
Abstract
Abstract
Background:
Adequate skin preparation is essential to preventing surgical site infection. Many products are available, each with specific manufacturers' directions. This lack of standardization may lead to incorrect use of the agents and affect the bacterial load reduction. We hypothesize that a lack of adherence to utilization protocols for surgical skin antiseptics affects bacterial load reduction.
Methods:
Thirty subjects who routinely perform surgical skin preparation were recruited from four hospitals. Participants completed a questionnaire of both demographics and familiarity with two of the most common skin prep formulas: Chlorhexidine gluconate-isopropyl alcohol (CHG-IPA) and povidone-iodine (PVI) scrub and paint. Randomly selecting one formula, subjects performed skin preparation for ankle surgery on a healthy standardized patient. This was repeated using the second formula on the opposite ankle. Performance was recorded and reviewed by two independent evaluators using standardized dichotomous checklists created against the manufacturer's recommended application. Swabs of the patients' first interweb space and medial malleolus were obtained before, 1 min after, and 30 min after prep, and plated on Luria Bertani agar. Bacterial loads were measured in colony forming units (CFUs) for each anatomical site. Data was analyzed using a univariate linear regression.
Results:
Subjects had an average of 12.7 ± 2.2 y operating room experience and 8.8 ± 1.5 y of skin prep experience. Despite this, no participant performed 100% of the manufacturers' steps correctly. All essential formula-specific steps were performed 90% of the time for CHG-IPA and 33.3% for PVI (p = 0.0001). No correlation was found between experience or familiarity and number of correct steps for either formula. Average reduction in CFUs was not different between CHG-IPA and PVI at 30 min for all anatomical sites (75.2 ± 5.4% vs. 73.7 ± 4.5%, p = 0.7662). Bacterial reductions at 30 min following skin prep were not substantially correlated with operator experience, protocol compliance, or total prep time for either formula.
Conclusion:
This study demonstrates existing problems with infection prevention as those tasked with pre-operative skin preparation do so with tremendous incongruence according to manufacturer guidelines. No effect on bacterial load was identified, however with a larger sample size this may be noted. Standardization of the prep solutions as well as simplification and education of the correct techniques may enhance protocol compliance.
H
At least 50% of HAIs are believed to be preventable [4,5]. Variations in sterile protocols in operating rooms (OR) to reduce SSI among healthcare providers are common and likely substantially influence the incidence of these infections [6]. Accordingly, future efforts to reduce HAIs should on reducing variations in techniques between healthcare workers (HCWs). One major area of focus is the appropriate usage of skin antiseptics to reduce HAIs related to surgery. Pre-incisional skin preparation with an antiseptic solution is crucial in preventing surgical HAI. ChloraPrep® (2% chlorhexidine and 70% isopropyl alcohol; CareFusion, Inc., Leawood, KS) is an alcohol-based skin preparation approved by the U.S. Food and Drug Administration that has become increasingly popular over the last two decades in the OR. Yet, despite clinical evidence favoring ChloraPrep, povidone-iodine based products such as ‘Scrub & Paint’ remain commonly used throughout the United States.
Given the wide variety of surgical prep agents available on the market, few studies to date have investigated the familiarity and compliance of HCWs who routinely perform surgical prep [7–9]. Thus, the aim of our study was to determine if there was a discrepancy in the standard practice of skin antiseptics and the industry-recommended practice based upon the type of modality used. The primary outcome of our study was to measure protocol compliance; additional outcomes measured were bacterial load after antiseptic application by experienced HCWs.
Patients and Methods
Materials
Two percent chlorhexidine gluconate/70% isopropyl alcohol (CHG-IPA) and povidone iodine (PVI) scrub and paint were provided by CareFusion. CHG-IPA is a sterile single-use device comprising a breakable glass vial of liquid within a plastic/sponge applicator. The PVI product is a multi-compartment sterile stray with several sponges and two 59-mL bottles of iodine-based solution. A detergent-containing additive is applied first and blotted followed by a diluted povidone iodine solution that is air-dried.
Study location
A simulated OR at the Tulane Center for Advanced Medical Simulation and Team Training (New Orleans, LA) was used for the study. Institutional Board Review approval was obtained from Tulane University before initiating this study.
