
Abstract
Abstract
Background:
Nosocomial meningitis and ventriculitis (MEN) are serious complications in neuro-critical care unit (NCCU) patients. Few data are available on the risk factors and mortality rates among NCCU patients with these disorders caused by multi-drug-resistant (MDR) pathogens. Our aim was to identify the risk factors for MEN caused by such pathogens and in-hospital deaths in critically ill neurologic patients and to evaluate the impact of empirical combination antibiotic therapy (ECAT) on the outcomes of these patients.
Methods:
We conducted a retrospective study of critically ill neurologic patients having nosocomial MEN who were admitted to the NCCU in a university teaching hospital from January 2003 to December 2013, with MEN being defined using the modified U.S. Centers for Disease Control and Prevention criteria for nosocomial infections.
Results:
In total, 6,149 consecutive NCCU patients were screened; 132 had MEN. Logistic regression analysis demonstrated that MDR MEN was related to infection with gram-negative (GN) bacteria (odds ratio 3.16; 95% confidence interval [CI] 1.08–9.25; p = 0.036), and inadequate initial antibiotic therapy (odds ratio 9.80; 95% CI 3.79–25.32; p < 0.001). The ECAT was associated with a lower mortality rate (hazard ratio 0.35; 95% CI 0.14–0.86; p = 0.022) in Cox proportional hazard regression analysis. The other variable independently associated with a greater mortality rate was a greater Simplified Acute Physiology Score II (hazard ratio 1.07; 95% CI 1.01–1.13; p = 0.018).
Conclusions:
Initial combination therapy improves the in-hospital mortality rate among NCCU patients with nosocomial MEN. Inadequate initial antibiotic therapy and GN infection were associated with MDR MEN.
H
Previous studies have been conducted to identify risk factors associated with surgical site infections after neurologic procedures [2–5]. However, most have focused mainly on neurosurgical-associated MEN or infections acquired in the NCCU, and none has explored the impact on the outcomes of MEN caused by MDR pathogens. Additionally, the factors that cause MDR infection and the major determinants of in-hospital death have not been elucidated fully. To address this gap, the present study was designed to investigate the risk factors for MDR MEN and in-hospital death among a cohort of critically ill neurologic patients having MEN. The impact of empirical combination antimicrobial therapy (ECAT) on the mortality rate also was evaluated.
Patients and Methods
Patients and inclusion criteria
This study was approved by the Ethics Committee for the Evaluation of Biomedical Research Projects of Huashan Hospital. The requirement for informed consent was waived because of the retrospective and noninterventional design of the study.
Figure 1 shows a flow chart of the study. All patients admitted to the NCCU of the level I Neurotrauma Center of Huashan Hospital, a university teaching hospital, from January 2003 to December 2013 were evaluated retrospectively. The clinical and microbiologic databases were screened to identify all cases of nosocomial MEN that met the diagnostic criteria defined by the U.S. Centers for Disease Control and Prevention [6]:
• MEN that develops more than 48 h after hospital admission and as late as three d after discharge or 30 d after surgery. • Definitive microbial culture from the cerebrospinal fluid (CSF); • At least one of the following signs or symptoms (with no other recognized cause): Fever >38°C, headache, stiff neck, meningeal signs, cranial nerve signs, or irritability; and • At least one of the following laboratory abnormalities: An increased white cell count, an elevated serum protein concentration or a decreased glucose concentration in the CSF; micro-organisms evident on Gram staining of the CSF; microbial culture from blood; a positive laboratory CSF, blood, or urine test; a diagnostic single antibody titer (immunoglobin [Ig] M); or a fourfold increase in the paired serum pathogen-specific IgG concentration.
