
Abstract
Abstract
Background:
The aim of this study was to compare the prosthetic joint infection (PJI) rate after knee revision arthroplasty in two consecutive periods with different antibiotic prophylaxis: short (one day) versus long (five days).
Methods:
From January 2007 to September 2010 antibiotic prophylaxis consisted of 800 mg of teicoplanin and 2 g of ceftazidime intravenously and 1 g of ceftazidime two hours after the first dose. From October 2010, it was prolonged post-operatively using vancomycin and ceftazidime intravenously until the fifth day.
Results:
During the study period, 341 revision surgeries met the inclusion criteria. The PJI rate was lower in the long-prophylaxis group (2.2% versus 6.9%, p=0.049). Prolonged post-operative antibiotic treatment was the only variable associated independently with a lower rate of PJI (odds ratio [OR]: 0.27, 95% confidence interval [CI]: 0.07–0.99).
T
Patients and Methods
All patients who underwent revision total knee arthroplasty between January 2007 and February 2013 were reviewed retrospectively. For this study, only patients who met the pre-operative criteria of aseptic loosening were reviewed. The criteria for aseptic loosening were: local pain, radiologic signs of loosening, and the absence of inflammatory symptoms or signs of infection including fever, local redness, erythema, or fistulae. In all cases C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were used as screening for infection, and when abnormal (CRP ≥1.3 mg/L or ESR >30 mm/h), a bone scan, 99mTc-hexamethylpropyleneamine oxime leukocyte scan, and culture of synovial fluid obtained by sterile aspiration were performed to rule out infection. Only those revision surgeries in which tibial and/or femoral component was exchanged were included; there were 78 cases in which only polyethylene or patella were replaced, therefore, these were excluded from the study.
From January 2007 to September 2010 antibiotic prophylaxis consisted of one intravenous dose of 800 mg of teicoplanin (instead of vancomycin because it can be infused in 10–20 min without risk of red-man syndrome), and 2 g of ceftazidime during induction of anesthesia and 1 g of ceftazidime two hours after the first dose. From October 2010, patients received the same prophylaxis during induction of anesthesia (teicoplanin and ceftazidime), but it was decided to prolong the administration of antibiotics using vancomycin 1 g/12 h and ceftazidime 2 g/8 h intravenously until the fifth post-operative day. Thus, we defined two groups of patients according to the type of antibiotic prophylaxis: one group of patients who received antibiotic prophylaxis for one day (short-prophylaxis group) and one group of patients who received antibiotic prophylaxis for five days (long-prophylaxis group). The Ethical Committee of our institution approved the study.
Throughout both periods, there were no variations in the pre-operative washing protocol, skin preparation, hand hygiene solutions, surgical team, surgical techniques, use of cement loaded with gentamicin for implant fixation, or operating rooms. The revision arthroplasties were performed in a non-laminar airflow operating room. The operation was performed under limb ischemia with the patient in the supine position and used previous incisions whenever possible. In case of difficulty removing the implant, an osteotomy of anterior tibiae tuberosity was performed. Antibiotic-loaded cement was used for implant fixation as standard for revision knee arthrosplasty. All revision arthroplasties were cemented with Cemex® Genta from Tecres Medical (Verona, Italy) containing the equivalent of 1 g of gentamicin. No tissue grafts were necessary. Drainage tubes were removed within the 48 h post-operative period.
During the operation, six deep samples were submitted to the microbiology laboratory. Synovial fluid was aspirated and 50% inoculated into aerobic and 50% into anaerobic blood culture flasks (BACTEC 9400™, Beckton Dickinson, Franklin Lakes, NJ); solid samples from peri-prosthetic tissue were taken and placed into sterile containers. Each culture was transported, processed, and analyzed using standard procedures. The histology was considered positive for infection when five or more neutrophils per high-power field (×40) in at least five separate microscopic fields were found. The study was performed in paraffin sections and not in frozen sections avoiding histologic technical bias [17]. Culture results were considered false-positive when only one sample was positive; if two or more intra-operative cultures were positive for the same micro-organism these were considered as true-positive. In these cases, patients received a specific antibiotic treatment according to the antibiogram for four weeks.
