
Abstract
Abstract
Background:
Emergency operations performed on an obstructed colon are accompanied by an increased risk of anastomotic insufficiency. Tissue-destructive matrix metalloproteinase (MMP) activity is elevated in the obstructed colon and contributes to a loss of suture-holding submucosal collagen, which may be mediated by tumor necrosis factor (TNF)-α. Our aim was to study the effect of the non-selective MMP and TNF-α converting enzyme (TACE) inhibitor GM6001 (30 mg/kg) on anastomosis repair in obstructed left colon. GM6001 has been proved to be highly efficacious in elective anastomosis rodent models.
Methods:
A partial obstruction of the distal colon was induced in male Sprague-Dawley rats. After 4 d the obstructed colonic segment was resected, and an end-to-end anastomosis was constructed. Seven days later, the anastomoses were evaluated for clinical leakage. Histopathological and immunohistochemical assessments were also performed. Finally, the direct effect of GM6001 on epithelialization was studied in cultured colonic epithelial cells.
Results:
Unlike the robust beneficial effect on anastomosis under uncomplicated conditions, here GM6001 had a negative impact on anastomotic wound healing following colonic obstruction and substantially (p=0.004) more rats in the GM6001 group (75%) than in the control group (11%) had developed anastomotic leakage. In the anastomotic wounds, the myofibroblast abundance and cell proliferation were similar in the two groups. Histologically, GM6001 treatment resulted in wider and minimally epithelialized wounds that were commonly necrotic on the luminal side and infiltrated with numerous granulocytes. In vitro, GM6001 also delayed (p=0.026) epithelialization of denuded intestinal epithelium grown on type I collagen.
Conclusions:
Non-selective MMP/TACE inhibition with GM6001 increased the anastomotic complications following colon obstruction. Inhibition of epithelialization is one possible mechanism responsible for the increased leakage following GM6001 treatment.
A
The collagen in the submucosal layer constitutes the suture-holding capacity and has a substantial effect on the integrity of anastomoses in the early healing phase [3,4]. During normal anastomotic healing, the breakdown and synthesis of collagen occur concurrently. Collagen breakdown, which dominates over synthesis in the early wound healing phase, is mediated by the action of proteolytic enzymes such as matrix metalloproteinases (MMPs) [4]. The expression of MMPs is low or absent in the normal colon, but it increases dramatically following tissue injury [3,5]. The over-expression of specific MMPs in resected colon at the time of surgery has been associated with clinical anastomotic leakage [6]. In pre-clinical models, pharmacological non-selective inhibition of MMPs improves the early anastomosis integrity [7]. The mechanisms of these drugs involve the protection of existing collagen fibers from degradation [3,8].
In acute obstruction models of anastomosis repair, MMP expression is further elevated, and more of the bowel wall is engaged over a longer post-operative period than under uncomplicated conditions [9–11]. MMP activity also correlates inversely with collagen concentration in the obstructed colon [12].
Our hypothesis was that the inhibition of MMPs would improve the outcome of high-risk colonic anastomosis. Specifically, our aim was to investigate the effect of pharmacologic MMP inhibition on the incidence of complications using a colon obstruction model with a 27% complication rate [13]. The compound GM6001 was selected because it inhibits the release of the potent MMP inducer tumor necrosis factor (TNF)-α [14,15] and was found the most efficacious non-selective pan-MMP inhibitor with respect to the biomechanical strength of experimental anastomoses in a recent meta-analysis [7]. Although GM6001 treatment inhibits epithelial migration [16,17] it was not detrimental to epithelialization under uncomplicated conditions possibly because it concurrently reduced the anastomotic wound gap [8]. Therefore, we also investigated the effect of GM6001 on epithelialization in vivo and in vitro here.
