
Abstract
Abstract
Background:
Antibiotics combined with lavage have demonstrated a reduction in the bacterial contamination and decreases surgical site infection (SSI) rate. SSI leads to an immunocompromised situation, as immunologic defense is focused on controlling the septic focus, leaving unattended the neoplasm. It has been described that SSI may result in a worse oncologic outcome. The aim of this study is to evaluate prospectively the effect of peritoneal lavage with clindamycin and gentamicin on the oncologic outcome of colorectal tumors.
Methods:
A randomized study of patients with diagnosis of colorectal neoplasms and undergoing elective surgery was performed at our institutions between January and September 2011. Patients were randomly assigned into two groups: Those undergoing an intra-abdominal lavage with normal saline (Group 1) and those undergoing an intra-abdominal lavage with a gentamicin-clindamycin solution (Group 2). Recurrence, global survival, and disease-free survival were investigated.
Results:
One hundred and four patients were analyzed, with 52 in each group. After a minimum follow-up of 42 mo, mean disease-free survival was 37.2 ± 14.2 mo in Group 1 and 25.8 ± 16.3 mo in Group 2 (mean difference 11.4; confidence interval (CI) 95% (2.2–25.1); p = 0.009). Mean global survival was 44.2 ± 11.9 mo in Group 1 and 34.1 ± 14.1 mo in Group 2 (mean difference 10.1; CI 95% (2.2–18);p = 0.016).
Conclusion:
The intra-peritoneal lavage with gentamicin and clindamycin increases the disease-free and global survival colorectal tumors.
P
Several studies have demonstrated that flushing the peritoneal cavity may reduce the bacterial load, inhibit bacterial proliferation, and possibly minimize peritoneal adhesions. Antibiotics combined with the lavage might achieve a further reduction in the bacterial contamination and decrease the SSI infection rate [5]. This fact has been demonstrated in a previous study of our group [6].
SSI leads to an immunocompromised situation, as immunologic defense is focused on controlling the septic focus, leaving unattended other potential threats (e.g., neoplasms). Therefore, it has been described that SSI may result in a worse oncologic outcome [7].
The aim of this study is to evaluate the effect of peritoneal lavage with clindamycin and gentamicin, on the oncologic outcome colorectal tumors, and compare it with patients undergoing a peritoneal lavage only with normal saline.
Patients and Methods
A randomized study was performed at our institutions between January and September 2011. Inclusion criteria were a diagnosis of colon neoplasms and plans to undergo an elective surgery with curative aims. Open surgical approach was performed in all the patients included. Exclusion criteria were a pre-operative diagnosis of chronic renal failure (because of the risk of nephrotoxicity associated with intraperitoneal gentamicin absorption), allergy to gentamicin or clindamycin, and diagnosis of rectal cancer.
The sample size calculation was based on historic data of our center of mean global survival of 32 mo and an expected global survival of 38 mo in the experimental group. At 80% power and a significance level of p = 0.05, it was calculated that 53 patients were required in each arm of the study.
Patients were randomly assigned using a random-number table into two groups: Those undergoing an intra-abdominal lavage with a gentamicin-clindamycin solution (Group 1) and those undergoing an intra-abdominal lavage with normal saline (Group 2). Perioperative systemic antibiotics (ciprofloxacin 400 mg and metronidazole 1,500 mg; single dose pre-operatively, within 30 min of incision, and redosed after 4 h when the surgery is prolonged over that time) were used in both groups. No mechanical bowel preparation took place in any patient.
Methodology: Irrigation Technique
The lavage was performed immediately prior to closure of the abdominal wall. In Group 1, a lavage with an antibiotic solution, including gentamicin (240 mg) and clindamycin (600 mg) dissolved in 500 mL normal saline was performed. In Group 2, an irrigation of the entire abdominal cavity was performed with 500 mL normal saline.
In both groups, the solution was allowed to sit in the abdominal cavity for 3 min. Then it was aspirated.
Follow-Up Scheme
All the patients presented at least a minimum follow-up of 42 mo. The follow-up was performed by the surgeon and the oncologist every 3 mo during the first 2 post-operative years and every 6 mo from the 3rd to the 5th post-operative years. Complementary tests performed at each moment are showed in Table 1.
CEA = carcinogenic antigen; CT = computerized tomography.
