
Abstract
Abstract
Background:
The optimal duration of antimicrobial prophylaxis (AMP) in patients undergoing gastric cancer surgery remains debatable. The aim of this prospective cohort study was to evaluate the feasibility of intraoperative AMP in comparison with conventional AMP in patients undergoing elective open gastrectomy.
Methods:
The duration of AMP was shortened in two six-monthly stages in patients undergoing open gastrectomy for gastric cancer, and the incidences of surgical site infections (SSIs) and remote infections (RIs) were surveyed. In the first stage (September 2004 to February 2005), the patients received four intravenous injections of cefazolin 1 g at 12-h intervals starting from 30 min before surgery (conventional AMP). In the second stage (March 2005 to August 2005), the patients received the same agent at three-h intervals starting 30 min before surgery and continuing until the end of the operation (intraoperative AMP).
Results:
A total of 423 patients were enrolled, including 202 patients operated on in the first stage of cancer and 221 patients operated on in the second stage. The patient characteristics in the two stages were well balanced. There was no significant difference in the incidence of SSIs (10.4% vs. 8.1%; odds ratio [OR], 0.764; 95% confidence interval [CI] 0.395–1.480; p = 0.528) or RIs (7.9% vs. 5.9%; OR 0.727; 95% CI 0.340–1.551; p = 0.525) between the two stages. There were no serious adverse events related to the AMP. The treatment effects on the SSIs were similar in all subgroups of patients analyzed. There was no appreciable difference in the trend in the causative pathogens of the SSIs and RIs between the two stages.
Conclusions:
Intraoperative and conventional AMP were associated with similar incidences of SSIs and RIs. Intraoperative AMP appears to be feasible and sufficient in patients undergoing open gastrectomy for gastric cancer.
S
Despite this guideline recommendation, conventional AMP is still adopted in surgical practices, especially in Japan [8–10]. Conventional AMP is not only more expensive and carries the risk of an outbreak of multidrug-resistant bacteria [11,12] but may increase the risk of SSIs [13]. However, there is insufficient evidence to support the appropriateness of intraoperative AMP in gastric cancer surgery, especially in Eastern Asia, where extended lymphadenectomy is performed routinely [14].
The aim of this study was to evaluate prospectively the feasibility of intraoperative AMP as recommended by the U.S. Centers for Disease Control and Prevention (CDC) guideline in comparison with conventional AMP in patients undergoing open gastrectomy for gastric cancer. The surgical procedures and perioperative patient care protocols were uniform and carried out by the same surgical team through the study period. The incidences of SSIs and remote infections (RIs) were analyzed.
Patients and Methods
Patients
We conducted this single-institutional, open-label, prospective cohort study between September 2004 and August 2005. The study was approved by the Institutional Review Board. Patients scheduled to undergo elective open gastrectomy with ≥D1 lymphadenectomy for histologically proved gastric cancer were enrolled consecutively. Patients undergoing laparoscopic procedures or concomitant pancreatoduodenectomy, those with an allergy to penicillin, and those with active infectious or malignant diseases were excluded.
AMP procedure
The duration of AMP was shortened in two six-monthly stages. In the first stage (September 2004 to February 2005), the patients received a total of four intravenous injections of cefazolin (Otsuka CEZ injection Mc; Otsuka, Tokyo, Japan) 1 g at 12-h intervals starting 30 min before the surgery until the evening of post-operative day 1 regardless of the operation time (conventional AMP). In the second stage (March 2005 to August 2005), the patients received the same agent at 3-h interval(s) starting 30 min before surgery and continuing only until the end of the operation. If the operation was completed within 3 h of the initial administration of cefazolin, no additional dose was given (intraoperative AMP).
Collection and description of data
Data on various patient characteristics and operative details potentially associated with the risk of SSIs [7], including age, gender, American Society of Anesthesiology (ASA) score, body mass index, serum albumin concentration, presence/absence of diabetes mellitus, presence/absence of a smoking history, presence/absence of neoadjuvant chemotherapy, presence/absence of perioperative blood transfusion, depth of tumor invasion, type of gastrectomy, presence/absence of concomitant splenectomy or splenopancreatectomy, extent of lymphadenectomy, residual tumor status, operation time, and intraoperative blood loss in the two groups were recorded. The incidences and causative pathogens of the SSIs and RIs and the length of the post-operative hospital stay were compared between stages.