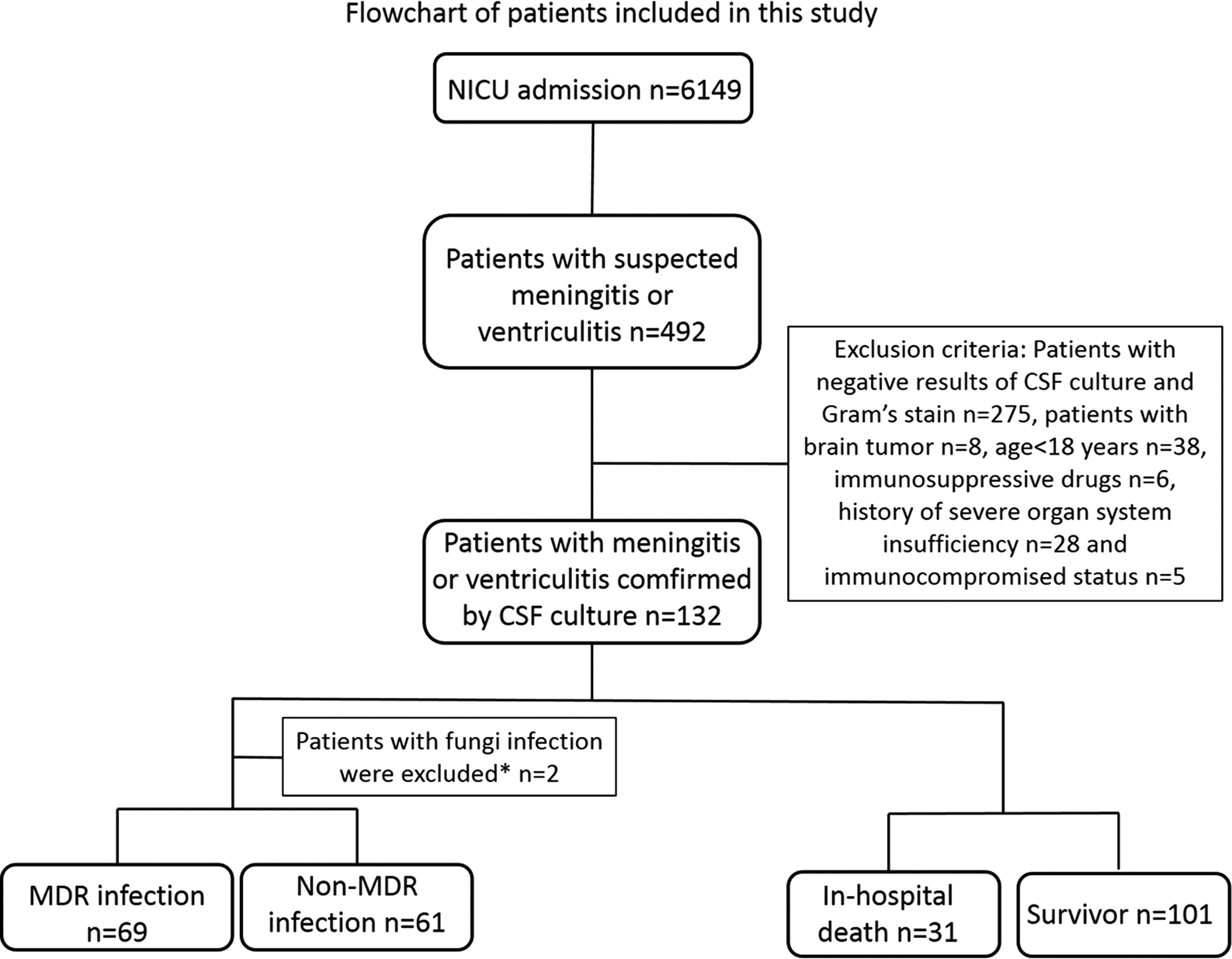
Flow chart of the study. *Two patients with brain injury having only fungal MEN were excluded from this analysis, because routine fungal susceptibility testing is not recommended in our hospital.
Samples of CSF were collected from the external ventricular drainage (EVD) site or by sustainable lumbar drainage when EVD was not available. Patients were excluded if the results of three CSF cultures or Gram-stained smears were negative during a 6 day period. Other exclusion criteria included age <18 years, presence of a brain tumor, current use of immunosuppressive drugs, history of severe organ system deficiency, and immunocompromised status.
