
Abstract
Abstract
Objective:
We aimed to assess the efficacy of applying a two-stage primary total knee arthroplasty (TKA) with an antibiotic-laden cement spacer block to treat infected osteoarthritic knees.
Methods:
This retrospective study included 17 cases of severely infected osteoarthritic knees treated with two-stage primary TKA. Open debridement and irrigation with insertion of a well-designed antibiotic cement spacer was performed as the first stage. Systemic antibiotics were used in the interval period. Two-stage TKAs were performed after elimination of infection. The pre- and post-operative Hospital for Special Surgery Knee (HSS) score as well as range of motion (ROM) were assessed.
Results:
Elimination of infection was achieved in 16 patients. C-reactive protein returned to normal levels in an average of 3.4 wks (range, 1–7 wks), whereas erythrocyte sedimentation rate (ESR) recovered in an average of 11.4 wks (range, 6–19 wks). The average interval between the two-stage operations was 16.8 wks (range, 10–27 wks). Compared with the pre-operative level, the mean HSS score had a substantial increase after the first-stage and second-stage surgery (p<0.05). The post-operative maximum extension degree was smaller and the maximum flexion and ROM degree were larger than the pre-operative degree (all p<0.05). There were no recurrent infections and no patients lost to follow-up. One patient chose to receive arthrodesis because of uncontrolled infection after numerous operations and treatments.
Conclusions:
Two-stage TKA with open debridement, irrigation, and insertion of a well-designed antibiotic-laden cement spacer at the first stage could provide effective pain relief and function restoration as well as infection control in the interval. This treatment protocol provided an encouraging final clinical outcome, which could be a reliable alternative for patients with infected osteoarthritic knees.
S
Patients and Methods
Ethics statement
The study was approved by the local ethics committee (Ethics Committee of Shanghai Changzheng Hospital) and written informed consent was obtained. A retrospective case series study was performed to review all 17 patients who underwent two-stage TKA to treat infected osteoarthritis between June 2006 and November 2012.
Patients
The patients included 6 men and 11 women with a mean age of 63.7 y (range, 43–74). These patients had an average Hospital for Special Surgery Knee (HSS) score of 37.7 (range, 19–56), and an average knee range of motion (ROM) of 64.7 degrees (range, 40–100 degrees). All had a flexion contracture to some extent (average, 12.1 degrees; range, 5–20 degrees). Eight had a history of knee injections, three had a history of arthroscopy for osteoarthritis, two were infected after knee trauma, one had a previous knee arthrotomy to remove loose particles, and the other three had no history of knee operation or infection (no overlap for each type of patients). Diagnosis was confirmed by laboratory parameters (erythrocyte sedimentation rate [ESR] and levels of C-reactive protein [CRP]), radiologic examination, and bacterial culture result of joint fluid and positive symptoms (purulent drainage, fever [temperature >38°C], localized pain, or tenderness). They were all diagnosed with infected osteoarthritis (Fig. 1). Nine of these patients had positive pre-operative cultures for the following organisms: Staphylococcus epidermidis, four; S. aureus, three (one methicillin-resistant S. aureus [MRSA] case), one Streptococcus and one Pseudomonas aeruginosa. Six had negative pre-operative cultures and another two patients had no results because of no joint fluid was extracted. All had high levels of ESR and CRP, and some had a high white blood cell count (Table 1).

Pre-operative image. An anteroposterior radiography of a 65-y-old female with infected osteoarthritis of the left knee.
Pre- means before the first-stage surgery.
HSS=Hospital for Special Surgery Knee score; ROM=range of motion; ESR=erythrocyte sedimentation rate; CRP=C-reactive protein; MRSA=methicillin-resistant Staphylococcus aureus.