Patients and Methods
Experimental design
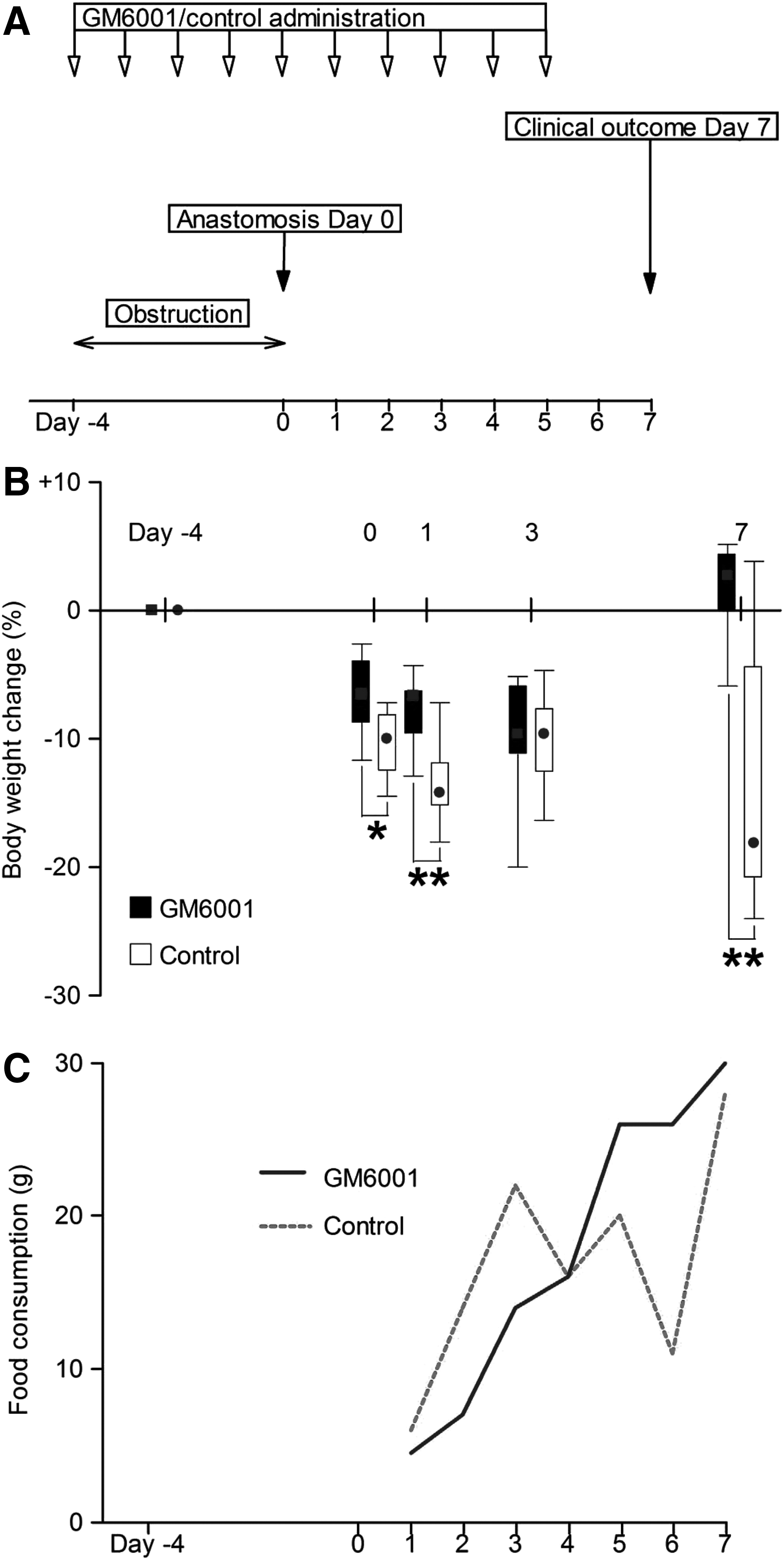
The aim of the in vivo study was to compare the effects of GM6001 (n=12) and the control treatment (n=12) on anastomotic leakage on post-operative day 7 after a 4-d obstruction period (Fig. 1A). To study the direct effects of GM6001 on epithelialization, an in vitro experiment was carried out using colonic epithelial cells cultured on type I collagen.
Design of the animal experiment
GM6001
GM6001 (AMS Scientific, Concorde, CA) is a non-selective hydroxamate-based MMP and TNF-α converting enzyme (TACE) inhibitor with an inhibitory profile for MMPs in the low nanomolar range [8,15,18,19]. The IC50 for TACE is 320 nM [19].
Animal study
Male Sprague-Dawley rats (Taconic, Lille Skensved, Denmark) of 7–8 w of age and weighing 210–276 g were used. The rats had free access to food pellets and tap water [8,12,20]. Our study was approved by the local ethics committee of Lund University (M174-04).