Data collection
The severity of head trauma was measured using the Glasgow Coma Scale, with scores ranging from 3 (deep coma or death) to 15 (fully awake). Other data collected were age, gender, diagnosis, Simplified Acute Physiology Score II (SAPS II) at the time of admission, open compound cranial fractures, basilar skull fractures (including sinus and inner table fracture), CSF leakage, surgical procedure performed (includes decompressive craniectomy or craniotomy with hematoma evacuation), intracranial pressure (ICP) monitoring performed (all ICP monitors were placed in the ventricle and could be used for CSF drainage if necessary), EVD procedure performed (all EVD drainage chambers had anti-reflux valves), incidence of pneumonia, severe sepsis or septic shock, length (d) of the period at risk for nosocomial MEN, total treatment time, pathogenic organisms identified in the CSF, empiric and definitive antimicrobial regimens used, results of antibiotic susceptibility testing, length of hospital stay, and in-hospital mortality rate.
Definitions
Pathogenic organisms were considered to be resistant to a certain class of antibiotic if they were reported as intermediate or resistant to at least one of the agents in that class. Pathogens were defined as MDR if they were resistant to at least one representative drug in three of the seven categories of antimicrobial agents: Cephalosporins, fluoroquinolones, aminoglycosides, carbapenems, extended-spectrum penicillins, macrolides, and β-lactam/β-lactamase inhibitors [1].
The onset of nosocomial MEN coincided with the collection date (≥48 h after admission) of the first CSF culture yielding the pathogen. The period (d) during which the patient was at risk for MEN was defined as the period between hospital admission and MEN onset. We also recorded the total NCCU stay and the post-MEN-onset NCCU stay (the endpoint of both was NCCU discharge or death). Critically ill patients who required surgery were given prophylactic antibiotics using our institutional protocol: 1 g of ceftriaxone sodium (or 1 g of vancomycin if a patient was allergic to penicillin) administered intravenously within 60 min prior to surgical incision and discontinued within 24 h after surgery.
Any antimicrobial agents used before the in vitro susceptibility data of the CSF isolate were available were included in the final analysis of the empiric antimicrobial regimens. Each empiric regimen was then designated as adequate or inadequate according to whether the regimen contained any antimicrobial agents with activity against the pathogens isolated in vitro [7]. Definitive therapy was considered to be a treatment that was continued or started on the day the antibiogram results became available. Antibiotic treatment was continued until three consecutive CSF cultures from separate days produced negative results.
Statistical analysis
Categorical variables are reported as percentages and were assessed with the χ2 test or two-tailed Fisher exact test as appropriate. The results are reported as odds ratio (OR) with 95% confidence interval (CI). Continuous variables are expressed as the mean ± standard deviation or median and interquartile range. Normally and non-normally distributed continuous variables were compared with the Student t-test and the Mann–Whitney U test, respectively. Logistic regression was performed to adjust for multiple predictors of MDR infection. Cox regression analysis was performed to identify risk factors for in-hospital death of patients with MEN. The results of Cox regression are reported as the hazard ratio (HR) with 95% CI. Survival curves were prepared using the Kaplan–Meier method with the log-rank test applied to compare survival distributions. The backward mode with a p value threshold of 0.25 for elimination was used for multivariable regression. All p values were two-tailed, and statistical significance was set at p < 0.05. All statistical analyses were performed using STATA software (version 11.0; STATA Corporation, College Station, TX).
Results
Patient characteristics
In total, 6,149 consecutive critically ill patients were admitted to the NCCU of the level I Neurotrauma Center of our university teaching hospital from January 2003 to December 2013. Of these patients, 132 (97 males, 35 females; mean age 44 y; age range 18–77 y) were found to have MEN on the basis of positive CSF cultures and were analyzed in this study. The diagnosis at admission was traumatic brain injury (TBI) in 89 patients, primary intracerebral/intraventricular hemorrhage (PICH/PIVH) in 36, primary subarachnoid hemorrhage in six, and ischemic stroke in one. In total, 152 strains of offending organisms were confirmed by CSF culture and Gram staining.
