
Abstract
Abstract
Background:
Necrotizing fasciitis (NF) is a potentially fatal subcutaneous tissue and fascia infection. We studied the role of serum procalcitonin in the identification and assessment of severity of sepsis in patients with NF.
Methods:
A retrospective analysis was conducted from January 2000 to December 2013 for all patients who admitted to surgical intensive care with provisional diagnosis of NF. Patients were categorized into four groups based on the initial procalcitonin concentrations (Group I: <0.5 low risk, Group II: ≥0.5–<2 moderate risk, Group III: ≥2–<10 high risk, and Group IV: ≥10 ng/mL high likelihood of severe sepsis).
Results:
During the study period, 331 cases were identified to have NF with a mean age of 51 ± 14 years. Serum procalcitonin was tested in 62 cases (only between 2011 and December 2013) and all were positive (Group I: 22%, Group II: 18%, Group III: 21%, and Group IV: 39%). The most common affected regions were thigh and chest in Group II (46% and 9%, respectively), lower limbs in Group III (46%), and perineum and abdomen in Group IV (25% and 21%, respectively). In the four groups, 21 patients developed septic shock (Group I: 0%, Group II: 14%, Group III: 24%, and Group IV: 62%). The cut off procalcitonin value for septic shock was 5.6 ng/mL. Using receiver-operating characteristic curve, this cut off with the Area under the Curve (AUC) of 0.77 was found to have sensitivity 81% and specificity 67%. Sequential Organ Failure Assessment (SOFA) score was substantially greater in Group III and Group IV in comparison to Group I and Group II, p = 0.006. Procalcitonin levels were correlated well with SOFA score (r = 0.34, p = 0.007). There were 17 deaths in the four groups (Group I: 6%, Group II: 23%, Group III: 12%, and Group IV: 59%).
Conclusion:
Initial procalcitonin concentration in NF carries an important prognostic value and it correlates well with SOFA score and can predict the development of septic shock early in patients with NF.
N
Sepsis occurs when inflammatory responses are triggered throughout the body during infection. These inflammatory responses can damage multiple organ systems and cause them to fail [3]. It was estimated that nearly nine million people worldwide die annually from sepsis [3–5]. In the past decade, hospitalization rates for sepsis more than doubled, and these patients stayed longer than other patients and were eight times more likely to die during their hospitalization [6]. Often it is difficult to distinguish sepsis from non-infectious conditions which show signs of acute inflammation in critically ill patients. Numerous studies suggest that procalcitonin is a possible marker of SIRS related to infection [6,7]. Prior studies showed that procalcitonin is superior to C-reactive protein (CRP) in identification and severity assessment of sepsis; however, both markers cannot be used alone in differentiating infectious from noninfectious clinical syndrome [8]. Mortality remains high in NF despite the use of modern powerful antimicrobial drug regimens and advances in the care of the critically ill patients. We studied the role of initial serum procalcitonin concentration in the development and assessing the severity of sepsis in patients presenting with NF.
Patients and Methods
We conducted a retrospective analysis of all patients admitted to surgical intensive care unit with provisional diagnosis of NF at Hamad General Hospital (HGH) in the state of Qatar between January 2000 and December 2013. Demographic data, clinical features, site of infection, type of comorbidities, laboratory findings and outcomes were analyzed. The number of operative debridement, intensive care unit (ICU) and hospital stay and mortality were also documented.
The procalcitonin test has been introduced recently in HGH; therefore, not all NF cases in the past underwent procalcitonin assessment at admission. Serum procalcitonin concentrations on admission (within 24 h) were tested in 62 cases (between January 2011 and December 2013) and accordingly patients were categorized into four groups based on the initial procalcitonin concentration (Group I: <0.5 low risk; Group II: ≥0.5–<2 moderate risk; Group III: ≥2–<10 high risk; and Group IV: ≥10 ng/mL high likelihood for sepsis) [9–11].
Definition
NF was diagnosed upon clinical and laboratory assessments on arrival and during the hospital course based on signs and symptoms defined by the U.S. Centers for Disease Control and Prevention and the National Necrotizing Fasciitis Foundation and scoring [1–2]. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score was calculated using parameters such as CRP, white blood cell count, hemoglobin, sodium concentration, creatinine concentration, and serum glucose concentration [12]. Further confirmatory permanent section biopsy for all cases and intra-operative frozen section biopsy for gram staining were performed whenever applicable.
