
Abstract
Abstract
Background:
Rhabdomyolysis has multiple etiologies with unclear mechanisms; however, rhabdomyolysis caused by Staphylococcus aureus infection is rare.
Case Report:
A case report of severe rhabdomyolysis in a patient who presented with endocarditis caused by methicillin-susceptible S. aureus and review of relevant literature.
Results:
The patient had a history of cardiac surgery for tetralogy of Fallot. He was admitted to the hospital because of fever and digestive symptoms. Respiratory and hemodynamic status deteriorated rapidly, leading to admission to the intensive care unit (ICU) for mechanical ventilation and vasopressor support. Laboratory tests disclosed severe rhabdomyolysis with a serum concentration of creatine kinase that peaked at 49,068 IU/L; all blood cultures grew methicillin-susceptible S. aureus. Antibiotic therapy was amoxicillin-clavulanic acid, ciprofloxacin, and gentamicin initially and was changed subsequently to oxacillin, clindamycin, and gentamicin. Transesophageal echocardiography showed vegetation on the pulmonary valve, thus confirming the diagnosis of acute endocarditis. Viral testing and computed tomography (CT) scan ruled out any obvious alternative etiology for rhabdomyolysis. Bacterial analysis did not reveal any specificity of the staphylococcal strain. The patient improved with antibiotics and was discharged from the ICU on day 26. He underwent redux surgery for valve replacement on day 53.
Conclusions:
Staphylococcal endocarditis should be suspected in cases of severe unexplained rhabdomyolysis with acute infectious symptoms.
R
Case Report
A 23-year-old patient was admitted to the hospital for severe fatigue, high fever (39°C), and digestive symptoms for 24 h. He had a tetralogy of Fallot corrected surgically when he was four years old. Stenosis of the right ventricular outflow tract occurred in 2008 and required insertion of a Freestyle® prosthesis (Medtronic, Minneapolis, MN) and of a Melody® valve (Medtronic) in 2012 because of persistent substantial obstruction of right ventricular ejection. Medical treatment was limited to acetylsalicylic acid. Upon admission, clinical examination revealed a marked hyperthermia (39.3°C), blood pressure of 110/80 mm Hg with tachycardia (140 beats/min), and mottling of the lower limbs without myalgia or arthralgia. No obvious source of infection was found. Urine was brown, suggesting a myoglobinuria. Chest radiograph showed cardiomegaly without lung infiltrate. The initial laboratory tests revealed increased aspartate aminotransferase (AST; 520 IU/L), alanine aminotransferase (ALAT; 120 IU/L), creatine kinase (43,968 IU/L), and C-reactive protein (CRP; 240 mg/L) without hyperleukocytosis (4,720/mm3), hyperlactatemia (3.52 mmol/L), and a severe thrombocytopenia (40,000/mm3). Transthoracic echocardiography depicted chronic cor pulmonale and preserved left ventricular function (ejection fraction: 59%) without evidence of valvular vegetations. Transesophageal echocardiography did not show findings consistent with endocarditis. After complete microbiologic documentation and sepsis with digestive origin being suspected, treatment with intravenous amoxicillin-clavulanic acid, ciprofloxacin, and gentamicin was initiated.
Respiratory and hemodynamic status deteriorated rapidly leading to intubation, mechanical ventilation, and vasopressor support (norepinephrine: 4 mg/h maximal rate). Laboratory tests confirmed worsening of the rhabdomyolysis with a creatine kinase concentration that peaked at 49,068 IU/L two days after admission. Creatine kinase concentration decreased rapidly between day two and day four and increased again on day five; this new peak concomitant with a macular rash located on the anterior side of the knees, chest, and ankles (Fig. 1). All blood cultures grew methicillin-susceptible S. aureus (MSSA). Accordingly, antibiotic therapy was changed to intravenous oxacillin (12 g/d), clindamycin (1,800 mg/d), and gentamicin (240 mg/d). Despite adequate fluid resuscitation and alkalinization, renal function deteriorated rapidly and intermittent hemodialysis was required for a total of 12 sessions. Noradrenaline was discontinued eight days after admission.