Incidence of MEN and distribution of pathogens
Patients with at least one of the following risk factors were considered to have been exposed to the same risks as those who developed MEN: Open compound cranial fracture, basilar skull fracture, CSF leakage, previous surgical procedure, ICP monitoring, previous EVD procedure, pneumonia, or severe sepsis or septic shock. Over the 11-year study period, 5,360 of 6,149 patients were exposed to the same risks as those who developed MEN. Therefore, the incidence of MEN was 2.5% (132/5,360) in our NCCU. From 2003 to 2013, gram-negative (GN) bacteria were predominant, accounting for 71.7% of all pathogens (109/152) that caused MEN in the NCCU setting. Gram-positive (GP) bacteria accounted for 25.7% (n = 39), and fungi accounted for 2.6% (n = 4). Acinetobacter baumannii (25.7%; 39/152), Klebsiella pneumoniae (15.1%; n = 23), and Pseudomonas aeruginosa (8.6%; n = 13) were the three most common pathogens causing MEN (Table 1).
Fungal drug resistance was not tested because susceptibility testing of fungi is not recommended on a routine basis in our hospital.
MDR = multi-drug resistant; PDR = pan-drug resistant.
Treatment
All patients were treated empirically with extended-spectrum antibiotics within a few hours of MEN onset. No patients died before the CSF culture results were available. The antimicrobial agents were administered either intravenously or, if necessary, intrathecally or intraventricularly. The doses for intravenous and intrathecal/intraventricular administration conformed to the current recommendations for the treatment of nosocomial MEN [8,9]:
• Intravenous administration: Ampicillin 2 g q 4 h; ceftriaxone 2 g q 12 h; ceftazidime 2 g q 8 h; cefepime 2 g q 8 h; piperacillin/tazobactam 4.5 g q 6 h; cefoperazone-sulbactam 3 g q 8 h; meropenem 1 g q 8 h; ciprofloxacin 400 mg q 8 h; vancomycin 1 g q 12 h; trimethoprim-sulfamethoxazole 5 mg/kg q 8–12 h; tigecycline loading dose of 100 mg followed by 50 mg q 12 h; amikacin 15 mg/kg q 24 h; gentamicin 5 mg/kg q 24 h; colistin 5 mg/kg/day divided into two or three doses; and fluconazole 400 mg q 24 h. • Intrathecal or intraventricular administration (antimicrobial agents infused directly into the ventricles or lumbar subarachnoid space through a drainage catheter; the catheter usually was closed for one h to maintain an effective CSF concentration): Vancomycin 10 mg q 24 h; gentamicin 4 mg q 24 h; and amikacin 30 mg q 24 h or colistin 5 mg q 12 h.
The antibiotic regimens were concordant with the recommendations for empiric and definitive therapy of nosocomial MEN in previous studies [8–12]. The median duration of treatment was 18 d. In the empiric phase of treatment, monotherapy (antibiotic therapy involving a single drug) was used in 61 patients (46.2%), and combination therapy was used in the remainder. Only 16 of 61 patients (26%) on empiric monotherapy received appropriate antibiotics, whereas 41 of 71 patients (58%) on empiric combination therapy were so treated (OR 3.84; 95% CI 1.83–8.06; p = 0.0004). Thus, the patients in the initial monotherapy group were at a significantly greater risk of being treated with inappropriate antibiotics than were the patients in the initial combination therapy group. A total of 44 patients (33.3%) received combination therapy in the definitive phase. Intrathecal/intraventricular therapy was applied in 22 patients (16.7%) in the empiric phase and 50 (37.9%) in the definitive phase. For ventricular catheter-related MEN, the therapeutic strategies included not only antibiotic treatment but also the exchange of a new ventricular catheter or removal of the original catheter and continuous drainage of CSF via a lumbar subarachnoid catheter.