The rats were acclimatized for at least 7 d prior to surgery. Anesthesia was induced with a subcutaneous injection of fentanyl citrate (0.14 mg/kg), fluanisone (4.4 mg/kg), and midazolam (2.2 mg/kg), and was then maintained with fentanyl citrate (0.14 mg/kg).
The rats were allocated to GM6001 (30 mg/kg) or control (vehicle) treatment by randomization. Treatments were administered by subcutaneous injections 1 h prior to the surgery and then once daily for nine consecutive days (Fig. 1A). GM6001 was suspended in ethanol and diluted to 5 mg/mL with phosphate-buffered saline (pH 7.4). Ethanol and phosphate-buffered saline in the corresponding volumes served as the control treatment [8,15,16].
The skin was shaved and cleansed with chlorhexidine, and the peritoneal cavity was exposed through a 30 mm midline incision. Colonic obstruction was established on day −4 using a silicone ring, with an inner diameter of 6.5 mm around the distal colon, approximately 30 mm proximal to the peritoneal reflection [10,12,13,21,22]. The abdominal wall was then closed with continuous 4-0 polyglactin sutures in two separate layers. Four days later (day 0), the colonic obstruction was discontinued by the resection of a 10 mm colonic segment. An end-to-end anastomosis was constructed with nine interrupted 7-0 polypropylene sutures (Prolene®; Ethicon, Johnson & Johnson, Somerville, NJ). After surgery, the rats received 5 mL of a serum glucose (25 mg/mL) solution (Rehydrex®; Fresenius Kabi, Uppsala, Sweden) intra-peritoneally and subcutaneous buprenorphine (0.02 mg/kg) for post-operative analgesia. Then, the rats were maintained in separate cages to record food intake and the first passage of stool. The rats were killed by asphyxiation in a carbon dioxide chamber at the end of the experiment.
The International Study Group of Rectal Cancer classifies an abscess in the perianastomotic area as anastomotic leakage [23]. Essentially, this criterion for anastomotic insufficiency was applied to our experimental model. Accordingly, the anastomoses were graded on a five-point scale during dissection of the anastomotic area. Anastomotic leakage was represented by grades three or four (Table 1).
Histopathological and immunohistochemical evaluations were also performed on four representative anastomoses from each group. The tissues were formalin-fixed, paraffin-embedded and cut serially into 5 μm sections. One section was stained with hematoxylin and eosin to evaluate the longitudinal width of the anastomotic wounds [8], epithelialization [8], necrosis, edema, vascularity, and cellularity. Type I collagen was assessed in the adjacent section using Van Gieson and Alcian blue staining. The number of blood vessels and cells/degree of edema and necrosis was semi-quantitatively estimated on a four-grade scale as follows: None, few/slight, moderate, or many/severe.
The immunohistochemical staining was carried out using antibodies, reagents and the complete autostainer system from Dako (Glostrup, Denmark). A citrate buffer solution of pH 9 was used for α-smooth muscle actin, and a citrate buffer solution of pH 6 was used for Ki-67 epitope retrieval. The primary mouse monoclonal antibody against human α-smooth muscle actin (1A4 clone) was applied at the ready-to-use concentration for 30 min at room temperature. The primary mouse monoclonal antibody against rat Ki-67 antigen (MIB-5 clone) was used at a 1:30 dilution for 60 min at room temperature. These sections were counterstained with Mayer's hematoxylin. The α-smooth muscle actin was scored on a four-tiered scale with no, weak, moderate, or intense staining. Ki-67 labeling was indicated by the number of positive nuclei in 100 cells in five high-power fields (×400).
Effect of GM6001 on epithelialization in vitro
Caco-2 cells (American Tissue Type Culture Collection; Rockville, MD) were seeded into 96-well tissue culture plates (50,000 cells/well) coated with type I collagen (Cellcoat; Greiner Bio-One, Frickenhausen, Germany) the major ECM component of anastomotic wounds. The cells were incubated in 150 μl of Dulbecco's modified Eagles medium containing 10% fetal calf serum and antibiotics at 37°C in 5% CO2/air [24]. Twenty-three h after seeding, the media were supplemented with 10 μm GM6001 in 0.1% dimethyl sulfoxide (DMSO) or with 0.1% DMSO alone (control). After another 1 h of incubation, suction was applied through an ultrafine pipette tip, resulting in uniform defects of 0.50 mm2 in area. The aspirated media were returned to the wells and the incubation continued for 48 h. Photomicrographs were taken at 0, 24, and 48 h after denudation using a phase contrast microscope. The epithelial defect areas were determined by ImageJ 1.46r software (National Institutes of Health, Bethesda, MD), and the relative change in the cell-free area was calculated.