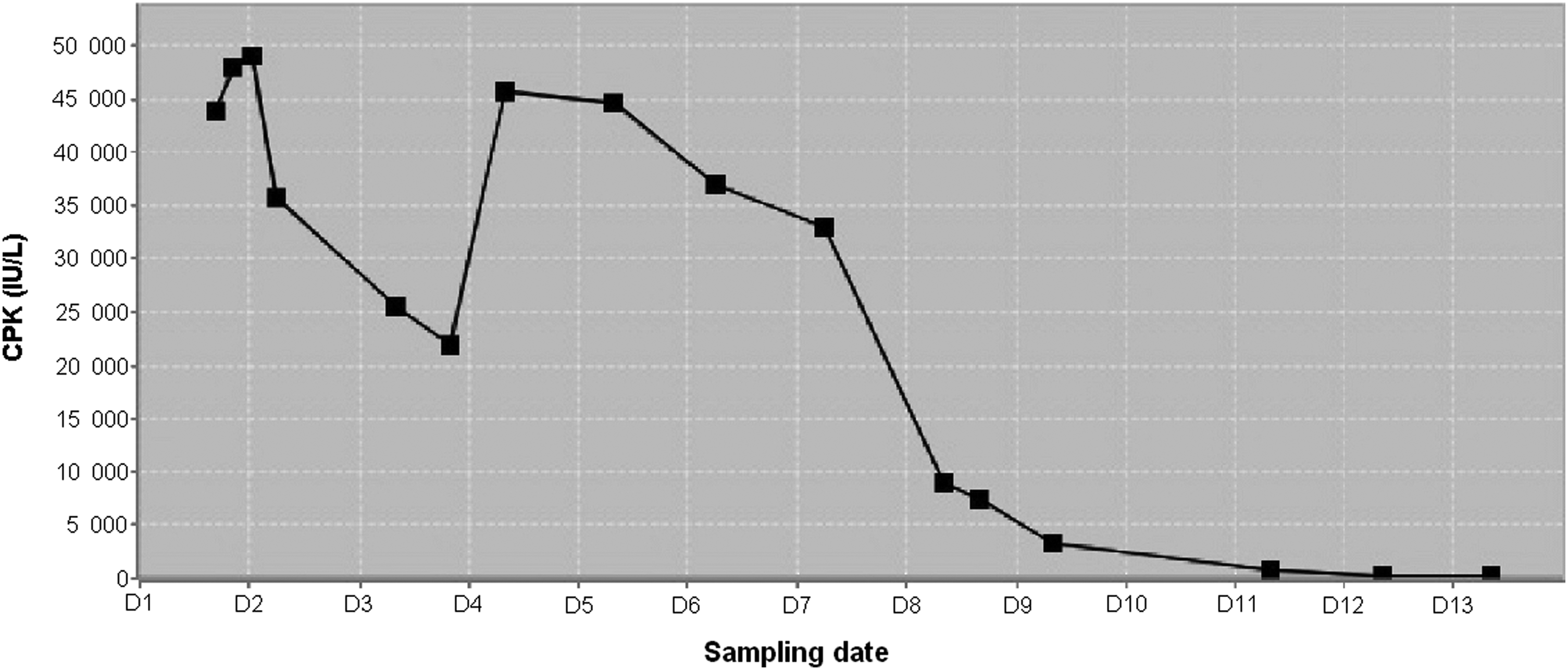
Circulating creatine kinase (CPK) concentrations during the patient's hospitalization.
Clinical examination did not reveal any abscess, suppurative myositis, or septic embolism and chest and abdominal CT scan was normal. Toxic shock syndrome (TSS) was ruled out because the TSST-1 gene was not harbored by the isolate. The other main virulence factors, i.e., enterotoxins, exfoliative toxins, and Panton-Valentine leukocidin were also absent. The typing of the strain by the French Reference Center for Staphylococci in Lyon revealed a MSSA CC15 strain. The complete and extensive viral evaluation was negative or disclosed old immunization.
Despite improvement, 10 days after admission, there were still clinical and biologic signs of possible ongoing infection. A repeated transthoracic echocardiography finally revealed a large and mobile vegetation (17 × 15 mm) of the Melody valve resulting in an elevated intra-stent pressure gradient. This confirmed the clinically suspected acute infective endocarditis. Antibiotic therapy was then modified; clindamycin was replaced by rifampicin. The patient was extubated on day 12 and discharged from the ICU on day 25.