Parameters
The investigated clinical parameters were age, gender, comorbidities, location of the neoplasm, complications (anastomotic leak, organ-space SSI, and incisional SSI), mortality, and hospital stay. Oncologic parameters include recurrence, global survival, and disease-free survival. Recurrence included local recurrence and distant metastases. Recurrence was defined as the presence of images suspicious of neoplasm at CT scan or colonoscopy and confirmed by histological analysis. The recurrence was evaluated by an oncologist blinded to the irrigation technique used.
Incisional SSI was defined as the presence of a purulent discharge from the surgical incision and confirmed with microbiological culture. Incisional SSI was determined by an epidemiology nurse blinded to the treatment groups. Infection surveillance was extended for 30 d following discharge.
Statistics
Statistical analysis was performed with the statistical software SPSS 19.0 for Windows (SPSS, Inc., Chicago, IL). Quantitative variables that followed a normal distribution were defined by the mean and standard deviation. For non-Gaussian variables, the median and range were used. Qualitative variables were defined by number and percentage of cases.
Comparison of variables was performed with a Student t-test for quantitative variables following a Gaussian distribution. Non-parametric tests (Mann-Whitney) were used for non-Gaussian variables. Comparison of qualitative variables was performed with the Chi-square test; in those cases with fewer than five observations in the cell, the Fisher exact probability method was used. Survival curves were evaluated by Kaplan-Meier test and compared with log rank. P < 0.05 was regarded as significant. The study was approved by the local ethics committee.
Results
A total of 106 patients were assessed for eligibility, 53 in each group. Perioperative mortality appeared in one patient in each group and these cases were excluded, so that finally, 52 patients were analyzed in both groups. COHORT flow diagram is shown in Figure 1. There were no differences in demographic data and comorbidities between groups, and their distribution is summarized in Table 2. The tumors were located in the right colon (40%), the transverse colon (6%), the left colon (54%).
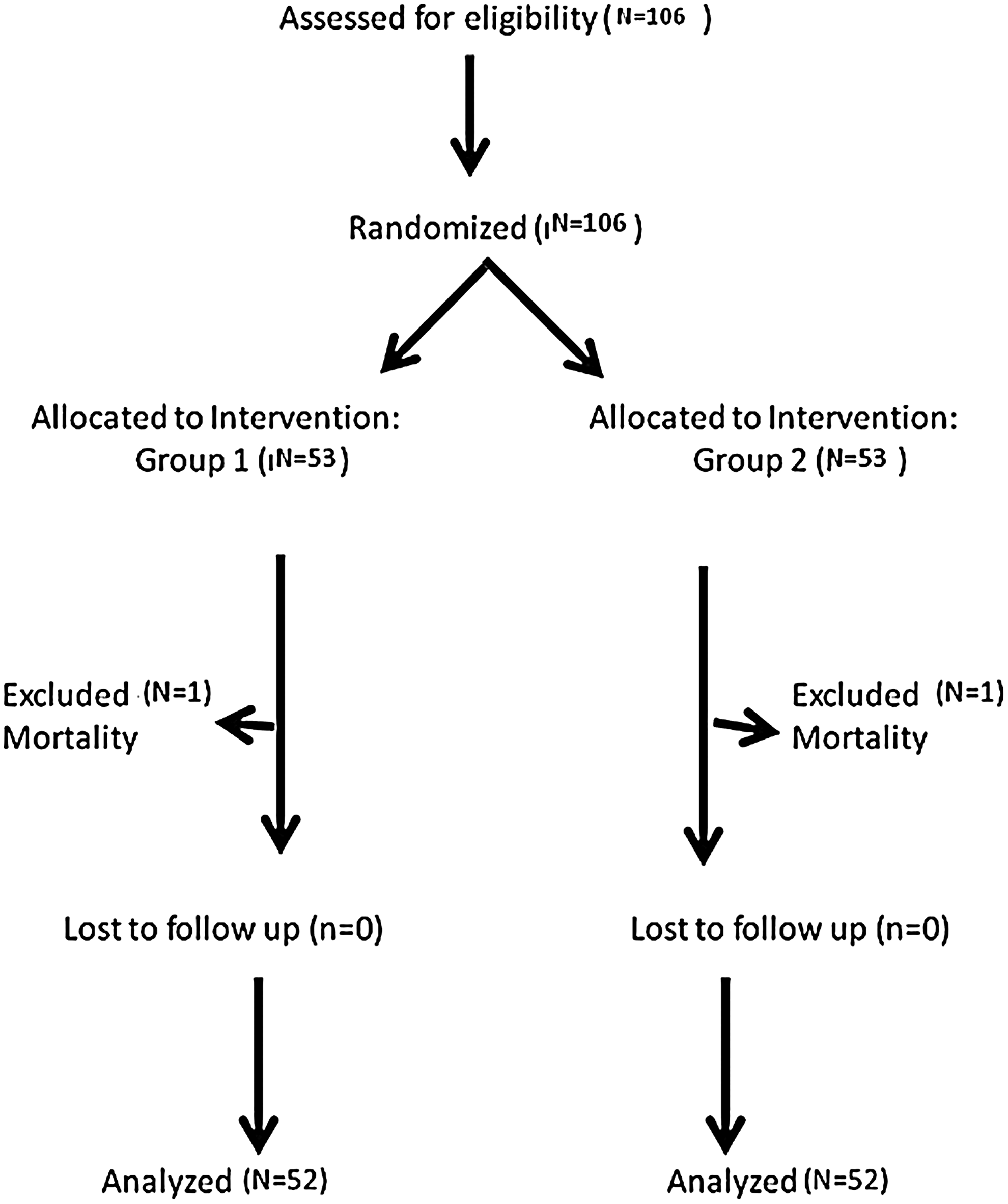
COHORT flow diagram.