Sequential Organ Failure Assessment (SOFA) score was calculated using parameters such as the ratio of partial pressure arterial oxygen and fraction of inspired oxygen (PaO2/FiO2), platelets count, bilirubin concentration, Glasgow coma score, Mean Arterial Pressure, use of vasopressors, creatinine concentration, and urine output [13]. Septic shock was defined as sepsis-induced hypotension (i.e., systolic blood pressure less than 90 mmHg or a fall in systolic blood pressure of >40 mmHg persisting despite adequate fluid resuscitation [14].
Statistical analysis
Data were presented as proportions, median (range) or mean (±standard deviation), as appropriate. Baseline demographic characteristics, medical history, clinical presentation, and outcomes were compared between the four groups according to initial procalcitonin concentrations. Analyses were conducted using ANOVA test for continuous variables and Pearson chi-square (χ2) test for categorical variables. A two-tailed p < 0.05 was considered significant. Receiver-operating characteristic curves were plotted to identify initial procalcitonin concentration cut-off values for predicting septic shock. The area under the curve (AUC) was used to compare the discriminatory power of the scoring system or other clinical variables of interest, with an AUC of 1.0 considered perfect discrimination and 0.5 considered equal to chance [15]. The correlation between procalcitonin and SOFA was performed using Pearson correlation and was considered substantial at the 0.01 concentration (two-tailed). Data analysis was carried out using the Statistical Package for Social Sciences version 18 (SPSS Inc, Chicago, Illinois).
Results
During the period between 2000 and December 2013, there were 331 cases admitted with NF. In the era from January 2011 to December 2013, there were 93 NF cases; serum procalcitonin concentrations were tested in only 62 cases (67%). All procalcitonin values were positive. These 62 cases were categorized according to the value of procalcitonin into four groups (Group I: n = 14; 22%, Group II: n = 11; 18%, Group III: n = 13; 21%, and Group IV: n = 24; 39%). Forty-seven patients were males and 15 were females (mean age 52 ± 14 years) (Table 1). Of these 62 patients, 45% were South Asian. Age and gender were comparable among the four procalcitonin groups (Table 2). NF patients frequently presented with pain and tenderness (66%), swelling (66%) and fever (53%); however, no substantial differences among the groups were observed in terms of initial clinical presentations. Diabetes mellitus (63%) was the most common comorbidity observed among the procalcitonin cohort. Minor trauma was reported in seven (12%) patients.
Intraoperative frozen section biopsy from gram staining.
SOFA = Sequential Organ Failure Assessment; LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis; ICU = Intensive care unit; DM = diabetes mellitus; ICU = intensive care unit; Los = length of stay.
Intraoperative frozen section biopsy for gram staining
SOFA = Sequential Organ Failure Assessment; LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis; ICU = Intensive care unit.
The common organism causing infections was streptococcus (37%) followed by staphylococcus (31%). There were no substantial differences in the frequencies of gram-positive or -negative and mono- or polymicrobial infections among the four groups. The most common affected regions included the thigh in Group II (46%), lower limbs in Group III (46%), and perineum and abdomen in Group IV (25% and 21%, respectively). Neck or facial regions were affected mainly in Group I (29%) and Group II (9%) (Table 2). All the NF cases were confirmed by permanent section biopsy; however, intra-operative frozen section biopsy for gram staining was performed in approximately half of the cases (Table 1).
As there were missing SOFA score values (12.9%), SPSS-replacing missing data using multiple imputation was utilized. SOFA score was substantially greater in Group IV (13.9 ± 3.4) in comparison to Groups III, II, and I (12.8 ± 3.4, 10.5 ± 5.9, and 10.2 ± 2.2, respectively), p = 0.008.
Serum creatinine concentration increased substantially with an increase in procalcitonin concentration, and Group IV had the highest concentration (median = 236, ranges from 48 to 750 mcmol/L). Serum bilirubin concentration was also found to increase with increasing procalcitonin concentration and was approaching the traditional significance concentration (p < 0.05) among the risk groups for severe sepsis (p = 0.06). Among the 62 cases, CRP was tested in 59 cases (95%) with mean value of 195 ± 124 (Table 3). The mean CRP value was exponentially increasing from Group I to Group IV (p = 0.03) (Table 2).
In the era from 2000 to 2010; *In the era from 2011 to 2013.
SOFA = Sequential Organ Failure Assessment; LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis.
LRINEC scores increased with an increase in procalcitonin concentrations. It was >6 for 50–91% of patients in all the study groups. For Group III and Group IV, 91% and 83% of NF patients had an LRINEC score ≥6. Median LRINEC score values ≥8 were found in Group III and Group IV (10 and 8, respectively), p = 0.02.