Blinding
Investigators performed all of the surgical procedures as well as the macroscopic and microscopic evaluations without prior knowledge regarding the allocated treatments.
Statistical analyses
Mann Whitney two-sided test or χ2 test were employed for the statistical analysis using SPSS® Statistics 17.0 (IBM Corporation, Somers, NY). p<0.05 was considered statistically significant. The data are presented as the median (interquartile range).
Results
Effect of GM6001 on body weight, food consumption, and bowel function
The animals in the GM6001 and control groups lost weight during the 4-d obstruction period. The body weight loss was greater (p=0.018) in the control group compared with the GM6001 group (Fig. 1B). The animals resumed eating after the discontinuation of the obstruction [22] and the construction of anastomoses on day 0 (Fig. 1C). Bowel function was restored 2.0 (1.0–2.8) d after the anastomoses were made in the GM6001-treated rats compared with 1.5 (1.0–2.5) d for the control animals (p=0.888). The GM6001-treated animals regained their initial body weight by day 7 in contrast to the vehicle-treated animals, which had lost 18.2% (p=0.006) of their initial body weight. Therefore, the GM6001-treated animals weighed substantially (p=0.003) more (259 (245–274) g) than the control animals (207 (200–222) g) on day 7.
Effect of GM6001 on leakage of anastomoses made in the obstructed colon
Three control animals were excluded; one rat died following the induction of anesthesia on day 0, another died on post-operative day 1 and the third rat died on post-operative day 3. The anastomoses in the two latter animals showed no signs of insufficiency. Three more animals, one control animal and two GM6001-treated, were prematurely killed on day 5 because of decreased well-being. In spite of stagnated feces proximal to the anastomoses, these segments were gradable.