NS = non-significant.
The surgical techniques are described in Table 3. There were no substantial differences in the surgical techniques between groups.
NS = non-significant.
Anastomotic leaks appeared in two patients in Group 1 and three in Group 2 (non-significant: NS). Median hospital stay was 6.5 d (range 5–14 d) in Group 1 and 6 d (range 5–32 d) in Group 2 (NS).
The incisional SSI rate was 3.8% in Group 1 and 13.5% in Group 2 (p = 0.009; OR = 4.94; CI 95% (1.27–19.19). The organ-space SSI rate was 0% in Group 1 and 5.8% in Group 2 (p = 0.014; OR = 2.14; CI 95% (1.13–3.57). According to the AJCC tumoral staging classification, there were no differences in the tumoral stages between groups (Table 4).
NS = non-significant.
All the patients with stage III tumors received adjuvant chemotherapic treatment, following a FOLFOX Scheme (12 cycles every 14 d). The interval between surgery and initiation of chemotherapy was 8 wks.
Oncologic Outcome
After a minimum follow-up of 42 mo, global recurrence rate was 19.2% (10 patients) in Group 1 and 36.5% (19 patients) in Group 2 (p = 0.04). A substantial difference in the distribution of recurrences could not be observed (Table 5). Global survival rate in Group 1 was 90.4% and in Group 2 69.2% (p = 0.016).
NS = non-significant.
Mean disease-free survival was 37.2 ± 14.2 mo in Group 1 and 25.8 ± 16.3 mo in Group 2 (mean difference 11.4; CI 95% (2.2–25.1); p = 0.009) (Fig. 2). Mean global survival was 44.2 ± 11.9 mo in Group 1 and 34.1 ± 14.1 mo in Group 2 (mean difference 10.1; CI 95% (2.2–18); p = 0.016) (Fig. 3). When stratifying the sample depending on the tumoral stage, and analyzing just stages II and III, that are the majority ones, global survival was still longer in Group 1 for both stages. (Fig. 4); for stage II, mean survival was 44.8 ± 8.2 mo in Group 1 and 40.6 ± 8.3 mo in Group 2 (Mean difference 4.2; CI95% (2.2–12,8); p = 0.05); for stage III, mean survival was 39 ± 10 mo in Group 1 and 29.7 ± 9.5 mo in Group 2 (Mean difference 9.3; CI 95% (7.3–25-7); p = 0.04).