In the four groups, 21 patients developed septic shock (Group I: 0%, Group II: 14%, Group III: 24%, and Group IV: 62%). The number of surgical debridement was comparable in the four groups. Also, all of the four groups had a comparable number of surgical interventions. The ICU length of stay was found to be substantially increased with the increase in procalcitonin concentrations (p < 0.05). Table 3 depicts comparison between NF patients based on whether procalcitonin status (tested or not). The occurrences of SOFA (p = 0.001) and septic shock (p = 0.08) were greater in the procalcitonin tested group.
The procalcitonin cut-off value for septic shock was 5.6 ng/mL. Using receiver-operating characteristic (ROC) curve; this cut-off with the area under the curve (AUC) of 0.77 (95% Confidence interval [CI]: 0.65–0.89, p = 0.001) was found to have sensitivity 81% and specificity 67% (Fig. 1). In the same ROC, CRP was not good as procalcitonin for identification of septic shock (AUC = 0.51, p = 0.83).

Prediction of septic shock based on procalcitonin concentrations. Procalcitonin cut-off = 5.57. Area under curve (AUC) is 0.77 (95% CI 0.65–0.89, p = 0.001), sensitivity =81%, and specificity = 67% C-reactive protein (CRP): AUC is 0.51, p = 0.83.
Pearson correlation demonstrated a positive correlation between procalcitonin and SOFA score; r = 0.34, p = 0.007. In Figure 2, Boxplot shows the correlation between procalcitonin groups and SOFA score. The mortality rates in the four groups were reported in 17 patients (27.4%) as follows (Group I: 7%, Group II: 36%, Group III: 15%, Group IV: 42%). Although it is of clinical importance, the difference between groups in terms of mortality was not statistically significant. The number of deaths was greater in Group IV (n = 10) followed by Group II (n = 4) (Fig. 3).
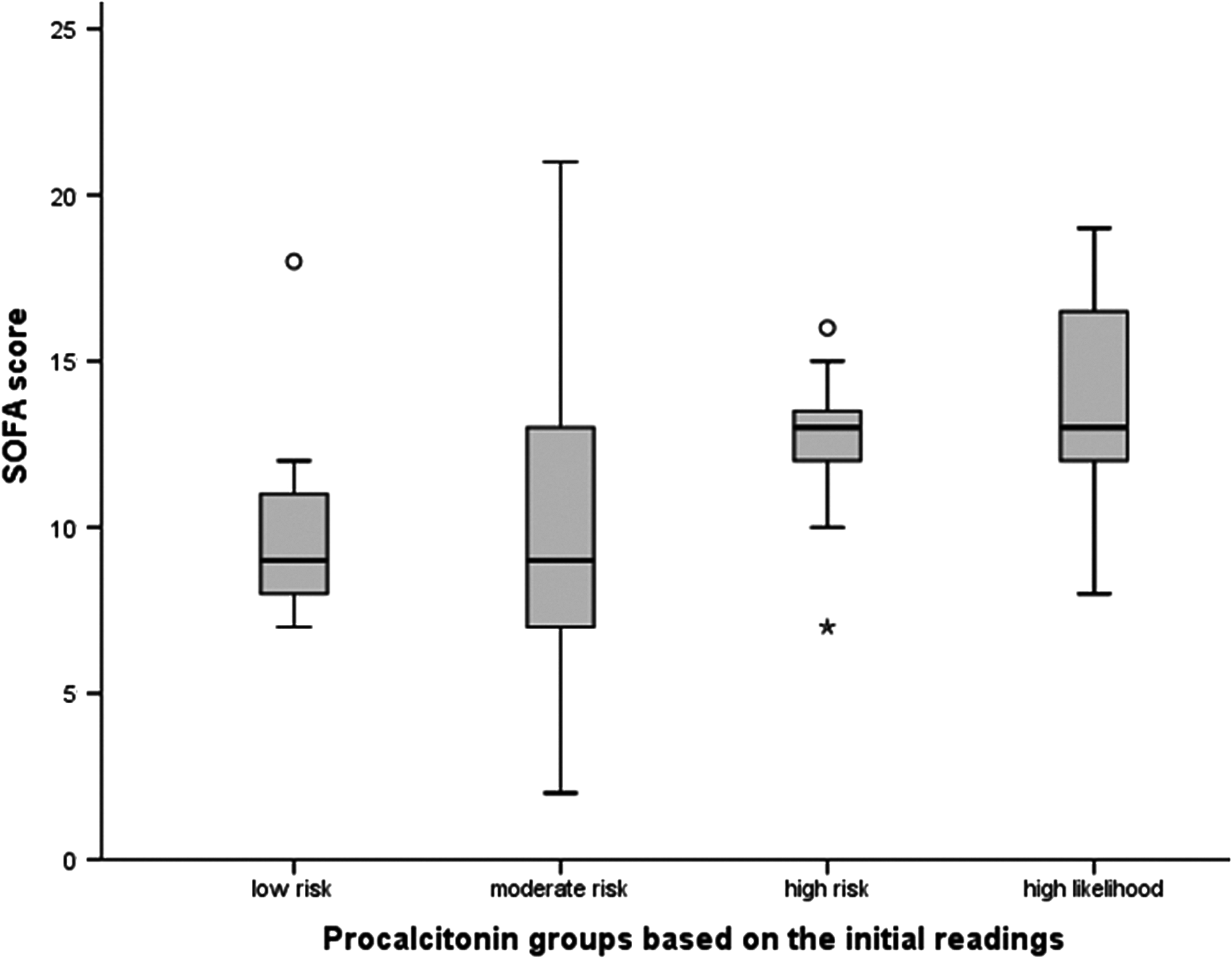
Procalcitonin groups based on the initial readings.

Outcomes in necrotizing fasciitis based on the procalcitonin concentrations (p = 0.02 for septic shock and p = 0.08 for mortality).
Discussion
We report a unique study from our region to evaluate the role of initial readings of procalcitonin in the prediction of septic shock in NF. This study has many key findings. The frequencies of septic shock and death are high among NF patients. In addition to procalcitonin, we correlated the SOFA score with the different concentrations of procalcitonin. Early diagnosis of sepsis is crucial because it helps to reduce mortality rates associated with NF with timely surgical intervention [16–18]. Consistent with the previous studies, our study population has a high mortality rate of 27% [3]. We also reported a septic shock rate of 37% in the present study. A recent multicenter study showed substantial inter-hospital variations in patient characteristics, microbiology, and etiology of NF [16]. The authors showed that patient's age and severity of NF were the main predictors of mortality and the mortality rate varied from 9% to 25% in different hospitals even within a defined region [16]. Kao et al. showed that mortality rate varied with hospitals, from 9 to 25% [16]. The rate of hospitalization for patients with sepsis by gender showed similar hospitalization rate for males and females [4].