The depth of tumor invasion was described according to the International Union Against Cancer (UICC) TNM staging system [15], and the extent of lymphadenectomy was chosen according to the Japanese gastric cancer treatment guidelines [14]. The definition of SSI was based on the National Nosocomial Infection Surveillance system of the CDC [7]. With respect to RIs, only those corresponding to ≥grade II of the Clavien-Dindo classification [16] were considered for the analysis.
Surgical procedure and perioperative patient care
Perioperative patient care, except for the AMP, was provided uniformly during the entire study period on the basis of a standardized clinical pathway. The patients were admitted to the hospital two or three days before surgery. All patients were asked to shower with hot water on the day before the operation. Hair was not removed at the site of the procedure. A peripheral venous catheter was inserted on the evening before the operation, which was changed once every three days thereafter. In the operating room, the skin was painted with 10% povidone–iodine solution and draped with a disposable towel. A urinary catheter was inserted immediately before the operation.
All the operations were performed by experienced surgeons who followed a uniform procedure in a standard aseptic manner. For total and distal gastrectomy, the Roux-en-Y anastomosis was chosen. For pylorus-preserving gastrectomy, a gastro-gastric anastomosis was employed [17]. For proximal gastrectomy, reconstruction with jejunal interposition was adopted [18]. All gastrectomies included at least one hand-sewn anastomosis. At the end of the operation, the abdominal cavity was washed with 3 L of saline, and one or two drains with a closed drainage system were placed through a stab incision(s) separate from the laparotomy incision. The fascia was closed by continuous suture with absorbable monofilament, and the skin was closed with stainless steel staples.
Post-operatively, the laparotomy site was covered with sterile gauze for 48 h and then left open. When the post-operative clinical course was uneventful, oral intake was resumed on post-operative day 3, the urinary catheter was removed on day 3, the drains were removed on day 3 or 4, the venous catheter on day 6, and the staples on day 7 or 8. The incisions were inspected twice daily until discharge, followed by inspection at the outpatient clinic until day 30. In cases with suspected SSI or RI, samples of pus were obtained if possible and cultured for aerobic and anaerobic bacteria to identify the causative pathogens. Pancreatic fistula, anastomotic leakage, and intra-abdominal abscess were diagnosed by a contrast swallow study, computed tomography, fistulography, or some combination thereof.
Statistical analysis
The IBM SPSS Statistics 20.0 program (IBM, Corp., Armonk, NY, USA) was used for the statistical analyses. The χ2 test was applied for comparisons of the nominal variables and the Student t-test or Mann-Whitney U test for comparisons of the continuous variables. Eleven subgroups were analyzed by logistic regression to assess the statistical interactions between various patient characteristics and the treatment effects on the SSIs. P values of <0.05 were considered to indicate significant differences.
Results
Patient characteristics and operative details
During the study period, 566 patients underwent surgery for gastric cancer. Of these, 423 eligible patients, including 202 patients operated on in the first stage and 221 patients operated on in the second stage, were enrolled. All the enrolled patients underwent open gastrectomy with ≥D1 lymphadenectomy as previously scheduled.
The patient characteristics and operative details in the two stages were well balanced (Table 1). More than 90% (n = 381) of the patients had an American Society of Anethesiologists score of 1 or 2, a serum albumin concentration of >3.5 g/dL, no history of neoajuvant chemotherapy, no blood transfusion, and R0 resection. The mean body weight of the enrolled 423 patients was 60.1 kg. Overweight patients with a body mass index of ≥25 kg/m2 accounted for 22.5% (n = 95) of the enrolled subjects, patients with diabetes mellitus for 16.5% (n = 70), and patients with a smoking history for 54.4% (n = 230). Partial (distal, pylorus-preserving, or proximal) gastrectomy was performed in 70.9% (n = 300) and total gastrectomy in the remaining 123 of the enrolled patients. The median number of AMP doses in the second stage was 1.9 (range 1–3).