The two-stage TKA protocol for osteoarthritic knees
The surgical procedure consisted of a routine midline skin incision, a routine medial parapatellar arthrotomy and a complete synovectomy, and radical debridement of infected or necrotic tissue. An intra-operative frozen section and bacterial cultivation of synovium and joint fluid were taken to confirm the diagnosis and optimize antibiotic choice. Bone cuts were made according to the size of the spacer block and all cuts were under extra-medullary guidance to avoid intra-medullary contamination. Patella were not cut at this stage. The osteophytes were removed completely and adequate soft tissue balancing and knee alignment were performed. The spacer block consisted of 80 g of Palacos R+G bone cement (Heraeus Medica, Hanau, Germany) mixed with gentamycin (4.8 g) and vancomycin (8 g). The antibiotic-loaded bone cement was poured into the spacer block mold at liquid stage, which was shaped as the prosthesis and taken out at the curing period. The spacer block was then molded (Fig. 2). The femoral spacer block was inserted first and then an appropriate tibial spacer block adjusted by the extension gap was inserted so that the limb was aligned and tissue tension was prevented. The spacer block should cover the full surface of bone ends. Routine closure and closed suction drains were used after numerous irrigations. The operated knee was placed straight and the drainage was removed within 48 h after surgery. Intravenous antibiotics were used for 1 wk. Optimal antibiotic was used with patients under bacterial culture and sensitive results whereas vancomycin was used for those without culture and sensitive results. Oral antibiotics (rifampicin+[optimal antibiotics/vancomycin]) were continued until two successive CRP results were normal and ESR results were below twice the value of the high threshold or had a continuous downtrend with no positive signs and symptoms. The CRP and ESR were followed every day in the first week and every 2 wks thereafter. The arthroplasty could be performed subsequently.