Thus, 21 rats, 12 GM6001-treated and nine control-treated rats remained in the study for the macroscopic evaluations on days 5 and 7. These demonstrated that nine of the 12 anastomoses in the GM6001 group were grade three, corresponding to a leakage, compared with one of the nine anastomoses in the control group (Fig. 2). This difference between the GM6001 and control groups was statistically significant (p=0.004). The typical appearance of a grade three anastomotic complication revealed multiple firm adhesions covering an abscess the size of a pea (5–10 mm) originating from a perforation in the anastomotic suture line.
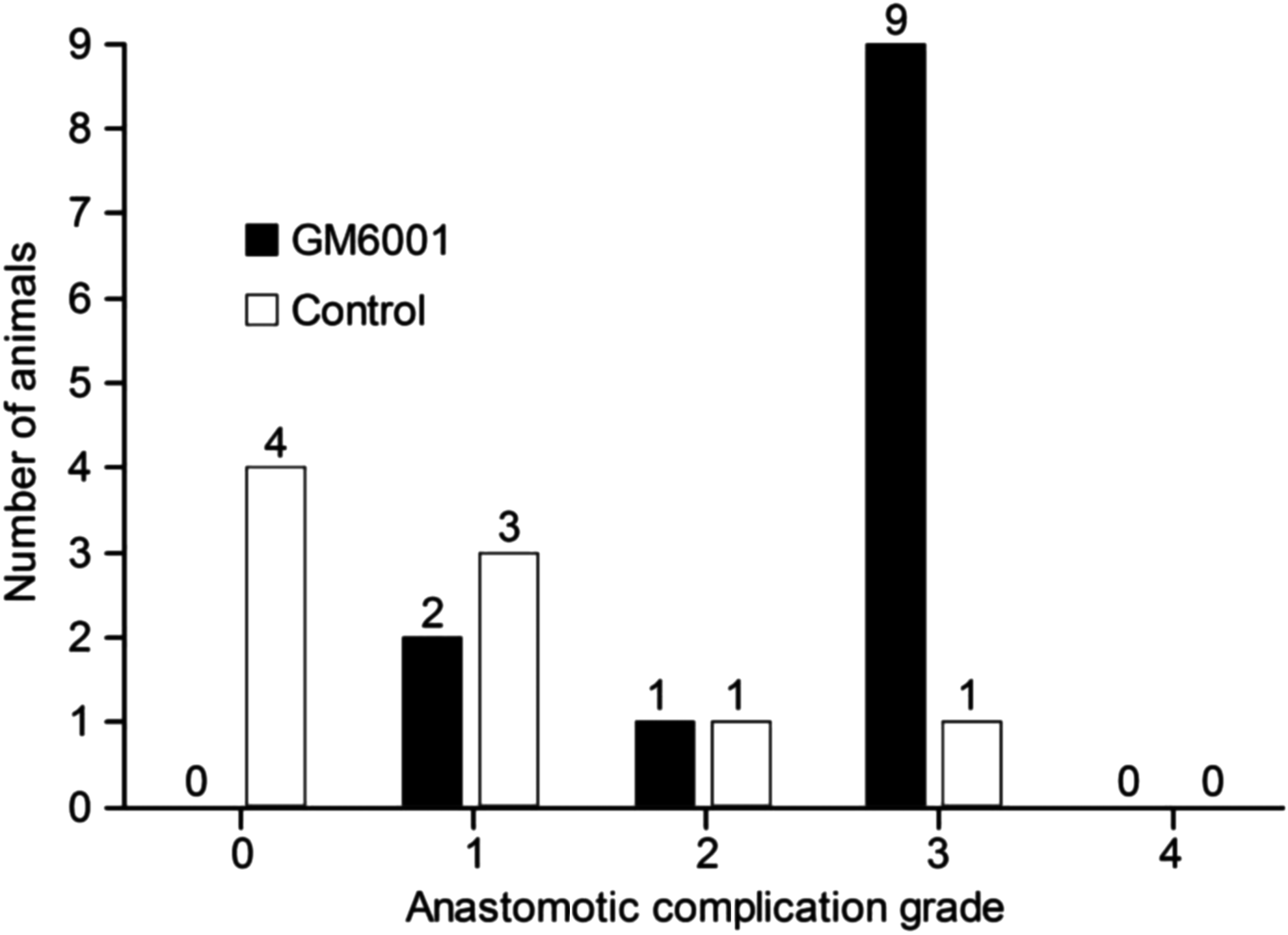
Effect of GM6001 on the healing of 7-day-old anastomoses using the criteria in Table 1 on a scale from 0 to 4. GM6001 (n=12) treatment increased (p=0.004, χ2 test) anastomotic leakage compared with the control treatment (n=9).
Histological and immunohistochemical analyses of the anastomotic wounds
The most prominent morphologic feature was the wider wound gap in the GM6001 treatment group compared with the control group (Fig. 3A–D). Another striking intergroup difference was the minimal epithelialization of the granulation tissue in the GM6001-treated rats compared with the control wounds, which were partially or completely covered with epithelium (Fig. 3A–D). Additionally, the necrosis on the wound surface facing the lumen was moderate to severe in the GM6001 group and absent to slight in the control group. The wounds were slightly edematous with a moderate number of blood vessels. The overall granulocytic infiltration was typically pronounced in the GM6001 group compared with the scattered granulocytes in the control wounds. There were few macrophages, lymphocytes, and plasma cells in either group. Mast cells were not observed in the granulation tissue, although they were occasionally present within the loose connective tissue of the adjacent uninjured colon [25]. Moreover, the amount of type I collagen appeared to be similar in the two groups (Fig. 3C and D). Immunostaining for α-smooth muscle actin indicated that myofibroblasts were the dominant cell types in the granulation tissue, although their abundance did not differ between the two groups (Fig. 3E and F). The proliferative activity was assessed by Ki-67 immunostaining and was low, with fewer than 5% of the cells in the wounds staining positive. There was no difference in the nuclear Ki-67 labeling between the GM6001 and control groups (Fig. 3G and H).