Procalcitonin was found to be linked with sepsis and has been part of research since the last three decades [19–20]. Nelson and et al. pointed out the favorable kinetics of procalcitonin as a predictor of sepsis as follows: It increases prior to 2 h, is reliably detectable between 2 to 4 h, has a peak concentration at 6 h, and maintains a plateau through 8 to 24 h [20]. Moreover, serum procalcitonin is detectable in low concentrations in healthy individuals, which can increase 1000-fold during active infection [20]. Normal serum procalcitonin concentration in a healthy individual is <0.05 ng/mL. Patients with procalcitonin concentration of <0.5 ng/mL are unlikely to have sepsis. However, this concentration does not exclude infection, because localized infections without systemic signs are still possible. In this case, procalcitonin could be reassessed after 6–24 h. Procalcitonin concentration of ≥0.5–2 ng/mL indicates moderate risk for progression to severe sepsis. Procalcitonin concentration of ≥2–<10 ng/mL is associated with high risk for progression to severe sepsis. High likelihood for severe sepsis or septic shock is associated with procalcitonin ≥10ng/mL [9–11]. Our finding showed that increased severity of NF and development of septic shock was associated with high serum procalcitonin concentrations on hospital admission. Among the study population, 21% patients were at high risk and 39% were at high likelihood for septic shock. In high likelihood for septic shock, procalcitonin concentration increased to 600-fold of normal concentration. This group of patients had the highest proportion of septic shock (57%), whereas none of the patients within the low risk group developed septic shock.
The role of procalcitonin concentration in predicting sepsis in patients of different age groups and in different conditions was studied by several authors such as Assicot et al. (newborn to age 12 y), Park et al. (neonates), Sitter et al. (kidney disease), and Delevaux et al. (inflammatory syndrome) [21–24]. Assicot et al. showed that high procalcitonin concentrations were related to acute septic episodes in children, but the reference range used was different [21]. They demonstrated that a range of 0.1–120 ng/mL was closely related to infectious complications and acute septic episodes. High serum procalcitonin (range 6–53 ng/mL) at diagnosis was reported in 24% of patients with severe bacterial infections. Conversely, 27% of patients with no signs of infection had procalcitonin concentration less than 0.1 ng/mL. Procalcitonin concentrations in 14% of patients with local infections without invasive sepsis were within or slightly above the normal range (0.1–1.5 ng/mL) [21].