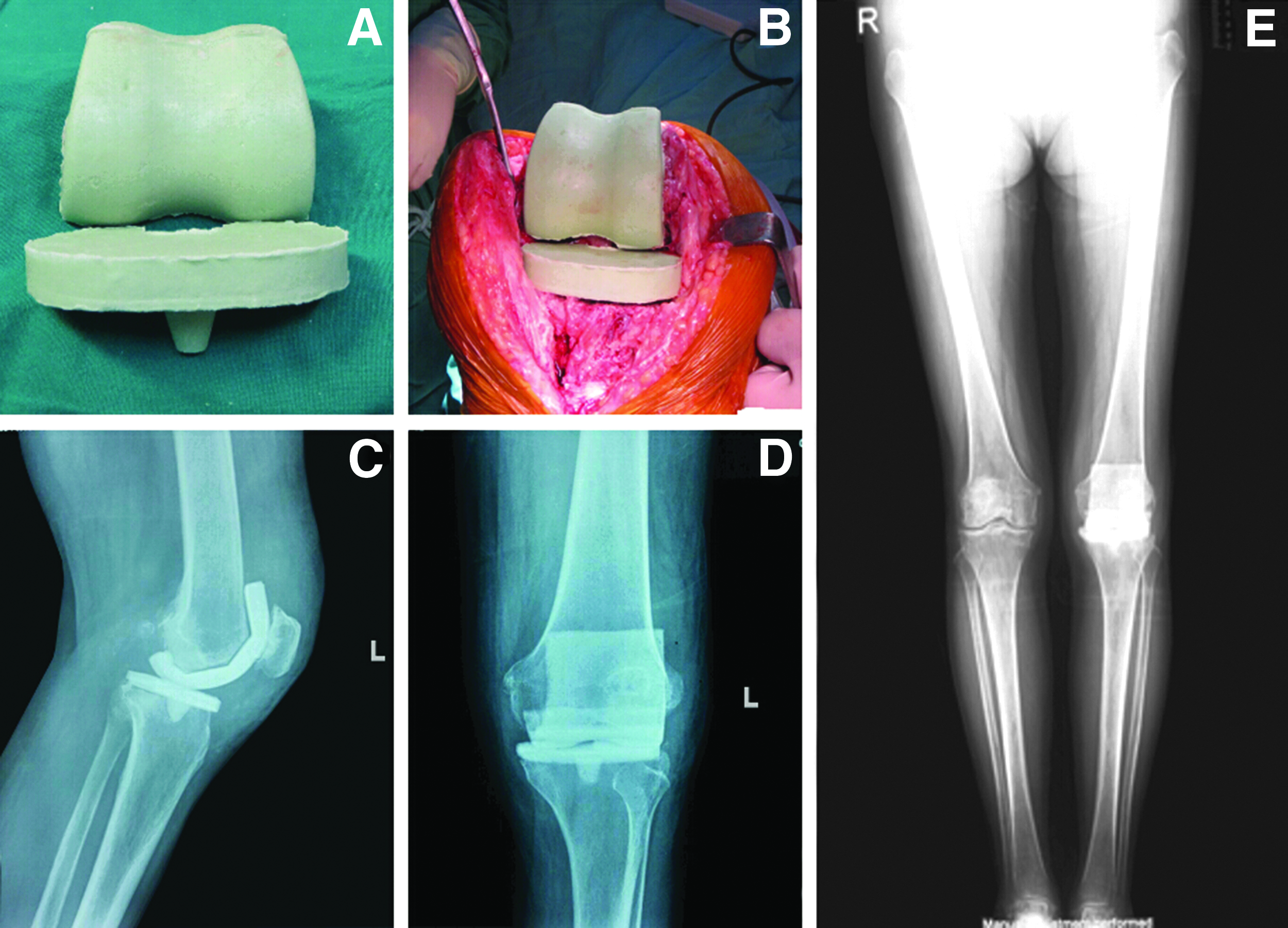
Well-designed antibiotic-laden cement spacer block. (
The initial incision was used and the surface of the bone ends were polished appropriately with a minimal intra-capsular and soft tissue dissection after retrieving the spacer block. Culture and a frozen section should be taken in patients in whom purulent fluid or substantial granulation tissue remain at surgery. The implantation procedure was the same as the primary TKA (Fig. 3). Posterior stabilized prosthesis was selected, patella replacement was performed, and antibiotic-loaded bone cement was used (40 g bone cement with 1 g vancomycin). Intravenous antibiotics (optimal antibiotics/clindamycin) were used for 3 d after implantation and oral antibiotics (rifampicin+[optimal antibiotics/clindamycin]) were continued for another 4 wks. Routine rehabilitation and functional training were undertaken and all patients were followed up at 6 wks, 12 wks, 6 mo, 12 mo, and once per year thereafter.
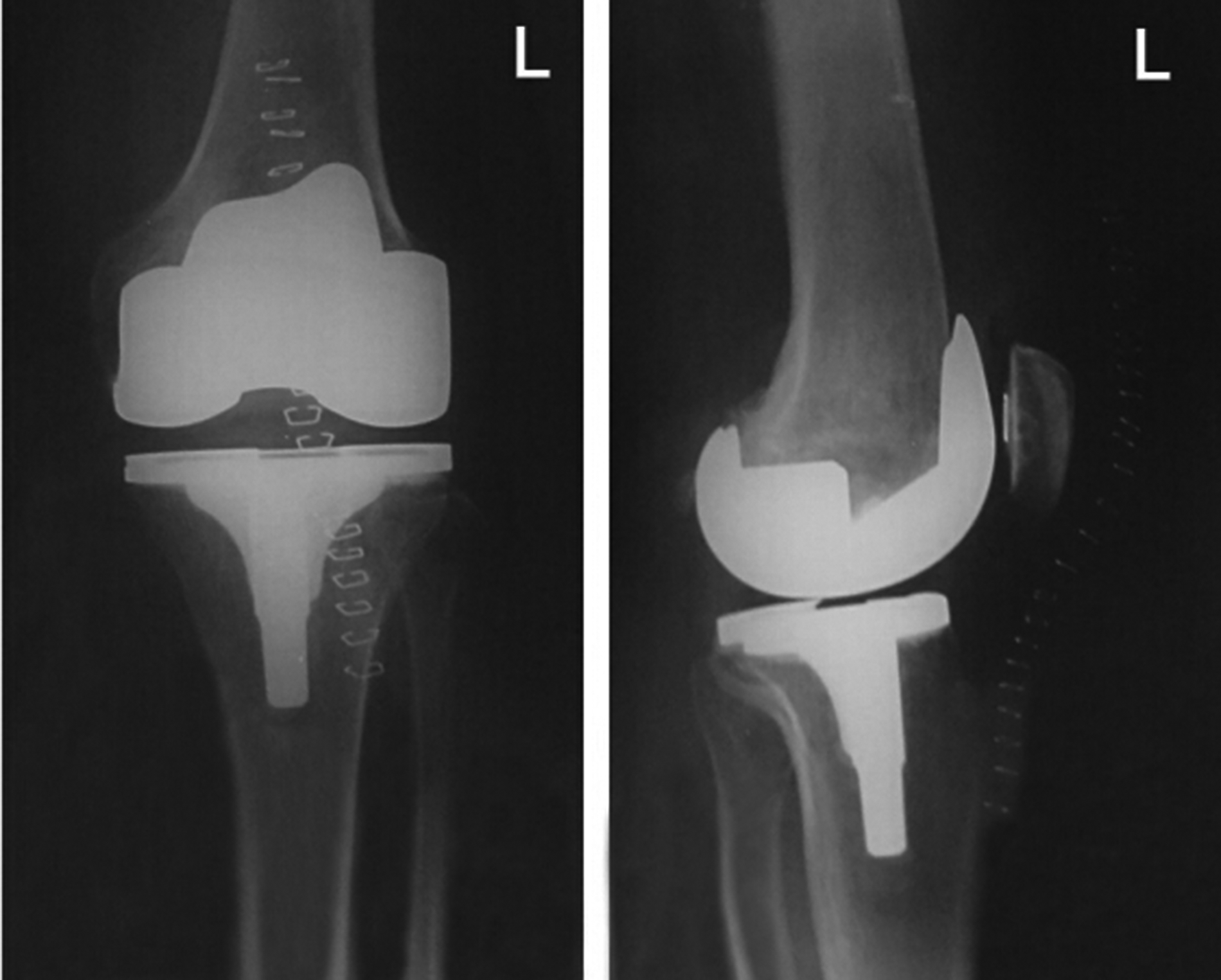
Post-operative image. Anteroposterior and lateral views after arthroplasty.
A repeated debridement and a replacement of a new spacer block was performed when the result of the frozen section still showed infection. Arthrodesis could be a therapeutic choice for patients whose infection could not be controlled by repeated operations and antibiotic treatments. This occurred in only one patient in this series.
Statistical analysis
To determine the effect of a two-stage operation, the pre-operative and post-operative maximum flexion degree (MFD), maximum extension degree (MED), and knee ROM were compared using paired t-tests. The different HSS scores among pre-operation, interval, and post-operative period were compared using analysis of variance (ANOVA) for repeated measures. All statistical analyses were performed using SPSS software version 19.0 (SPSS Inc., Chicago, IL), and the statistical figures were prepared using GraphPad Prism version 5.00 for Windows (GraphPad Software, San Diego CA). The level of significance was set at p<0.05.
Results
Infection was controlled successfully in 16 patients by using a two-stage method for primary TKA. C-reactive protein returned to normal level in an average of 3.4 wks (range, 1–7 wks), whereas ESR recovered in an average of 11.4 wks (range, 6–19 wks). The average interval time between two-stage operations was 16.8 wks (range, 10–27 wks). The pre-operative information is shown in Table 1. The mean HSS score in the interval time was 66.8 (range, 56–75) before the second stage surgery. The average range of post-operative knee motion was 1.6 degrees (range, 0–5 degrees) to 107.5 degrees (range, 95–125 degrees) and the mean post-ROM was 105.9 degrees (range, 90–125 degrees). The average HSS score was 83.9 (range, 77–91) at the latest follow-up of 8 y (average, 3.8 y; range, 2–8 y; Fig. 4, Tables 1 and 2). Compared with the pre-operative level, the mean HSS score increased after both the first-stage and second-stage surgery (p<0.05). The post-operative maximum extension degree was smaller and the maximum flexion and range of motion degree were larger than pre-operative degree (all p<0.05). There were no recurrent infections and no patients lost to follow-up.

Comparison results. (
Post-recover time of CRP: The time when CRP returned to normal after first-stage surgery.
Post-recover time of ESR: The time when ESR were below twice value of the high threshold after first-stage surgery.
Post-ROM and Post-HSS score were assessed at the latest follow-up.
Interval-HSS was assessed before the second stage surgery.
Patient 6 had no post-operative result because underwent arthrodesis for uncontrolled infection.