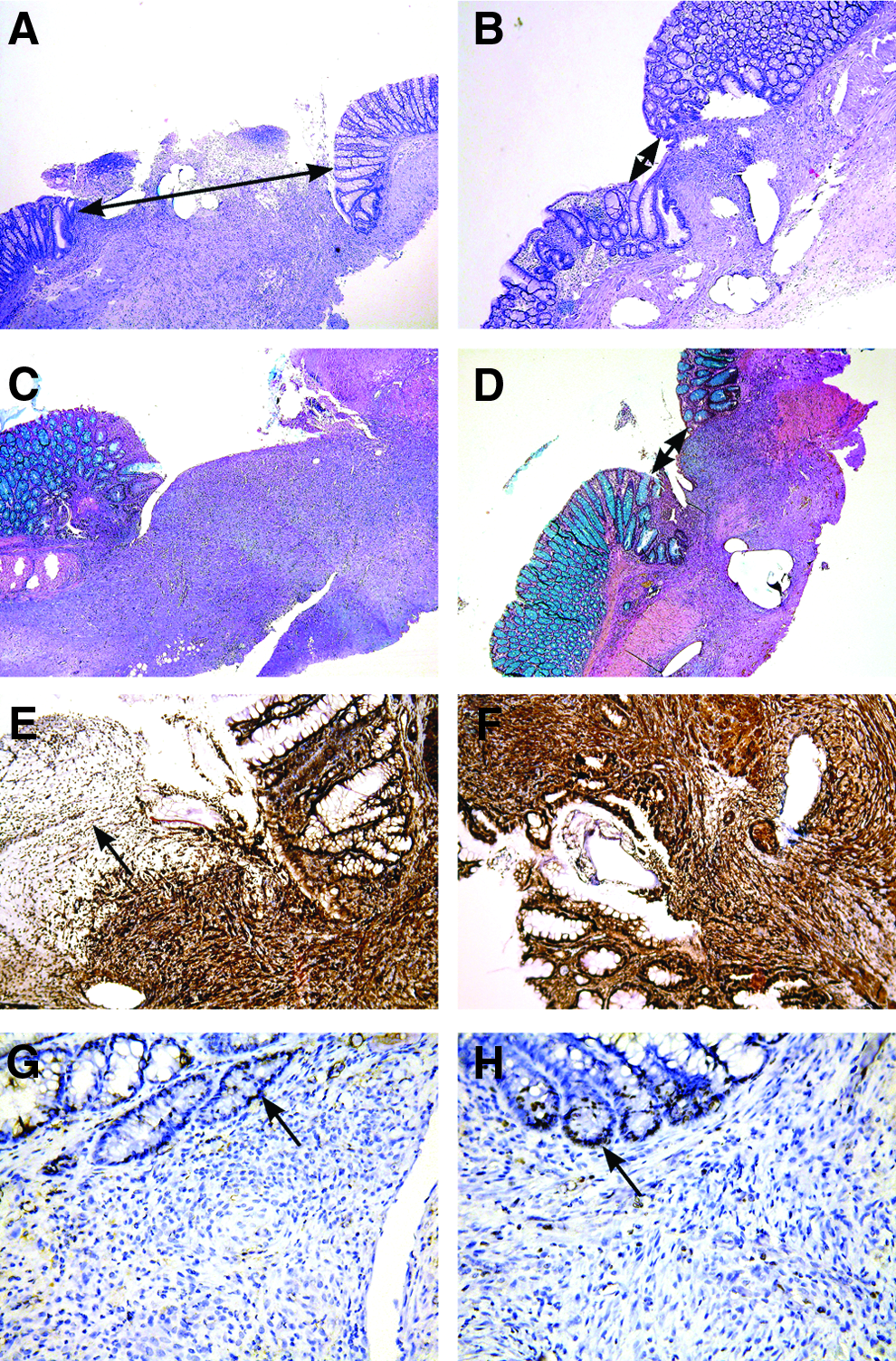
Effect of the MMP/TACE inhibitor GM6001 on morphology, myofibroblast abundance and cell proliferation in 7-day-old colon anastomoses (
GM6001 impaired epithelialization in vitro
Compared with the control treatment, GM6001 treatment impaired (p=0.026) the overall restitution of the standardized defects in colonic epithelial cell monolayer grown on type I collagen (Fig. 4).