Risk factors for MDR bacterial infection
In total, 130 patients were eligible for analysis of the risk factors for MDR MEN (Table 2). Two patients with only fungal MEN were excluded from this analysis because routine fungal susceptibility testing is not recommended in our hospital. The univariable analysis revealed that MDR infection was more likely in NCCU patients having severe sepsis or septic shock (OR 2.89; 95% CI 1.21–6.88; p = 0.015). Inadequate initial antibiotic therapy also was associated with MDR MEN (OR 9.39; 95% CI 4.20–20.98; p < 0.001). Among patients with MDR MEN, the rate of infection caused by GN bacteria (88%; 61/69) was significantly greater than that in patients without MDR infection (61%; 37/61; p < 0.001). The antibiotic treatment time in the MDR group was significantly longer than that in the non-MDR group (20.0 [14.0–30.0] d vs. 15.0 [10.0–22.5] d, respectively; p = 0.007).
Data are compared by the Student t-test (t), and the results are shown as mean ± standard deviation.
Data are compared by the Mann–Whitney U test (U), and the results are shown as median and interquartile range.
CI = confidence interval; CSF = cerebrospinal fluid; EVD = external ventricular drainage; GCS = Glasgow Coma Scale; GN = gram negative; ICP = intracranial pressure; MEN = meningitis or ventriculitis; NCCU = neuro-critical care unit; SAPS II = Simplified Acute Physiology Score II.
Of all variables analyzed, GN infection (OR 3.16; 95% CI 1.08–9.25; p = 0.036) and inadequate initial antibiotic therapy (OR 9.80; 95% CI 3.79–25.32; p < 0.001) were associated with MDR MEN in the final logistic regression analysis.
Major determinants of in-hospital death in NCCU patients with nosocomial MEN
The overall in-hospital mortality rate was 23.5% (31/132). According to the univariable analysis, the following eight factors were associated with a high risk of in-hospital death: GN infection (OR 6.73; 95% CI 1.51–29.94; p = 0.004), pneumonia (OR 4.53; 95% CI 1.28–15.99; p = 0.011), severe sepsis or septic shock (OR 7.94; 95% CI 3.23–19.53; p < 0.001), MDR bacterial infection (OR 4.11; 95% CI 1.62–10.43; p = 0.002), open compound cranial fractures (OR 3.35; 95% CI 1.24–9.07; p = 0.021), inadequate initial antibiotic therapy (OR 5.52; 95% CI 1.96–15.52; p < 0.001), and a greater SAPS II (41.4 ± 2.5 vs. 32.4 ± 1.2; p < 0.001). Patients who received combination therapy in the empiric phase were more likely to survive than patients who received monotherapy (OR 0.28; 95% CI 0.12–0.67; p = 0.004) (Table 3). However, in the final Cox regression analysis, only a greater SAPS II (HR 1.07; 95% CI 1.01–1.13; p = 0.018) and ECAT (HR 0.35; 95% CI 0.14–0.86; p = 0.022) were independent major determinants of in-hospital death. It is noteworthy that, according to our results, a β-lactam/β-lactamase inhibitor-based combination antibiotic regimen (OR 0.14; 95% CI 0.02–1.12; p = 0.043) was superior to all of the other combination antibiotic regimens.
Data are compared by the Student t-test, and the results are shown as mean ± standard deviation.
Data are compared by Mann–Whitney U test, and the results are shown as median and interquartile range.
Cefoperazone-sulbactam or piperacillin-tazobactam with aminoglycoside or fluoroquinolone.
Meropenem with aminoglycoside or fluoroquinolone.
Vancomycin with aminoglycoside, fluoroquinolone, or third-generation cephalosporin.
CI = confidence interval; CSF = cerebrospinal fluid; ECAT = empiric combination antibiotic therapy; EVD = external ventricular drainage; GCS = Glasgow coma scale; GN = gram-negative; ICP = intracranial pressure; MDR = multi-drug resistant infection; NICU = neuro-Intensive care unit; SAPS II = Simplified Acute Physiology Score II.