AMP = antimicrobial prophylaxis; ASA = American Society of Anesthesiologists.
Incidences of SSIs and RIs
Overall, 39 patients (9.2%) developed SSIs (Table 2). The incidence of SSIs was 10.4% (95% confidence interval [CI] 6.2%–14.6%) in the first stage compared with 8.1% (95% CI 4.5%–11.7%) in the second stage (odds ratio 0.764; 95% CI 0.395–1.480; p = 0.528). In both stages, the SSIs in most cases involved an organ(s) or space(s), being associated frequently with pancreatic fistula formation or anastomotic leakage. There were no cases of deep incisional SSIs, but superficial incisional SSIs were identified in six patients (3.0%) in the first stage and seven patients (3.2%) in the second stage. In the first stage, one patient died during hospitalization secondary to duodenal stump leakage necessitating emergency surgical intervention. All the other SSIs were treated successfully by surgical or radiologic intervention or antibiotic therapy.
Two patients in the second stage had both superficial incisional and organ/space surgical site infections.
Comparisons of the overall incidences.
AMP = antimicrobial prophylaxis.
Overall, 29 patients (6.9%) developed RIs (Table 2). The incidence of RIs was 7.9% (95% CI 4.2%–11.6%) in the first stage compared with 5.9% (95% CI 2.8%–9.0%) in the second stage (OR 0.727; 95% CI 0.340–1.551; p = 0.525). All the RIs were treated successfully by antibiotic administration, physical therapy, catheter removal, or some combination thereof. Six patients in each of the stages had both SSI and RI.
No serious AMP-related adverse events were observed. The median post-operative hospital stay was 12 days, being about the same in the two stages (p = 0.493) (Table 2).
Subgroup analysis
The treatment effects on the SSIs were similar in all the subgroups; there were no statistically significant interactions between the treatment effects and the patient characteristics, including the body mass index (<25 kg/m2/≥25 kg/m2), presence/absence of diabetes mellitus, presence/absence of a smoking history, and type of gastrectomy (total/partial) (Fig. 1). The treatment effects on the SSIs also were similar among the patients who underwent partial gastrectomy; the ORs for SSIs with intraoperative AMP in patients who underwent proximal gastrectomy, distal gastrectomy, and pylorus-preserving gastrectomy were 1.444 (95% CI 0.080–26.230), 0.306 (95% CI 0.058–1.623), and 0.732 (95% CI 0.118–4.559), respectively.