CRP=C-reactive protein; ESR=erythrocyte sedimentation rate; ROM=range of motion; HSS=Hospital for Special Surgery Knee score.
Only one patient accepted arthrodesis for uncontrolled infection after undergoing debridement twice and a continuous systemic antibiotic treatment. His CRP and ESR remained at a high level for 3 wks after debridement with acute inflammatory performance, therefore, a debridement and spacer block insertion was taken again at 22 d after the first surgery. However, infection was still not controlled after 4 wks follow-up. The patient finally elected to have arthrodesis instead. The results of the arthrodesis was acceptable for obvious pain relief and no recurrent infection.
Discussion
Epidemiologic studies have shown that infectious arthritis of the knee accounts for approximately 40%–50% of all infected arthritis [6]. Uncontrolled knee infection could lead to continuous intra-articular damage and usually causes undesirable results such as bone loss, contracture, osteomyelitis, and osteoporosis, which were unfavorable to subsequent treatment. The traditional treatment of infectious arthritis of the knee includes decompression, debridement, irrigation, and systemic antibiotics. The methods for decompression, debridement, and irrigation consist of arthroscopy and arthrotomy, but the optimum method remains to be determined [1,5]. Wirtz et al. [7] compared the results of septic arthritis of the knee treated by arthroscopic debridement and arthrotomy and found arthrotomy to be superior in patients with symptoms of infection for more than 5 d and bone destruction. Total knee arthroplasty and arthrodesis could be performed after controlling infection in patients with degenerative arthritis or obvious joint damage.
Severe arthritis with infection has limited therapeutic alternatives, among which arthrodesis is appropriate for patients for whom repeated operations and treatments have failed to control infection because it contributes to complete control of the infection and pain alleviation. However, arthrodesis may cause some complications, such as non-union, malunion, recurrent infection, and knee dysfunction, and may increase the difficulty of later joint reconstruction [8–10]. Amputation is also an option for patients with uncontrolled infection because it removes the infectious tissues, but it will leave serious functional defects. In general, primary TKA is only recommended until the infections are completely controlled [10–12].
Two-stage revision TKA has been used widely as the gold standard for peri-prosthetic infection after TKA since first being put forward by Windsor et al. [3] in 1990. Many studies reported that the control rate of infection reached more than 90% in patients with two-stage revision treatment [13–15]. Gooding et al. [16] reported that a control rate of 98% in chronically infected TKA was achieved with the application of a prosthesis with antibiotic-loaded acrylic cement (PROSTALAC) functional spacer. Qiu et al. [17] treated 10 patients who had serious infection after TKA with two-stage revision treatment and achieved success in all cases. Furthermore, the two-stage revision treatment can also be applied to other infections. Wang et al. [18] conducted research on the clinical efficacy of spacer block loaded with antibiotic cement on osteomyelitis with non-union after intra-medullary fixation. Twelve patients with chronic osteomyelitis and non-union of bone caused by intra-medullary nailing were treated. An antibiotic-impregnated spacer was inserted after removal of the biomembrane and internal fixator, thorough debridement, and irrigation. After controlling osteomyelitis, two-stage bone transplantation and internal fixation were performed after 3 to 6 mo. All healed with no early complications or recurring infection during follow-up. These successful cases suggest that the two-stage TKA may also be applied in severe osteoarthritis with infection. Kirpalani et al. [19] applied two-stage TKA in five patients with diabetes mellitus with non-salvageable septic arthritis and reported no recurrence of infection after a follow-up of 38 mo with an HSS score of 83 points. Nazarian et al. [1] treated 14 cases of chronic knee pyogenic arthritis and degeneration with the same method. At 4.5 y post-operation, no infection or prosthetic loosening was observed. The KSS score improved from 46 to 89. Shaikh et al. [20] also preformed a two-stage primary TKA using intra-operatively molded articulating cement spacers in 15 patients with infected arthritic knees and had encouraging results. No patients had recurrent infection after TKA.
For severe knee osteoarthritis combined with infection, open incision is conducive to thorough debridement and irrigation. Infected synovial lesions and necrotic tissue should be removed as much as possible, especially in the posterior aspect of the knee where pathogens can accumulate and grow. Antibiotic-loaded bone cement spacer blocks provide effective local antibiotic concentration and maintain the soft-tissue tension as well as some joint functions in the knee.