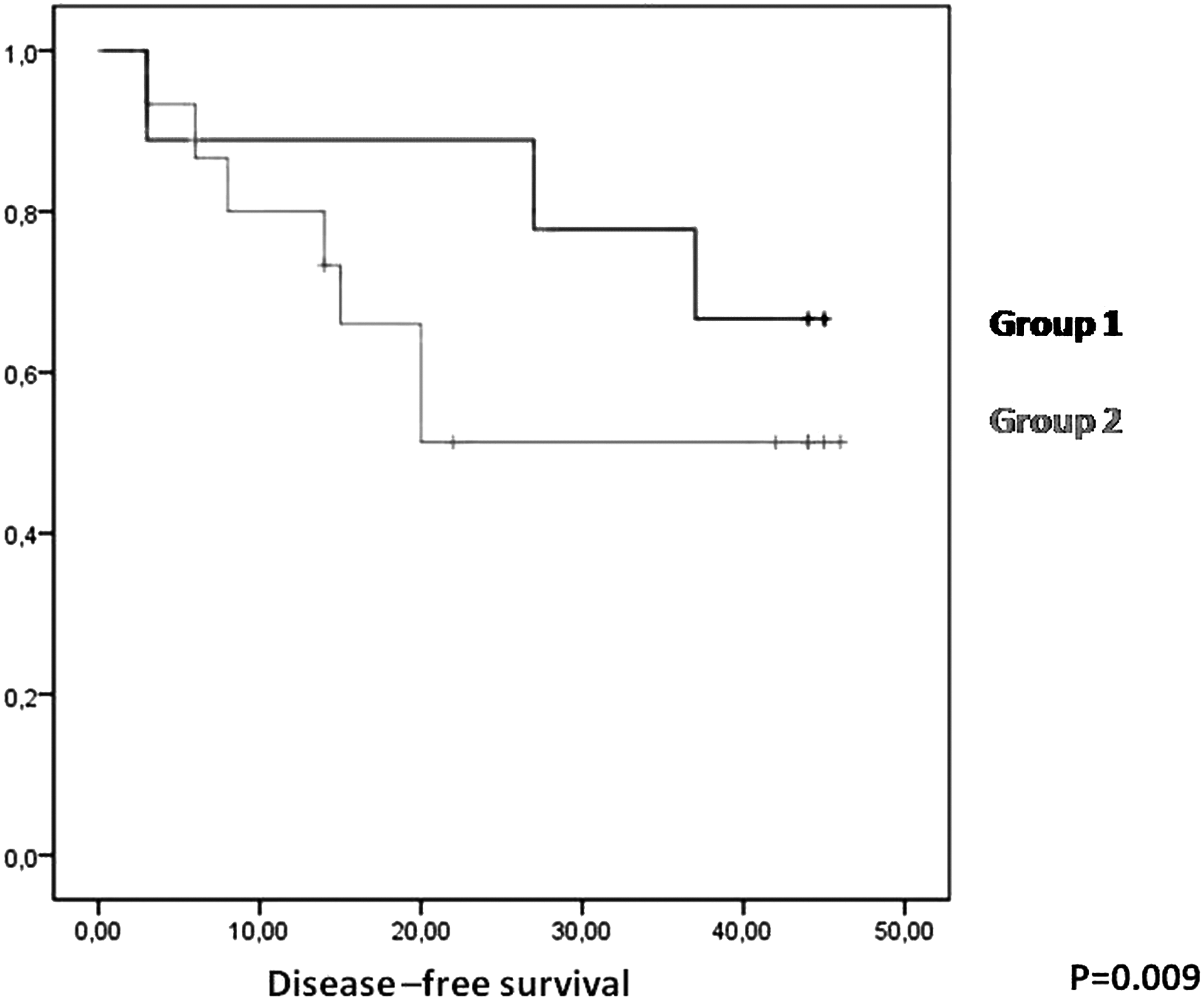
Disease-free survival between groups.
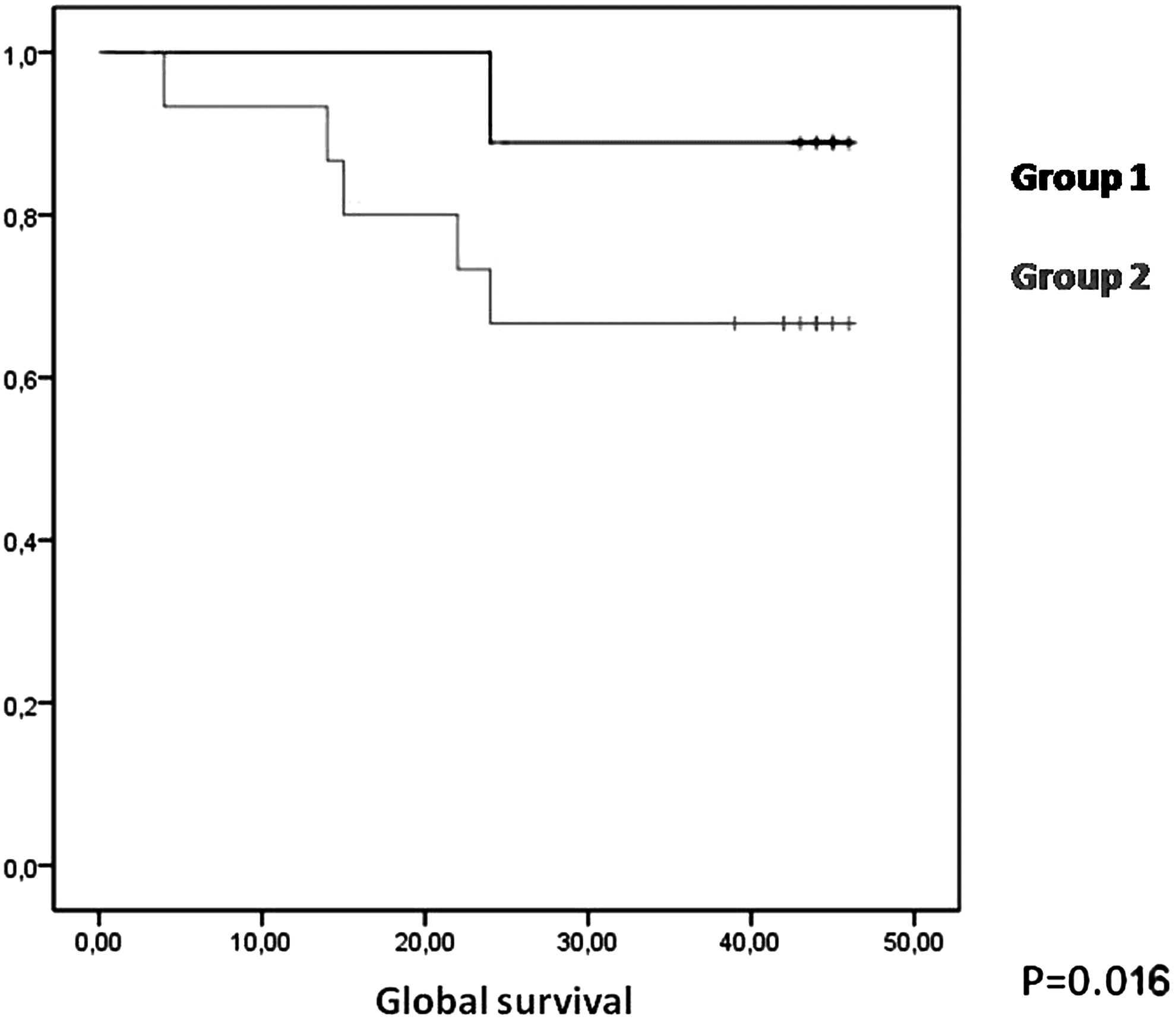
Global survival between groups.