Discussion
Incidence, in-hospital death, and pathogen distribution
The incidence of nosocomial MEN ranges from 0.8% to 6.2% in previous publications [4,13]. In the present study, the incidence was 2.5% (132/5,360), which is lower than the 5.7% reported in European studies but slightly greater than the 2.2% reported in North America [13]. However, the rate of nosocomial MEN reported in our series may not be directly comparable to that reported in previous studies because only patients in the NCCU, such as those with TBI and PICH, were included in our study, whereas the other studies included all patients undergoing craniotomy. In addition, our study excluded patients who were believed to have nosocomial MEN without a positive CSF culture, whereas other studies did not exclude such patients.
Nosocomial MEN is one of the most serious complications in NCCU patients, and the mortality rate ranges from 15% to 35% [9,14]. In the present series, the in-hospital mortality rate was 23.5% (31/132), which is in line with previous studies.
Overall, 152 pathogens were reported in the 132 patients with nosocomial MEN in our series. Gram-negative bacteria predominated, accounting for 71.7% of all pathogens. Our results are in accordance with those of previous studies showing that GN bacteria play a substantial role in MEN, representing 70% to 80% of the causative pathogens [14,15]. In the present study, A. baumannii accounted for 25.7% of all pathogens isolated from the CSF. This result is similar to the finding in some other studies that this organism was the most commonly identified offending organism among neurosurgical patients with nosocomial meningitis [14,16].
MDR MEN
Gram-negative infection
Our multivariable analysis revealed that GN infection was an independent risk factor for MDR pathogens. This observation is likely attributable to the relatively large proportion of patients (39/109; 36%) with A. baumannii, which is almost always an MDR pathogen [17], among the GN infection group. When A. baumannii infection was confirmed by CSF culture, either treatment with meropenem alone, tigecycline or colistin, or colistin alone was administered intravenously. When indicated by in vitro susceptibility results, colistin or an aminoglycoside was administered by an intrathecal/intraventricular route if necessary.
Inadequate initial antibiotic therapy
In the present study, inadequate initial antibiotic therapy was associated independently with the antimicrobial susceptibility profile of the MDR isolates. The susceptibility pattern of the infecting organism was not available at the time the empiric therapy was prescribed. While waiting for these results, the epidemiologic profile of the NCCU itself should be used to select the optimal empiric regimen.
We found that inadequate initial antibiotic therapy was strongly correlated with in-hospital death, but this association was not confirmed in the multivariable analysis. To date, only one study has investigated the relation between inadequate initial therapy and in-hospital death in patients with nosocomial MEN; it was reported that inadequate initial therapy was associated with death [18]. Notably, however, this study involved patients with MEN caused only by A. baumannii. Additionally, the authors did not exclude patients with brain tumors, who tend to have shorter hospital stays than do patients in the NCCU. Moreover, the overall mortality rate was significantly greater than that in the present study (>70%), and the sample (22 patients) was too small to support a consolidated statistical conclusion. In addition, the authors did not perform multivariable analysis. This could lead to biased results, because the patients frequently were affected by severe neurologic deficits, and the underlying neurologic state was a confounding factor for death [18].
According to studies in patients with ventilator-associated pneumonia, the effect of inadequate initial therapy on the in-hospital mortality rate is controversial [7,19]. Dupont et al. [20] concluded that studies reporting inadequate initial therapy as an independent risk factor for death were those with the highest mortality rates or the highest rates of inadequate initial therapy. Trauma patients have a significantly lower mortality rate than do medical patients, who usually have serious systemic illness [7]. Therefore, the absence of a difference in the mortality rate in our cohort may have been related to differences in the patient population and lower severity of disease compared with previous studies. Inadequate initial therapy might be of major importance in critically ill medical patients with severe systemic illness, who have high mortality rates, but may have a weaker influence on the outcome of patients having only brain trauma or cerebrovascular disease. Moreover, in the present study, the MDR group more frequently received inadequate initial therapy. This suggests that a lack of adequate antimicrobial therapy facilitates the development of more invasive infection. Nevertheless, few studies have focused on the effect of inadequate initial therapy on the in-hospital mortality rate in NCCU patients having MDR MEN. Further studies on this topic are needed.