After being discharged, patients were followed according to our protocol, which includes a first visit two weeks after surgery, a second visit after one month, a third visit after three months, and a final visit at one year. Six patients were excluded from the study because a second surgery not related to infection was necessary within the first 100 d of follow-up. Prosthetic joint infection was defined according to current criteria [18]. All patients with an early PJI returned to the operating room for debridement and six deep samples of synovial fluid or peri-prosthetic tissue were submitted to the microbiology laboratory.
Continuous variables were expressed as mean and standard deviation and compared using the Student t-test. The following variables were also categorized: age (≤70 y or >70 y), body mass index (<35 and ≥35), duration of surgery (<120 min or ≥120 min), and pre-operative American Society of Anesthaesiologist (ASA) classification (ASA 1–2 and ASA 3–4). Categorical variables were expressed as frequencies and percentages and compared using the χ2 test or Fisher exact test when necessary. Kaplan-Meier survival method was used to estimate the cumulative probability of failure because of PJI within the first 100 d after revision surgery according to the duration of antibiotic prophylaxis; the curves were compared using the log-rank test. All variables included in the univariable analysis were also included in a step-wise forward logistic regression model to identify independent variables associated with infection. The calibration of the model was assessed by means of the Hosmer–Lemeshow goodness-of-fit test. Statistical significance was defined as a two-tailed p<0.05. The analysis was performed using SPSS, version 20.0 (SPSS Inc., Chicago, IL).
Results
During the study period, 341 cases met inclusion criteria and were reviewed retrospectively. The mean (standard deviation [SD]) age of patients was 72.1 y (8.4) and 271 (78.1%) were female. The mean (SD) body mass index was 31.6 (5.0), and it was ≥35 in 65 (19.2%). The most frequent comorbidities were hypertension in 229 patients (66%), diabetes mellitus in 49 (14.1%), ischemic heart disease in 38 (11.0%), chronic obstructive pulmonary disease in 43 (12.4%), and chronic renal failure in 13 cases (3.7%). The pre-operative ASA classification was 3–4 in 70 cases (20.2%). The mean (SD) days of hospitalization were 7.4 (3.9). Intra-operative microbiology samples were obtained in all cases; in 91 cases (26.2%) at least one sample was positive, but only 24 (6.9%) were considered true-positive according to the protocol described in the Patients and Methods section. The most frequent micro-organism was coagulase-negative staphylococci in 75 cases (21.6%), Staphylococcus aureus in one case (0.3%), other gram-positive micro-organisms in 13 cases (3.7%), and a gram-negative micro-organism in 6 cases (1.7%).
The incidence of PJI after three months of follow-up was 4.9% (17 cases). The isolated micro-organisms in PJIs according to the type of antibiotic prophylactic regimen are shown in Table 1. Infection was polymicrobial in seven cases (41%) and at least one gram-negative micro-organism was isolated in 11 (65%) cases.
CoNS=coagulase-negative staphylococci.
Table 2 shows the baseline characteristics of patients according to the outcome. Duration of surgery ≥120 min (7.7% versus 2.6%, p=0.029) was associated with a higher risk of PJI. The infection rate was the same in those patients in whom the intra-operative cultures were positive or negative.
PJI=prosthetic joint infection; SD=standard deviation; ASA=American Society of Anesthaesiologists; BMI=body mass index; COPD=chronic obstructive pulmonary diseases; CRP=C-reactive protein; IOC=intra-operative culture; CoNS=coagulase-negative staphylococci.
Two hundred and three (59.5%) patients received a short antibiotic prophylaxis regimen whereas 138 (40.5%) received a long antibiotic regimen. Baseline characteristics of patients according to each group are shown in Table 3. Mean age (years) was higher in the long-prophylaxis group (73.6 versus 71.1, p=0.006). The proportion of patients with ischemic heart disease (2.5% versus 22.5%, p<0.001), and the presence of more than one intra-operative positive culture (3.9% versus 10.1%, p=0.049) were significantly higher in the long-prophylaxis group. No differences were found between groups in terms of gender, pre-operative ASA classification, body mass index, pre-operative CRP, type of revision, duration of surgery, days of hospitalization, or type of isolated micro-organisms. The prevalence of PJI was lower in patients who received a long antibiotic regimen (2.2% versus 6.9%, p=0.049). Figure 1 shows the cumulative probability of being free of PJI according to the antibiotic protocol (log rank test p=0.047).