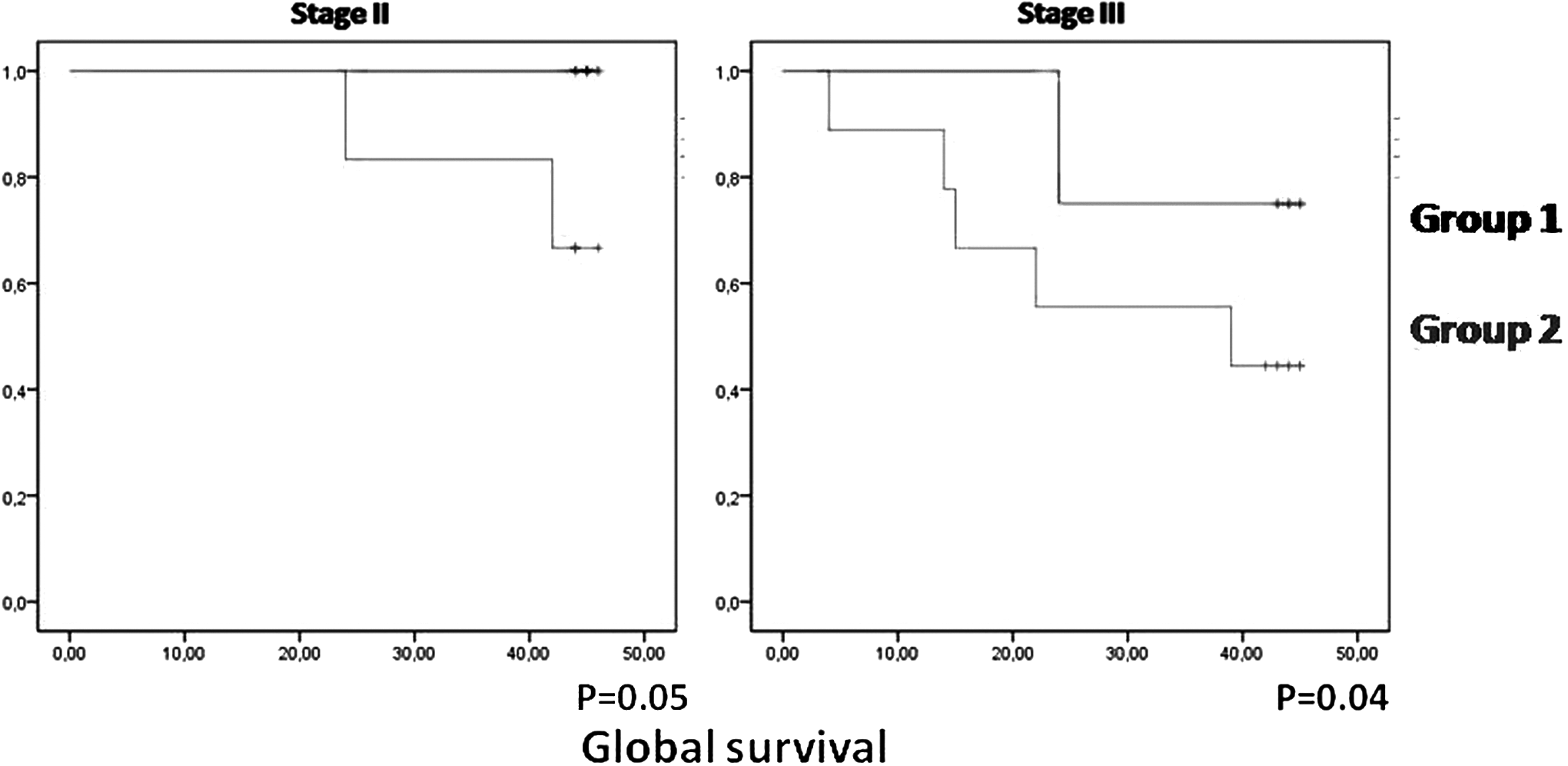
Global survival depending on the tumoral stage, between groups.
Given that SSI could be a confusion factor, a