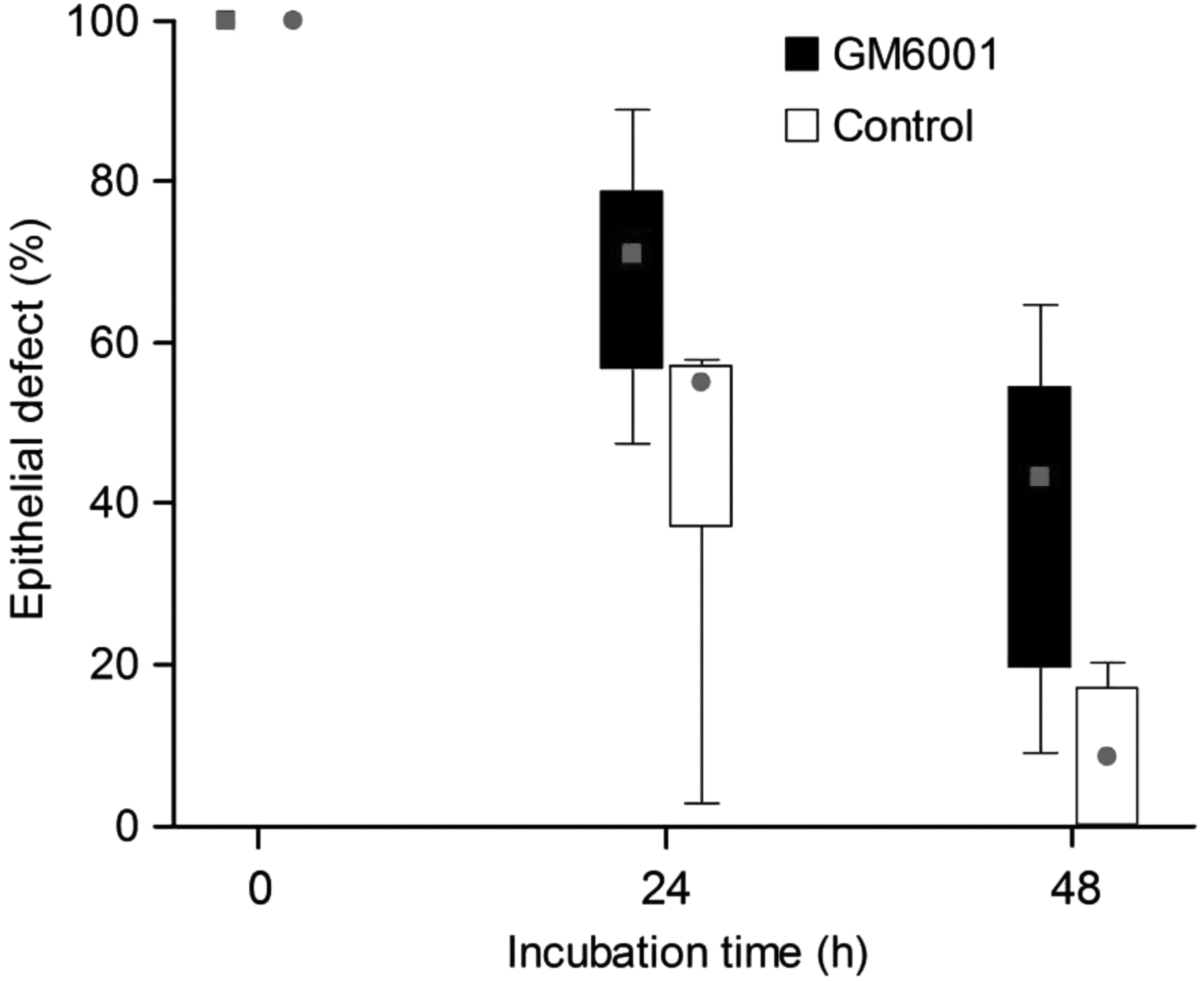
The effect of GM6001 on epithelial restitution using Caco-2 cells. Defects (0.50 mm2 in surface area) in the confluent epithelial layer were caused by applying suction to a micropipette tip. The cultures (n=6) were incubated in the presence or absence of 10 μM GM6001 in 0.1% DMSO (control). The epithelial defects were quantified by image analysis. GM6001 treatment impaired the overall epithelial restitution (p=0.026, Mann-Whitney two-sided test). The box represents the interquartile range; the whiskers represent the range; and the filled square (GM6001)/circle (control) within the box represents the median value.
Discussion
Emergency operations for the treatment of colonic obstruction are associated with increased anastomotic complications compared with elective operations [1,2]. Tissue-destructive MMPs are up-regulated in the obstructed colon and are responsible for collagen loss in the bowel wall [9,10,12,22]. Contrary to our expectations, non-selective MMP inhibition increased complications following anastomotic surgery of an experimentally obstructed colon.