In our study, the spacer block was shaped in a well-designed mold that we created which provided maximum coverage of bone ends and retained the basic prosthesis shape and the fundamental function of the knee. After the first-stage operation using this type of spacer block, the average HSS score increased substantially compared with the pre-operative level, meaning the patients' quality of life improved. It is interesting that three of the patients were fully comfortable with the well-designed spacer because no obvious difficulty and pain existed in their daily life. They did not believe further joint replacement surgery was necessary (Table 1).
Intravenous antibiotics were usually used for 6 wks after the first-stage debridement of two-stage revision TKA [5]. Nazarian et al. [1] used a two-stage primary TKA for infected osteoarthritis, and also used intravenous antibiotics for 6 wks after the first-stage operation. However, intravenous antibiotics were used only for 1 wk in our study and the results were also encouraging. Thus, in our experience, thorough debridement may be more important and more effective for infection eradication, and the efficacy of the long-time use of intravenous antibiotics is still controversial.
Eleven of the 17 patients in our study were infected after a previous operation to treat their knee osteoarthritis, including knee injection and arthroscopy. Moseley et al. [21] and Kirkley et al. [22] reported that arthroscopy did not have a substantial effect on osteoarthritis. On the basis of the new American Academy of Orothopaedic Surgeons guidelines, the use of intra-articular corticosteroids and hyaluronic acid are not recommended because their effects are not clear. Therefore, with its efficacy remaining dubious and the risk of infection, we believe that application of intra-capsular injection and arthroscopy for osteoarthritis should be limited.
According to bacteriology, more than 50% of peri-prosthetic infections reported have been caused by staphylococcus after a TKA. Staphylococcus aureus and S. epidermidis were the main pathogens in the early stages after the surgery (within 3 mo); pathogens such as coagulase-negative Staphylococcus, Streptococcus, Enterococcus, and Anaerobion were more common in the subsequent stages [23]. Similarly in infectious osteoarthritis, Staphylococcus was still considered the most common cause of infection followed by Streptococcus and Enterococcus. Interestingly, it is reported that approximately 46.5% of the S. aureus cases in TKA peri-prosthetic infections were methicillin-resistant S. aureus (MRSA) [24], whereas 41.7% of S. aureus cases were MRSA in infectious osteoarthritis [25]. Although it is difficult to draw a conclusion on the bacteriology of infectious osteoarthritis from our small sample size, we found that seven of the 17 cases analyzed were caused by Staphylococcus, which is consistent with the study mentioned above. Overall, according to current studies, Staphylococcus is the main cause for both peri-prosthetic infection and infectious osteoarthritis, and many of the species of pathogens are similar. However, the proportion of MRSA seems somewhat greater in the S. aureus cases of peri-prosthetic infections after TKA compared with those cases of infectious osteoarthritis. However, larger sample-size comparative studies are needed to verify these results.
Although this research is not the first report of these types of cases, only a few similar studies have been reported previously [1,19,20] and there are some differences in the protocol. We used a well-designed bone cement spacer block, which improved patients' quality of life during the interval time. We also took a different strategy of using intravenous antibiotics, which shortened the antibiotics application time. This is the first report of its kind of case from China that is focused primarily on Asians, specifically Chinese. Thus, it should be a good complement to prior research that is focused primarily on Caucasians [1,19].
Primary TKA is the optimum treatment for severe osteoarthritis. Infectious osteoarthritic patients often lose the chance to have TKA because of uncontrolled infection. In our study, 16 of 17 infectious osteoarthritic patients showed encouraging results through a two-stage TKA. Open debridement and a well-designed antibiotic-laden bone cement spacer block was taken at the first stage, and TKA was performed at the second stage. The second-stage procedure also followed the protocol of primary TKA. The post-operative function and satisfaction assessment of the 16 patients were high with no recurrent infection, loosening, or revision required. The success of this treatment method suggests that it should be a reliable alternative for the infected osteoarthritic knee.
Footnotes
Author Disclosure Statement
No competing financial interests exist.