relation between SSI and disease-free survival or global survival was investigated, without obtaining any significant association (Fig. 5 and 6).
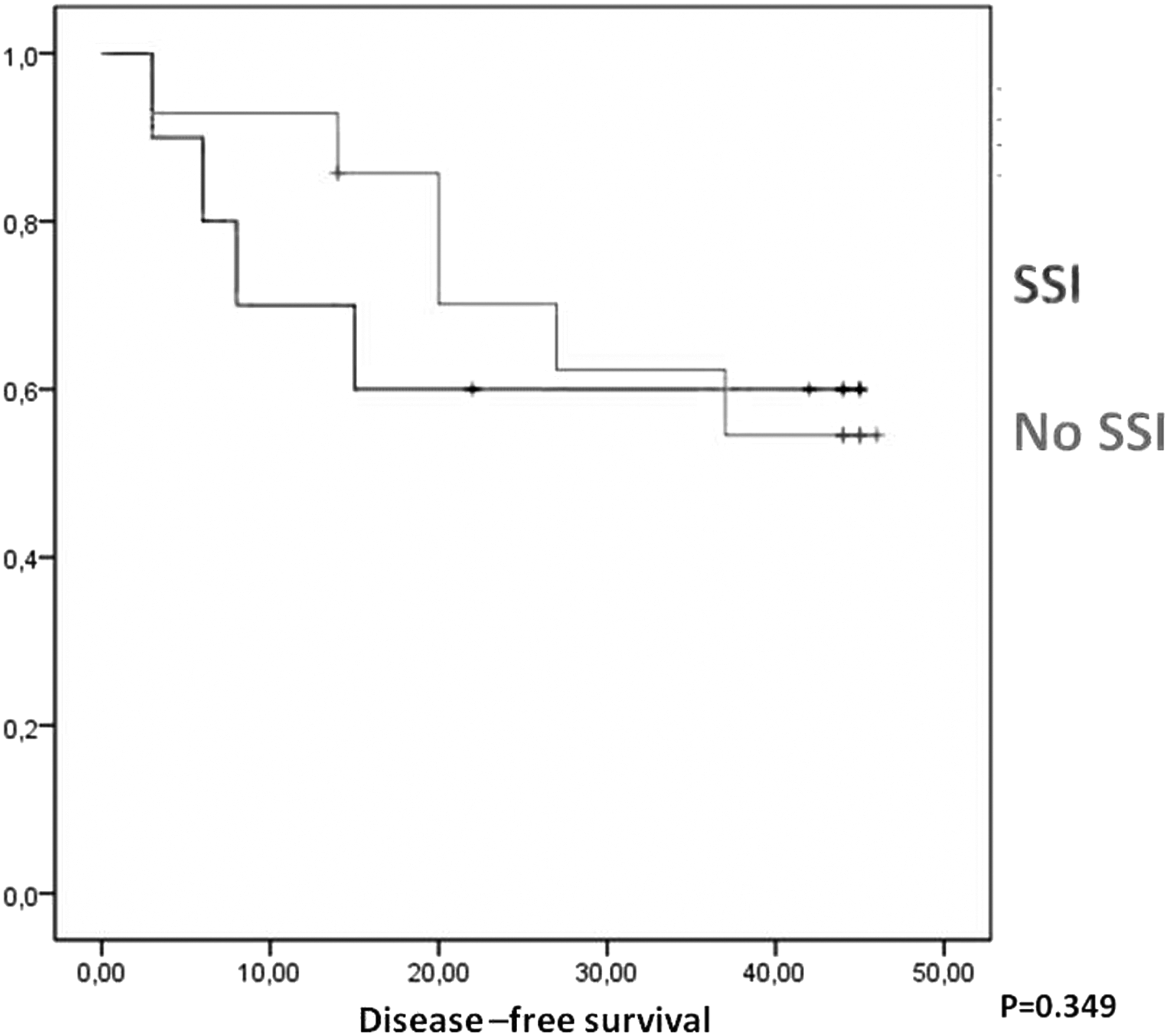
Disease-free survival associated to SSI.
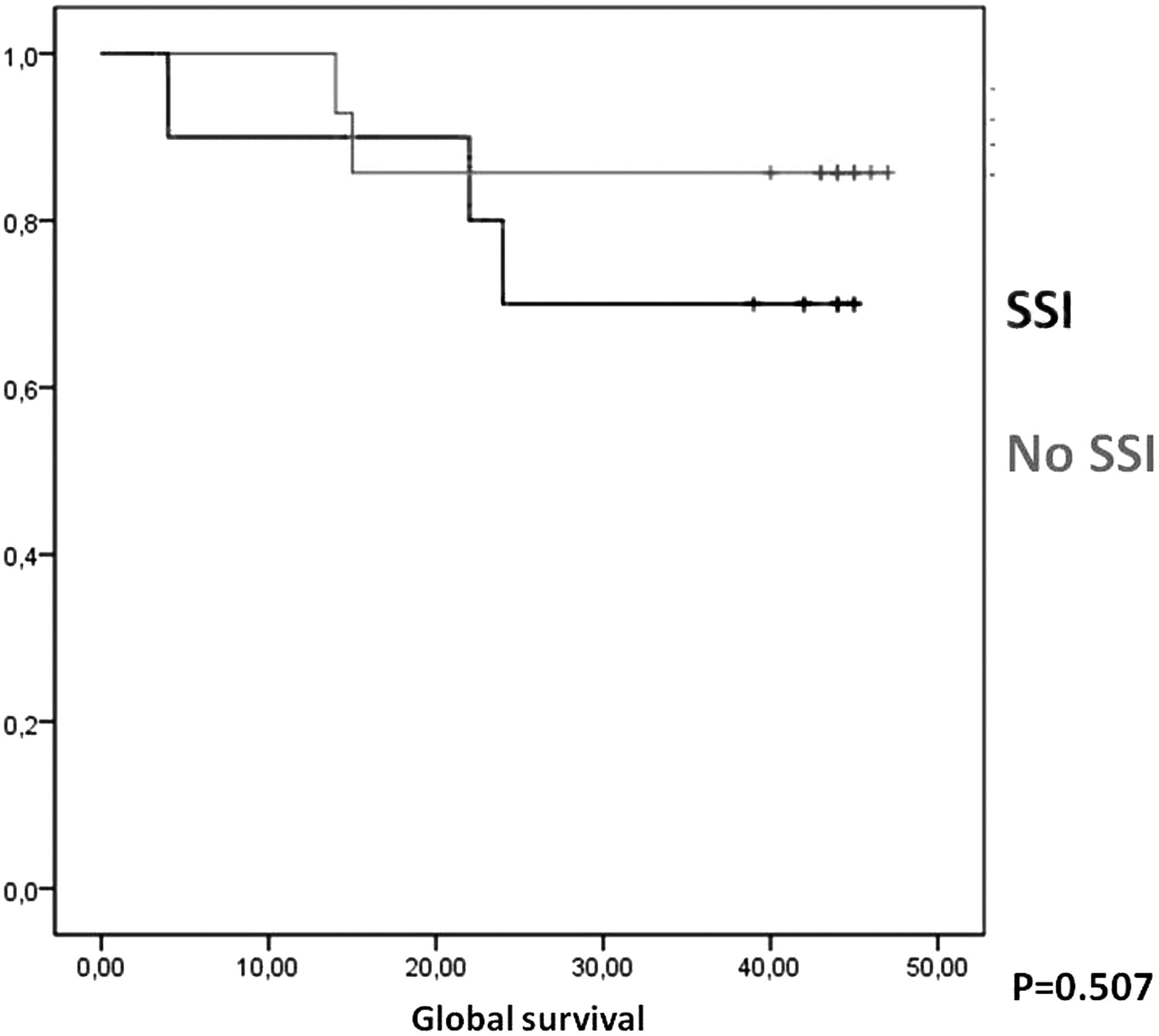
Global survival associated to SSI.