Synthetic MMP inhibitors reproducibly improve the anastomotic integrity in non-obstructed colons as monitored by morphological criteria and increased biomechanical strength [7]. The biomechanical strength of the anastomosis is a surrogate for leakage under normal healing conditions. Törnqvist et al. [13] demonstrated that the breaking strength of the anastomoses made in the obstructed colon was greater than in the non-obstructed colon in spite of the increased complication rate after resection and anastomosis. Therefore, the breaking strength of anastomoses made under complicated conditions does not appear to predict anastomotic leakage.
The opposite and beneficial effects of GM6001 and similar synthetic MMP inhibitors on wounds in non-obstructed large bowel segments and in normal skin are difficult to understand [7,26]. Negative effects with a broad-spectrum MMP inhibitor similar to GM6001 were observed in an experimental model of periodontitis [27]. It was speculated that the effective attenuation of the more than 20 members of the MMP family is detrimental to the healing process and anti-microbial host defense mechanisms [28,29].
In another study in rats, GM6001 treatment neither impaired fibroblast/myofibroblast proliferation nor collagen deposition in skin [16] or peritoneal wounds [15]. Herein, GM6001 had no apparent detrimental effect on fibrotic processes. One striking difference between the two experimental situations was the increased wound gap in the obstructed colon with GM6001 treatment, whereas the opposite was found in uncomplicated anastomotic healing [8]. Theoretically, differences in the contractile myofibroblasts could account for the difference in the wound width. We immunostained the wounds for α-smooth muscle actin, which is a reliable marker of myofibroblasts [16]. This analysis indicated that the number of myofibroblasts was similar in the GM6001 and control groups [30]. α-Smooth muscle actin is also expressed by the pericytes and smooth muscle cells of the blood vessels in granulation tissue [30]. The histological and immunohistochemical observations were semi-quantitative, and small differences may have been overlooked. This and the small number of samples pose some limitations to these analyses.
The severely impaired epithelialization of the anastomotic wounds with GM6001 could be recapitulated in vitro. Defective coverage of the anastomotic wound with epithelium increases the risk for bacterial invasion [31]. This fact would explain the increased superficial necrosis and elicitation of a pronounced inflammatory response. Direct support of this proposed mechanism could be found in work on the potent epithelial mitogen keratinocyte growth factor that increased the mucosal regeneration and bursting pressure of the colonic anastomosis without a concomitant increased collagen concentration [31,32]. Taken together, we speculate that treatment with GM6001 delayed the restitution of the protective epithelial barrier, resulting in increased bacterial invasion leading to abscess formation.
The lower occurrence of anastomotic complications than predicted in the control group might be a reason for the substantial difference. Therefore, we carried out a theoretical calculation by simulating an increased leakage rate in the control group to three of 11 matching the earlier figures [13]. The GM6001-treated animals still had substantially (p=0.022) more anastomotic complications. Additionally, if only the animals that completed the entire 7-d post-operative period were included in the statistical analysis, the difference between the two groups remained significant (p=0.006).
To maximize the therapeutic effect of GM6001, animals were treated throughout the whole study period. Admittedly, this regimen is not applicable to the clinical situation where the drug would presumably be given after, and not before, the patient had developed colonic obstruction.
GM6001 belongs to the class of peptidomimetic MMP inhibitors [33] that also inhibit TACE, which is a sheddase for TNF-α [15,34]. The levels of TNF-α for optimal wound healing are unknown. Under uncomplicated conditions, inhibition of TNF-α signaling with a p38 mitogen-activated protein kinase inhibitor [8] and specifically with the anti-TNF-α antibody infliximab [35,36] had no effect on the biomechanical properties of intestinal anastomoses. Anti-TNF-α antibody therapies do not appear to increase anastomotic leakage in patients with Crohn disease [37–40] or ulcerative colitis [41,42].
In addition to its role as an immunostimulant, TNF-α induces cachexia [43]. The depression of circulating TNF-α by GM6001 treatment would explain the improved appetite and gain of body weight observed in this study.
The use of more selective MMP inhibitors devoid of TACE inhibitory activity [5] as an alternative to the local administration of MMP inhibitors would most likely be preferable for anastomosis repair in an obstructed colon. Sutures coated with a MMP inhibitor have also been shown to improve anastomotic healing [44].
In conclusion, the non-selective inhibition of MMPs and TACE with GM6001 increased the leakage of high-risk anastomoses in the obstructed large bowel of rats.
Footnotes
Author Disclosure Statement
No competing financial interests exist.