Study participants
Thirty standardized patients with no pre-existing medical conditions were recruited from the general population. Exclusion criteria were the use of topical or oral antimicrobial agents 14 d prior to testing in accordance with the ASTM Standard Test Method for Evaluation of Preoperative, Precatheter or Preinjection Skin Preparations [10] or a known allergy to either skin preparations. Thirty HCWs who routinely perform surgical skin preparation as part of their daily job were recruited from four area hospitals. Participants were required to have prior experience in surgical prep with both CHG-IPA and PVI prep modalities. A pre-procedure demographic and experience survey was administered to all participants. Subjects received no instruction regarding the specific use of either modality prior to study participation.
Surgical site skin preparation
Standardized patients were positioned supine with both legs exposed below the knee. Subjects were instructed to prepare the one of the two lower extremities for a below knee amputation, including the full pre-operative procedure including skin antisepsis and placement of sterile drapes to minimize the Hawthorne effect. The choice of prep was randomly chosen to avoid selection bias. Upon completion of this procedure, the procedure was repeated using the other type of skin prep on remaining lower extremity. Subjects received no instruction regarding the specific use of either modality prior to prepping. Each subject performed skin preparation on only one standardized patient to minimize the confounding parameters of patient body habitus and baseline bacterial load, thus focusing analysis on the performance of the healthcare worker and the utility of the prep modalities in reducing bacterial load. This protocol reflects that employed by Saltzman et al. [11].
Performance assessment
All skin preparation performances were observed directly via two-way mirror, and audio and video were recorded for retrospective review. Performance was graded by two independent evaluators using standardized dichotomous checklists created by the manufacturer. Critical steps were identified by investigators as they specifically relate to the contact of the prep material on the surgical site. These steps are highlighted in Figure 1.
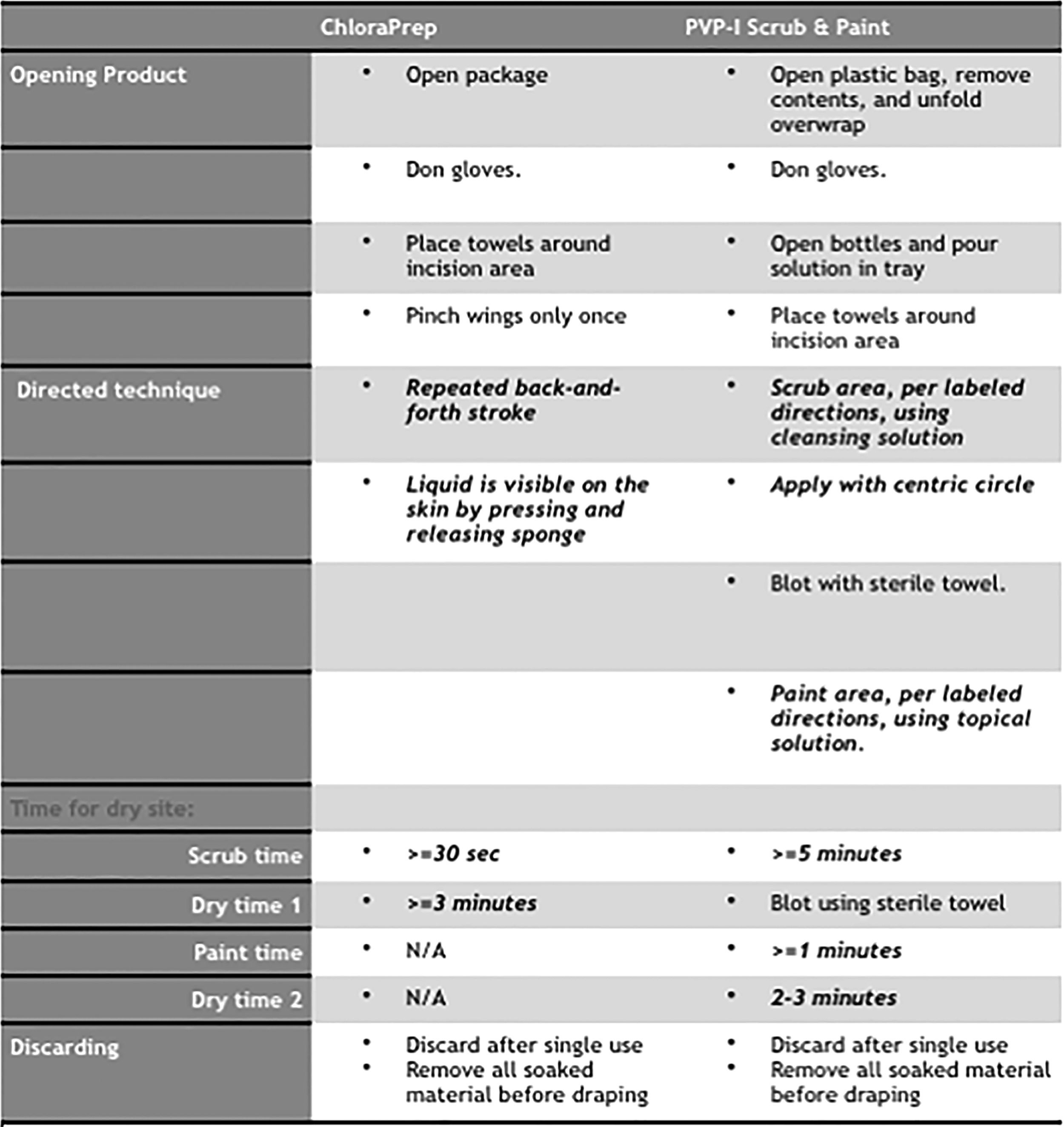
Dichotomous manufacturer's checklist for surgical skin preparation with chlorhexidine gluconate/isopropyl alcohol and povidone-iodine scrub and paint. Critical steps are bolded and italicized.