Park et al. also demonstrated increased severity of infection with high procalcitonin concentrations [22]. This study showed that 0.5 mg/L is the best cut-off value of procalcitonin for diagnosing neonatal bacterial infection. Multiple studies compared the utility of serum procalcitonin concentration with other biomarkers in predicting the progression of severity of sepsis in bacterial infection. Sitter et al. [23] compared procalcitonin with CRP concentrations in 197 patients with kidney disease and 97% of the patients who underwent hemodialysis had procalcitonin concentrations between 0.5 and 1.5 ng/mL. However, it elevated substantially (61.50 ± 115.4 ng/mL) in renal failure patients with bacterial infections. Loss of renal function, immunosuppressive agents, or autoimmune disorders does not affect procalcitonin concentrations substantially. Delevaux et al. [24] showed a value of procalcitonin >0.5 ng/mL is a marker of bacterial infection with sensitivity 65%; specificity 96%; positive predictive value 89%; and a negative predictive value 84%. No false positive results were reported for procalcitonin concentrations >1.2 ng/mL.
Simon et al. showed procalcitonin concentration was more sensitive and specific than CRP concentration for differentiating bacterial infections from non-infective causes of inflammation [25]. Holub et al. argued that serum procalcitonin kinetics can be used for monitoring the effect of antibiotic therapy [26]. Tamaki et al. showed diagnostic accuracy of procalcitonin in bacterial infections was 0.79 (sensitivity 53.3%, and specificity 97.1%) [27]. The odds ratio of procalcitonin ≥0.5 ng/mL was substantial for identifying bacterial infection. In our study, the cut-off procalcitonin value for septic shock was 5.6 ng/mL. The specificity and the sensitivity of this procalcitonin concentration were 67% and 81%. SOFA score have been used to assess organ function or the rate of organ failure [13]. In critically ill patients, initial SOFA scores less than nine predicted a lower mortality rate of 33% compared with score greater than 11, which predicted a mortality rate of 95% [28]. Sudhir et al. prospectively studied the relation of procalcitonin concentrations with SOFA scores and mortality rates in various stages of sepsis [29]. A substantial association between serum procalcitonin and SOFA scores (p < 0.05) was reported. However, serum procalcitonin concentrations did not predict mortality in their study. The sensitivity of procalcitonin concentrations to predict sepsis was 94%. Notably, respiratory tract infection was the frequent source of sepsis in their study. Our study also revealed a substantial association between the median SOFA scores and procalcitonin concentrations (p = 0.006). Median SOFA scores were above 11 in both high likelihood for sepsis (13, [8–19]) and high risk group (13 [7–16]) patients in our study. Lower limb, perianal, and abdominal regions were common regions associated with high risk for sepsis or organ failure in the present study. However, this was not statistically significant.
Of note, no substantial difference was observed between the number of surgical debridement performed among the four groups. Although the number of deaths increased with increasing the procalcitonin concentrations in Groups I, II, and IV, this observation was not statistically significant. We could not find an explanation for the lower number of deaths in Group III in comparison to Group II except for the age factor, as Group III patients were eight years younger.
Limitation of the study
The retrospective design and the relatively small sample size are limitations of the study. However, this number of NF cases is considered high in Qatar, which is a developing country with high GDP per capita, up-to-date health care services and a total population of 1.8 million people in 2012. Serum procalcitonin has been established as a diagnostic test in almost all the suspected NF cases in our hospital since 2011. CRP concentrations were measured in 95% of the 62 NF cases with positive procalcitonin. Although the proportions of the development of septic shock and mortality were greater after using procalcitonin test (2011–2013), these differences were not statistically significant when compared with the era from 2000–2010.
Conclusion
Initial procalcitonin concentration in NF carries an important prognostic value, and it correlates well with SOFA score, and can predict the development of septic shock in its early stage.
Footnotes
Acknowledgments
This study was approved by the medical research center at HMC, Qatar with IRB#14066/14.
Author Disclosure Statement
All the authors have read and approved the manuscript, and all have no conflict of interest and no financial issue to disclose.