Discussion
The concept of lavaging a contaminated or infected peritoneal cavity makes good sense intuitively. However, because microbes adhere to mesothelial cells, it is difficult to wash them off the peritoneal surface. It has been demonstrated that bacteria that adhered to the mesothelium were resistant to intra-peritoneal lavage, resulting in only transitory reductions of bacterial populations. The results obtained after antibiotic lavage defend the hypothesis that the topical effect of the antibiotics could completely inhibit the growth of bacteria in the peritoneum, even when microorganisms have adhered to the mesothelial cells [8–11].
A similar effect can occur with the neoplastic cells. Antibiotics might present certain anti-neoplastic properties. Gentamicin is the most widely investigated antibiotic for anti-neoplastic effects. It belongs to the aminoglycosides group, which acts joining the ribosoma subunits 30S and 50S and blocking the translation of bacterial mRNA in the initial phase of protein synthesis, originating non-functional proteins. It has been hypothesized that it may act similarly in neoplastic cells [12,13]. Several in vitro studies have demonstrated a cytostatic effect of gentamicin, specially in epithelial cells [14]. Bossa et al. tested gentamicin against mice bearing Ehrlich ascites carcinoma, obtaining antitumoral activity [15]. As all our patients presented colorectal adenocarcinoma, an anti-tumoral effect could be attributed to gentamicin irrigation.
To our knowledge, an anti-neoplastic effect has not been previously attributed to clindamycin. However, as we used a combination of both agents, it is impossible to know if the anti-neoplastic effect depends only on gentamicin, if clindamycin also has a certain action, or if the combination enhances or reduces the effect. Several antibiotic agents, such as metronidazole, present an immunomodulating effect. This property justifies its use in Crohn disease, reducing the inflammatory response [16].
Probably, the antibiotic irrigation might not only act as a cytostatic agent against tumoral cells, but it can also modulate the inflammatory response against the surgical aggression, reducing the immunocompromised stage. Despite the already mentioned immunomodulating effect of metronidazole, we discarded its use in the peritoneal lavage, because this antibiotic was employed in the systemic antibiotic prophylaxis. The use of the same agent in the peri-operative systemic prophylaxis and in the intra-peritoneal lavage probably would not add any benefit. Moreover, clindamycin resistance spectrum is not as high in Spain as in other countries. Thus, we decided to use clindamycin in the peritoneal lavage.
Although in our patients, the global or disease-free survival was not associated with the development of post-operative SSI, a certain association between the anti-bactericidal effect and the oncologic outcome might be present. In our previously related publication of SSI after antibiotic lavage [6], we observed that bacterial contamination was present in 59% of the patients undergoing lavage with normal saline. Notwithstanding, the incisional SSI rate was 14% and organ-space SSI rate 6%. That means that at least 39% of patients with bacterial contamination did not develop SSI, showing that the immunological defenses could control the inoculums. This might reveal that the immunologic defense is focused on controlling the septic focus, leaving unattended other potentially threats (e.g., neoplasms), and this is not clinically relevant. In our opinion, the better oncologic outcome in those patients undergoing antibiotic lavage can be partly justified by the reduction in the post-operative SSI and consequently improved immunologic defense, but other parts of the anti-neoplastic effect can be possibly based on an intrinsic immunomodulating effect of the antibiotics administered. However, this is just a pilot study and large multi-center trials are necessary to confirm the results before the technique might be adopted.
Conclusion
The intra-peritoneal lavage with gentamicin and clindamycin increases the disease-free and global survival in colorectal tumors.
Footnotes
Author Disclosure Statement
Drs. Ruiz-Tovar, Gamallo, Santos, and Calpena, and Ms. Llavero declare that they have no conflict of interests in the elaboration of this manuscript.