Because fever and biologic markers of inflammation persisted and given the elevated intra-stent pressure gradient, the patient underwent planned redux surgery on day 53. The Melody valve was removed and replaced by a homograft. Post-operative course was unremarkable and the patient was discharged home three months after surgery without any infectious complication.
Discussion
Severe rhabdomyolysis is a life-threatening condition that can induce severe hyperkalemia, acute renal failure resulting from hypovolemia and the precipitation of myoglobin in the tubules, acute disseminated intravascular coagulation (DIC), and severe hydroelectrolytic disorders [1], characterized by biologic signs but also by clinical symptoms such as myalgia. In our patient, rhabdomyolysis was defined only biologically because there was no evidence of clinical signs despite repeated and careful physical examination.
Rhabdomyolysis is a rare complication of bacterial infections. It is mainly caused by gram-positive lung infections, especially those caused by Streptococcus spp. Gram-negative bacteria are identified rarely as causative micro-organisms [3,5,11]. Only isolated cases reported Staphylococcus spp. as a source of severe rhabdomyolysis, as in our case, but they were often poorly documented. Rhabdomyolysis has been described mainly in the setting of staphylococcal TSS. In this particular case, it resulted from exposure to super-antigenic exotoxins promoting the production and release of pro-inflammatory cytokines [12]. Staphylococcal TSS is characterized clinically by scattered maculopapular exanthema inducing a desquamation one or two weeks later and characterized biologically by the presence of an exotoxin TSST-1 produced by S. aureus that was not found in our patient.
Rhabdomyolysis mechanisms during bacterial sepsis are unclear. It is well known that some micro-organisms result in muscle injuries through direct bacterial invasion, whereas others produce myotoxins (e.g., Clostridium spp.) or toxins with similar effects (Streptococcus spp. and Staphylococcus spp. pyrogenic toxin A) [13]. Other micro-organisms secrete several well-known enzymes such as cytolysin that may damage the cell membrane directly. Several authors also demonstrated the role played by endotoxins and other mediators such as interleukin-1 or tumor necrosis factor-α in the muscle damage occurring during sepsis [14]. The role of endotoxins presumably can explain the severe muscle loss observed commonly in prolonged sepsis. However, it cannot account for the sudden occurrence of rhabdomyolysis during bacterial sepsis, as in our case, unless the involved micro-organisms have specific toxic properties. Some rare cases similar to ours have been published previously, but mainly in the pediatric literature [8,15,16]. Three cases of rhabdomyolysis associated with an S. aureus infection have been reported in children without TSS. Adamski et al. [15] described the case of a 15-y-old boy with suppurative myositis and a rhabdomyolysis with a maximal circulating concentration of creatine kinase of 33,400 IU/L. Saül et al. [16] reported the case of a 13-y-old girl with unexplained rhabdomyolysis and with a maximum creatine kinase concentration of 59,729 IU/L. This patient did not exhibit any signs of TSS or bacteremia but Staphylococcus was isolated in her urine [16]. Bandi et al. [8] described the case of a 12-y-old boy with rhabdomyolysis associated with S. aureus endocarditis and a circulating creatine kinase peak of 12,156 IU/L. To our knowledge, only one case of rhabdomyolysis of mild intensity (circulating creatine kinase peak of 990 IU/L) was reported in a 20-y-old man with a S. aureus endocarditis [7]. In conclusion, S. aureus acute endocarditis can be suspected in the presence of severe unexplained rhabdomyolysis associated with acute infectious symptoms.
Footnotes
Acknowledgments
Written informed consent was obtained from the patient for publication of this case report and of the associated images. A copy of the written consent is available for review from the editor of this journal. This work was performed at the University hospital of Limoges, France. We thank Sarah Demai who provided medical writing services.
Author contributions were as follows: C.R. and B.F. cared for the patient and drafted the manuscript. A.L.F., M.D., P.V., E.D., and O.B. analyzed the data and revised the manuscript. C.E. cared for the patient and revised the manuscript. All authors read and approved the final manuscript.
Author Disclosure Statement
No competing financial interest exist.