silicone is introduced into subcutaneous tissue, a granulomatous inflammatory response and foreign body giant cell reactions are activated, forming walled-off pockets of material called siliconomas [2]. Furthermore, recent studies have suggested that silicone is not as stable biochemically as once believed; it may be oxidized to silica, after which it may be incorporated into the reticuloendothelial system [3]. The illicit misuse of silicone by laypersons has been associated with serious adverse effects, attributed to large injection volumes, non-sterile techniques, lack of medical training by those administering the injections, and in some cases, impurity of the material injected, including use of industrial-grade silicone with a variety of filler materials [1]. These adverse effects include what is known as silicone embolization syndrome.
Proof of silicone embolization dates back to 1967, when silicone administered to mice via local subcutaneous injections was later found deposited in the spleen, liver, adrenal glands, and kidneys [4]. On the basis of this study, it was hypothesized that the mechanism likely involved circulating phagocytes that ingested the material from its local source [5]. The phenomenon was evidenced clinically in 1975, when a female patient experienced rapid cardiopulmonary and neurologic decline, and died within hours of a breast silicone injection that had been injected mistakenly intra-vascularly. At autopsy the patient was found to have spectrography-confirmed silicone vacuoles showering the lungs, liver, kidneys, and brain. At that time, the cause of death was described as acute bilateral pulmonary edema [6]. Over the next decade, multiple cases were described in which patients developed acute pneumonitis after subcutaneous silicone injections. Bronchoalveolar lavage (BAL) in these cases demonstrated silicone inclusions within alveolar macrophages and in alveolar supernatant fluid, and increased numbers of alveolar inflammatory cells. Most patients presented within hours of the injections with fever, hypoxemia, and bilateral pulmonary infiltrates. However, one patient presented years after the injection, upon sustaining blunt trauma to the prior injection site. His presentation involved a lesser degree of the described pulmonary findings, plus local inflammation at the site [7,8]. This was the first description of a latent presentation, in which a previously sequestered and latent collection of silicone was mobilized by trauma to the area, gaining exposure to both circulation and inflammatory cells.
By the early 2000s, it was well known that illicitly injected silicone had the potential to embolize to the pulmonary vessels and cause respiratory failure. However, varying degrees of severity began to be delineated, beginning with five patients who had received illicit silicone injection into the vaginal wall. Two cases were rapidly progressive and fatal within 10 h of injection, while the other patients had more insidious courses of up to 31 d. Upon autopsy of the rapidly progressive cases, large pulmonary vessel branches demonstrated acute cor pulmonale and massive silicone emboli filling the lumen, but minimal pathologic findings in the alveolar tissue. Upon autopsy of the insidious cases, pathology demonstrated impressive alveolar infiltration, inflammation, and injury, as well as previously described findings of silicone deposits within the alveolar spaces, walls, and macrophages. The authors proposed two different pathophysiologic mechanisms to describe these two different presentations. In the rapidly fatal cases, erroneous intra-venous injection of a large volume of silicone had caused near-total occlusion of pulmonary vessels, with rapid cardiopulmonary decline and death before a significant inflammatory response could occur. In the insidious cases, peri-vascular injections had allowed the material to infiltrate nearby vessels, disseminating more gradually and yielding smaller emboli to pulmonary capillaries. Subsequently, these emboli activated inflammatory cascades, causing extrusion and hemorrhage into the parenchyma, and alveolar infiltration and inflammation [9]. At this time it was also theorized that even individuals who did not develop either type of acute complication could still experience a depot-like effect from subcutaneous silicone pockets, which may allow smaller amounts of material to enter circulation over longer periods of time [9]. In these cases, manipulation of the local site could predicate or exacerbate an influx of previously sequestered silicone into circulation, allowing varying degrees of dissemination and embolization depending on the volume mobilized.
In 2005, it was proposed that cell-mediated immune reactions to the material may be an additional pathophysiologic factor [10]. If this were true, these patients' presentations may be caused not only by dissemination and embolism, but also include a component of massive immune response after initial immune sensitization at the time of injection, a latent interval of granulomatous sequestration, and re-exposure to systemic circulation upon disruption of the siliconoma. This could help explain why a patient such as ours may enter a state mimicking overwhelming sepsis, despite multiple negative blood and soft tissue cultures. Therefore, when our patient initially presented with abdominal pain, a petechial rash, and symptoms of systemic inflammatory response that had progressed over 1 mo since her first I&D, we now believe that she was experiencing complications of gradual silicone dissemination from the local site that had been manipulated. When further manipulation mobilized additional material, her presentation became much more acute.