Empirical combination antibiotic therapy
The present results revealed that ECAT could significantly improve the in-hospital mortality rate among patients having MEN and that use of β-lactam/β-lactamase inhibitor-based empiric combination therapy (OR 0.14; 95% CI 0.02–1.12; p = 0.043) may be an effective way to reduce the in-hospital mortality rate of patients with MEN. Combination antibiotic therapy was the most important independent protective factor; it also is the only factor that can be controlled by clinicians. This association was confirmed by survival curve analysis (p = 0.0035; log-rank test) (Fig. 2). Kim et al. [9] recommended intravenous meropenem plus an intrathecal or intraventricular aminoglycoside as empiric antimicrobial therapy in patients with risk factors for Acinetobacter MEN. Van de Beek et al. [8] and other authors [12,21] have emphasized the importance of combination empiric antimicrobial therapy for MEN in critically ill neurologic patients because such patients tend to have external drainage devices and a long hospitalization, meaning that they are at high risk of developing MDR, polymicrobial, and multi-organ infections. Thus, ECAT may enhance the likelihood of appropriate therapy in the early phase, treating other concomitant organic infections such as pneumonia and sepsis and shortening the duration of MEN symptoms, which is considered a determinant of outcome [22].
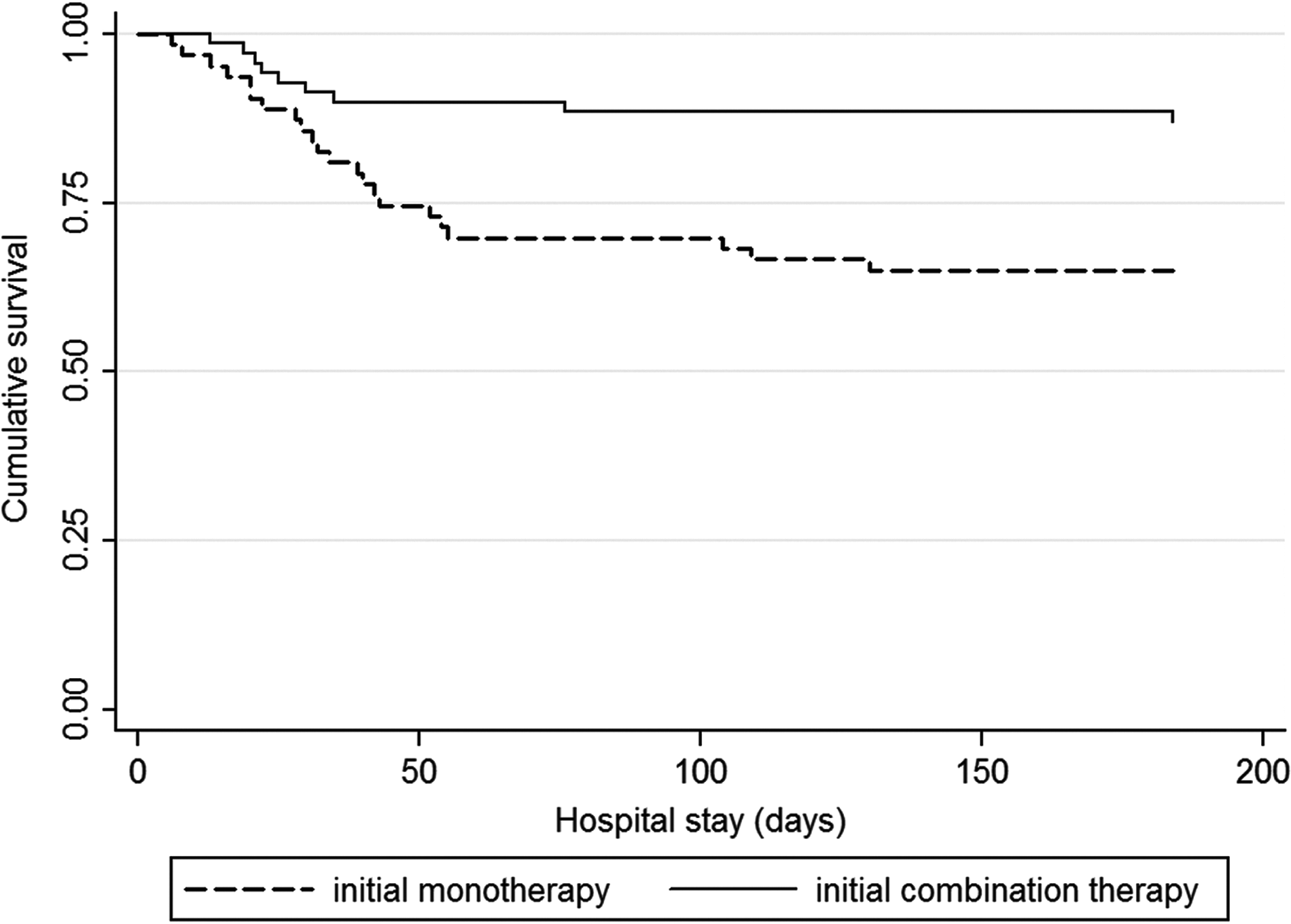
Cumulative survival curves of patients receiving combined antibiotic therapy compared with patients having monotherapy in the empiric phase of treatment. (Log-rank test, p = 0.0035.)
Notably, the outcome of MEN did not appear to be related to the antibiotic administration route in the present study, although a higher CSF antibiotic concentration can be achieved by intrathecal/intraventricular than by intravenous administration [23]. A possible reason for this is that CSF penetration of drugs is variable and depends on the integrity of the blood–brain barrier. When the brain is injured by trauma or a hematoma, the blood–brain barrier is severely impaired; thus, intravenously