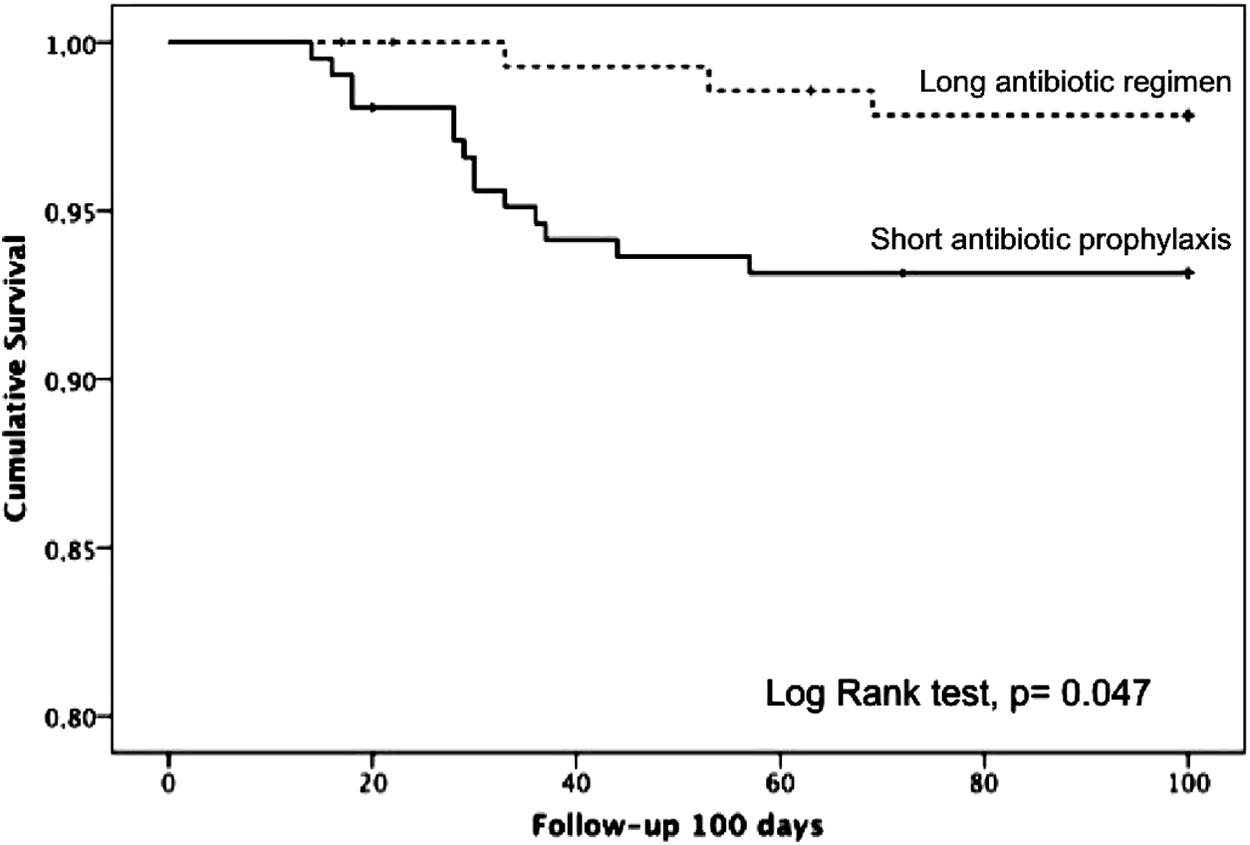
Cumulative probability of being free of prosthetic joint infection after 100 d from revision arthroplasty according to prophylactic antibiotic regimen.