By the mid-2000s, most cases of silicone embolization syndrome had a high rate of full recovery as a result of advanced critical care techniques, yielding more information from patients who survived. A common pathophysiologic pathway with fat embolization syndrome (FES) was proposed initially in 2005 by Pastor et al. [10] based on similar pathologic findings. Later that year, a case review of 11 articles compared 32 patients hospitalized after illegal silicone injections. Six patients experienced neurologic changes during or immediately after the injections and all had a rapidly fatal course, likely a result of direct intra-vascular injection. The remaining patients presented with respiratory distress, and had a 93% rate of discharge home within 3 wks despite a critical presentation and unstable course. All patients had diffuse bilateral patchy infiltrates on chest radiography, with BAL or lung pathology demonstrating silicone globules infiltrating alveolar spaces, macrophages, walls, and pulmonary capillaries, as well as neutrophil-predominant inflammation. Alveolar hemorrhage was present in 21 of the patients. Pulmonary ventilation perfusion (
In summary, these cases have proposed a variety of mechanisms by which illicitly injected silicone may gain access to the circulation: presenting immediately, after direct intra-vascular injection; presenting insidiously because of vascular infiltration and phagocytic migration from peri-vascular deposits; and presenting latently, upon trauma or manipulation of sequestered subcutaneous and soft tissue collections. Our patient presented with symptoms of systemic inflammatory response and a petechial rash 1 mo after surgical debridement of high-volume gluteal silicone collections. Upon subsequent surgical debridement, she experienced multiple organ dysfunction syndrome with ARDS. This is consistent with the literature yet unique in that it occurred in conjunction with a necessary surgical debridement of the local site, and therefore, presents a unique management dilemma of which surgeons should be aware.
The implications of this case necessitate that physicians be vigilant for the development of respiratory failure and systemic inflammatory response syndrome in patients who require manipulation of prior silicone deposits, particularly if the injections were of large volume or obtained illicitly. Tactics for managing this complication in the future may include adding daily debridements to remove residual foreign body material before it enters the circulation, and maintaining close observation in the ICU until the patient stabilizes. For patients with large collections or who are already experiencing systemic and respiratory symptoms, surgeons may opt to perform an image-guided wide local excision of the area, in order to avoid mobilizing sequestered foreign material. In these instances, wide excision may be the best chance of a curative treatment but will unfortunately leave patients with substantial cosmetic deformity. Salgado et al. [12] recommends another surgical option, namely ultrasound-guided liposuction with intra-muscular fat transfer, which demonstrated good cosmetic results and reasonable removal of silicone deposits. Regardless of the approach, ongoing management may be required, using imaging studies such as computed tomography, MRI, and radiolabeling to identify areas of continued inflammation.
Thus far, an array of medical options have been attempted, including systemic corticosteroids and antibiotics, which have mostly yielded little improvement and variable results [1]. A regimen of minocycline or tetracycline plus celecoxib has been described for two patients with latent presentation and mostly local symptoms, and garnered improvement where the antibiotics alone did not [1,13]. Although additional studies will be required to demonstrate the effectiveness of this regimen, this may be an appropriate option for patients with local symptoms, in light of the risks of precipitating a latent silicone embolism syndrome with surgical manipulation of the site.
Conclusions
Silicone embolization syndrome, although rare, has been well described by multiple case reports and reviews over the past several decades. As described in this unique case, patients may develop the syndrome after surgical debridement of previously sequestered local silicone collections. Therefore, surgeons should be aware of this possibility and vigilant for its development when they encounter a patient requiring I&D of a prior silicone injection site. Strategies for managing this complication in the future include adding daily debridements, maintaining close observation peri-operatively, or opting to perform alternate procedures such as an image-guided wide local excision or liposuction with fat transfer.
Footnotes
Acknowledgments
Author Disclosure Statement
No competing interests exist, financial or otherwise.