administered antibiotics can penetrate into the brain such that an effective antimicrobial concentration can be achieved in the CSF [24]. Our results therefore suggest that combination therapy plays a more critical role in the early phase than does the drug delivery route in the treatment of MEN in NCCU patients.
SAPS II
In the present series, a greater SAPS II was an independent risk factor for in-hospital death. This can be explained by the fact that a greater SAPS II usually indicates impaired immunity and significant underlying conditions [25]; thus, critically ill patients with a greater SAPS II are more vulnerable to both neurologic and non-neurologic organ system dysfunction than are patients with a lower score.
Because of the relatively low incidence of nosocomial MEN and ethical considerations, it is difficult to identify a clinical trial showing clearly the risk factors associated with MDR infection and death in NCCU patients. The prevention and management of nosocomial MEN pose substantial challenges, especially with the emergence of infection caused by MDR pathogens. The present study involved the largest series of patients with nosocomial MEN in the NCCU examined to date. The findings indicate that the use of initial combination antibiotic therapy is superior to monotherapy in treating this serious infection and provided useful information regarding the cause of MDR MEN.
Conclusion
We have highlighted the importance of ECAT as a protective factor against in-hospital death and may improve the outcome of NCCU patients having MEN. Inadequate initial antibiotic therapy and GN infection were risk factors for nosocomial MDR MEN.
Footnotes
Acknowledgments
We thank Dr. Xiaofei Jiang and Dr. Jian Chen for their enabling of convenience in data collection.
This study was supported by the National Natural Science Foundation of China (NSFC Grants 30371454, 81271375, and 81171133), The Science and Technology Commission of Shanghai Municipality Project (10JC1402300), and the Shanghai Nature Science Foundation (08411952000).
Author Disclosure Statement
No competing financial interests exist.