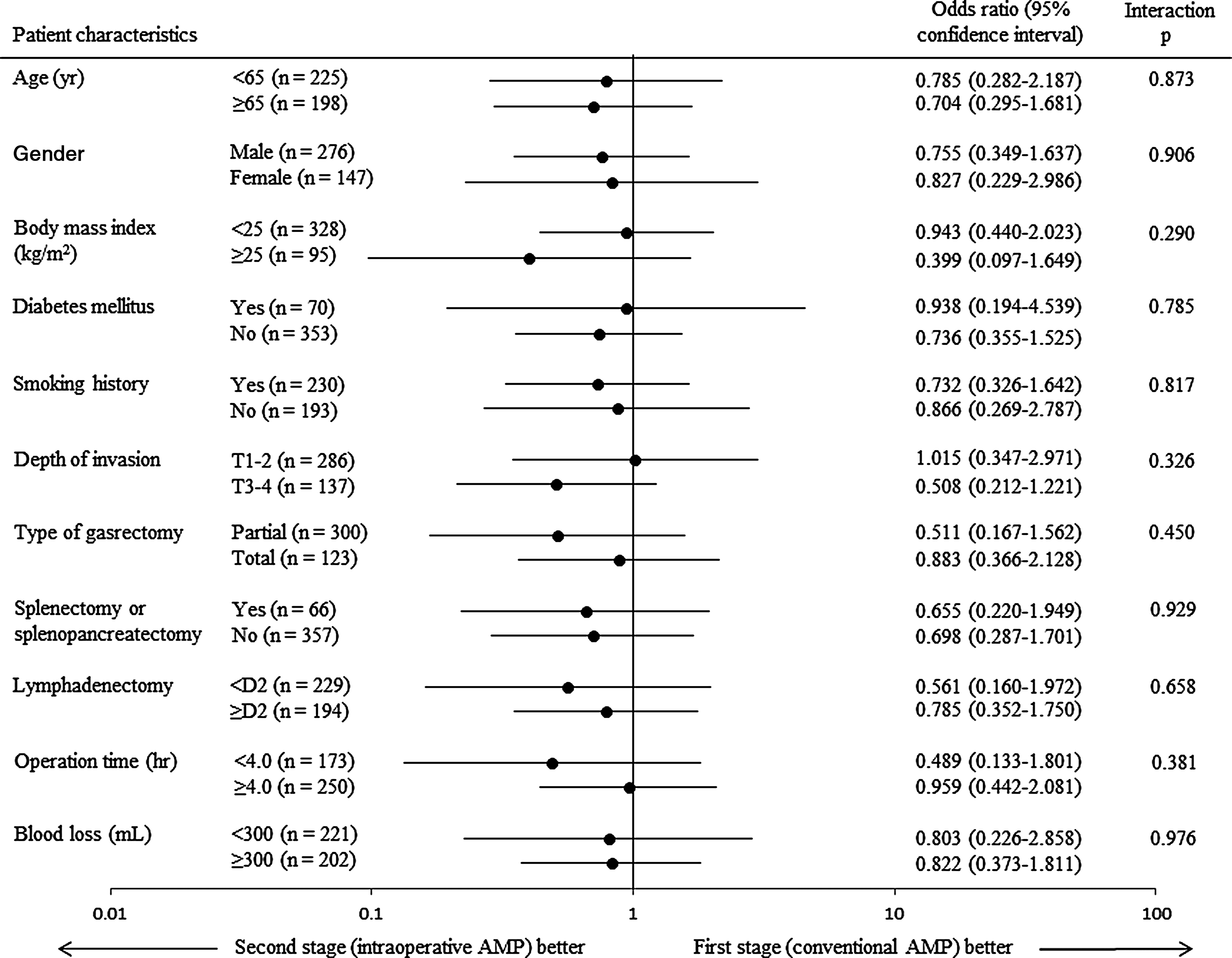
Forest plot of subgroup analyses. P values for interactions and odds ratios for surgical site infections with intraoperative antimicrobial prophylaxis (AMP).
Pathogens isolated from sites of SSIs and RIs
The pathogens initially isolated from the sites of the SSIs are shown in Table 3. Among the 39 patients with SSIs, no pathogens could be identified in six patients in the first stage and five patients in the second stage. Multiple pathogens were isolated in six patients in each of the two stages. The pathogens most commonly isolated were Staphylococcus spp. and Streptococcus spp., followed by Haemophilus spp., Enterococcus faecalis, and others, in that order. No multidrug-resistant strains were found in either stage.
AMP = antimicrobial prophylaxis.
The pathogens initially isolated from the sites of the RIs are shown in Table 4. No pathogens could be identified in seven patients in the first stage and three patients in the second stage. The pathogen most commonly isolated was Staphylococcus spp. Again, no multidrug-resistant strains were found in either stage.
AMP = antimicrobial prophylaxis.
During the entire study period, no clinically apparent episodes of bacterial transmission among patients were encountered that resulted in multiple simultaneous infections caused by a particular pathogen.
Discussion
In this study, intraoperative and conventional AMP were associated with similar incidences of SSIs. Intraoperative AMP thus appears to be feasible and sufficient in patients undergoing open gastrectomy for gastric cancer.
The recently revised guidelines for AMP recommend the intraoperative use of cefazolin 2 g (3 g for patients weighing ≥120 kg) at 4 h interval(s) during gastroduodenal procedures [19]. In Japan, the standard therapeutic dose of cefazolin is 1 g, which has been associated with acceptable incidences of SSIs in patients with gastric cancer [20–22]. Cefazolin 1 g might be sufficient for SSI prevention in most Japanese patients, as they are, on average, lighter than their Western counterparts. It is obvious, however, that the use of a greater dosage (>1 g) should be considered for overweight Japanese patients.