SD=standard deviation; ASA=American Society of Anesthaesiologists; BMI=body mass index; COPD=chronic obstructive pulmonary diseases; CRP=C-reactive protein; IOC=intra-operative cultures; CoNS=coagulase-negative staphylococci; PJI=prosthetic joint infection.
All variables studied in the univariable analysis (age, male gender, pre-operative ASA ≥3, body mass index ≥35, hypertension, diabetes mellitus, ischemic heart disease, anti-coagulant treatment, obstructive pulmonary disease, rheumatoid arthritis, steroid therapy, chronic renal failure, total revision surgery as type of revision, pre-operative CRP >1.5 mg/dL, duration of surgery ≥120 min, any intra-operative positive cultures, and antibiotic regimen) were included in a step-wise forward logistic regression model analysis. There was a trend toward a higher PJI rate when the duration of surgery was ≥120 min (OR: 2.77, 95% CI: 0.93–8.23). A prolonged post-operative antibiotic treatment was the only variable associated independently with a lower rate of PJI (OR: 0.27, 95% CI: 0.07–0.99) (Hosmer-Lemeshow goodness-of-fit statistic, p=0.942). By removing those patients with true-positive intra-operative cultures who received four weeks of antibiotic treatment, the results were similar although differences did not reach statistical significance (PJI rate in short and long course 7.2% versus 2.4%, p=0.06).
Discussion
Controversy exists regarding the optimal duration of prophylaxis in surgery. The most recent U.S. guidelines for antimicrobial prophylaxis recognizes that the shortest effective duration of antimicrobial administration for preventing surgical site infection is not known [19]. The panel considered that the duration of antimicrobial prophylaxis should be less than 24 h for most procedures except cardiothoracic surgeries, for which a prophylaxis duration of up to 48 h has been accepted, although evidence to support this practice remains controversial [20,21]. This guideline is applicable for total joint arthroplasty, where 24 h or less of antibiotic prophylaxis duration has been documented as effective as longer than 24 h according to the literature [22–27]. However, in revision surgery the information about the duration of antibiotic prophylaxis is scant. Finnish Arthroplasty Register provided data on 43,149 knee arthroplasties, 40,135 primary total knee arthroplasties (93.0%), 2,166 total revisions (5.0%), and 848 partial revisions [8]. The infection rate was higher among revision surgeries (total or partial) than in primary arthroplasty and when antibiotic prophylaxis consisted of only systemic antibiotics without antibiotic-loaded cement. For this reason, in all revision surgeries in our center (total or partial), we use systemic antibiotics plus antibiotic-loaded cement as part of our standard protocol (see Patients and Methods). Unfortunately, Jamsen et al. [8] did not provide information about the duration of systemic antibiotic prophylaxis in primary or revision surgery. Recently, Liu et al. [28] reported a reduction in infection rate after adding vancomycin to cefazolin for 24 h in total knee revision arthroplasty, from 7.89% (15/190) to 3.21% (7/214, p=0.046). In our institution, a single dose of 800 mg of teicoplanin and two doses of ceftazidime were associated with an infection rate of 6.9% whereas the infection rate was 2.2% after prolonging the duration up to five days. The long prophylactic regimen was the only independent variable associated with a lower risk of infection (OR: 0.27, 95% CI: 0.07–0.99). Therefore, it is necessary to design further studies to establish the optimal duration of antibiotics in revision knee arthroplasty.
The first limitation of our study is its retrospective nature. However, there were no other modifications in the protocol of revision surgery or patient management. In addition, we performed a multivariable analysis to control for confounders that support the influence of antibiotic regimen. The second limitation is the relatively low number of patients included in the study; yet we have analyzed a relatively short period of time in a single center. Finally, the follow-up of the study was three months when the majority of authors recommend 365 days, however, recent studies [29] confirm that the majority of infections after arthroplasty occur within the first three months and only a small number are detected afterwards. This supports the change made by NHSN in January 2013 to a 90-d surveillance time period for these procedures.
In conclusion, five days of antibiotic prophylaxis has been associated with a lower infection rate, therefore, in the future it will be necessary to design studies to address the optimal duration of prophylactic antibiotics.
Footnotes
Author Disclosure Statement
No competing financial interests exist.