In Japan, a multi-institutional randomized controlled trial recently demonstrated the non-inferiority of intraoperative AMP to conventional AMP (until post-operative day 2) in terms of SSI prevention in patients undergoing distal gastrectomy for gastric cancer [20]. A similar result was shown in a single-institutional randomized study carried out in patients undergoing partial or total gastrectomy [21]. Cefazolin was used exclusively in the two studies. An earlier multi-institutional randomized controlled trial using cefazolin and ampicillin-sulbactam also showed an equivalent effect of single- and multiple-dose (until post-operative day 3) antibiotic administration in preventing SSIs in patients undergoing elective gastric cancer surgery [22]. Our findings are consistent with these reports.
The overall incidence of SSIs in the present study was comparable to those reported from previous studies [20–22]. Most of the SSIs involved an organ(s) or space(s), also consistent with previous reports [13,20]. However, these organ/space SSIs could be associated with the quality and invasiveness of the surgery itself. Meticulous procedures, especially during supra-pancreatic lymph node dissection and the anastomoses, might be essential to minimize the risk of such SSIs. Our results suggest that intraoperative and conventional AMP have similar effects on the prevention of both superficial incisional and organ/space SSIs.
The traditionally longer use of AMP by Japanese surgeons could be attributed partly to their belief, albeit not based on sufficient evidence, that it can minimize the risk of all post-operative infections, including SSIs and RIs. Our study showed that the incidence not only of SSIs, but also of RIs, was similar after intraoperative and conventional AMP. In all of the patients except one who received conventional AMP, the SSIs and RIs were treated successfully, suggesting that extended AMP offers little additional benefit in controlling such infections. Our study also suggested that more careful surveillance is required in patients with SSIs, in view of the greater risk of concurrent RIs.
All of the causative pathogens isolated from the SSIs and RIs were components of the normal flora of the intestinal tract, oral cavity, respiratory tract, or skin. The causative pathogens most commonly isolated were Staphylococcus spp. and enteric bacteria, as previously reported [22,23]. Despite the small sample, there was no appreciable difference in the bacteriological trend between the two stages in the present study. Notably, no multidrug-resistant strains were isolated in either stage. Thus, even administration of as many as four antimicrobial doses until the evening of post-operative day 1 appeared to be associated with little risk of an outbreak of such strains.
We traditionally admit patients to the hospital two or three days before the operation for pre-operative orientation and preparation, including endoscopic tumor border marking. However, a prolonged pre-operative hospital stay has been suggested as a factor in a greater risk of SSIs [2,7]. Thus, minimizing the pre-operative hospital stay might decrease further the incidence of SSIs observed in the present study.
Povidone–iodine is the antiseptic agent most commonly used for pre-operative skin preparation in Japan. However, recent Western studies have suggested that the skin preparation agent affects the incidence of incisional SSIs in patients undergoing general surgery [24–26]. Assessing the comparative effects of povidone–iodine and other agents, including chlorhexidine gluconate and alcohol-containing products, on the risk of SSIs in Japanese patients may be a future task.
The limitations of this study include its non-randomized design and the possibility of bacterial transmission [27] among the patients in each treatment stage. However, the patient characteristics in the two stages were well balanced, and there were no apparent episodes of bacterial transmission among the patients during the entire study period. The subgroup analysis showed that there were no detectable confounders significantly biasing the study results. In addition, single-institutional studies such as ours can offer homogeneity among subjects in respect to the perioperative care and surgical procedures, factors that exert a potent influence on the incidence of SSIs [7]. Thus, the results of the present study, together with those of previously controlled randomized trials [20–22], strongly support the efficacy and feasibility of intraoperative AMP and discourage the routine continuation of AMP into postoperative day 1, 2, or 3 in patients undergoing surgery for gastric cancer.
Footnotes
Author Disclosure Statement
No competing financial interests exist for any of the authors.