Bacterial load quantification
The first interweb space and medial malleolus of both feet were swabbed with a sterile cotton tip applicator for 10 sec and plated on Luria Bertani (LB) agar at three different intervals (prior to skin prep, 1 min after, and 30 min after prep) in triplicate. The site of skin prep was covered with a sterile towel between sampling. LB agar plates were incubated at 37°C for 24 h and bacterial colony forming units (CFUs) were enumerated by a single standard operator blinded to skin prep modality and anatomical site.
Data analysis
All data are presented as mean±standard error of the mean unless otherwise indicated. A Student t-test was used to analyze continuous variables and a Fisher exact test for categorical variables. One way analysis of variance (ANOVA) was used to compare multiple sets of data. Pearson correlation coefficients were calculated from linear plots with provider experience as the independent variable for the combined data for both preps. A p value < 0.05 was considered to be statistically significant. Data analysis was performed using GraphPad software (version 5; San Diego, CA, USA).
Results
Baseline demographic information
Subjects enrolled in this study were 25 nurses and five surgery residents with an average of 12.7 ± 2.2 y experience in the OR and 8.8 ± 1.5 y with skin preparation. Baseline demographic information for study participants is shown in Table 1.
SEM = standard error of the mean.
Study performance
Study performance data is presented in Table 2. No subject completed all of the manufacturer's recommended steps for the PVI preparation, whereas 16.7% (n = 5/30) completed all recommended steps with CHG-IPA (p = 0.027). Compliance with critical steps was greater with CHG-IPA, with 90% (n = 27/30) completing all critical steps and 33.3% (n = 10/30) for PVI preps (p = 0.0001). No subject completed the manufacturer recommended total prep time of 300 sec for PVI with an average of prep time of 102.9 ± 1.2 sec. However, all participants scrubbed with CHG-IPA for longer than the manufacturer recommended 30 sec with an average prep time of 84.9 ± 1.1 sec. Breaks in sterile technique were commonly observed but not substantially different between preps, occurring 26.7% for CHG-IPA preparations (n = 8/30) and 36.7% (n = 11/30) for PVI preparations (p > 0.05).
CHG/IPA = chlorhexidine gluconate-isopropyl alcohol; PVI = povidone-iodine.
Skin bacterial load quantification
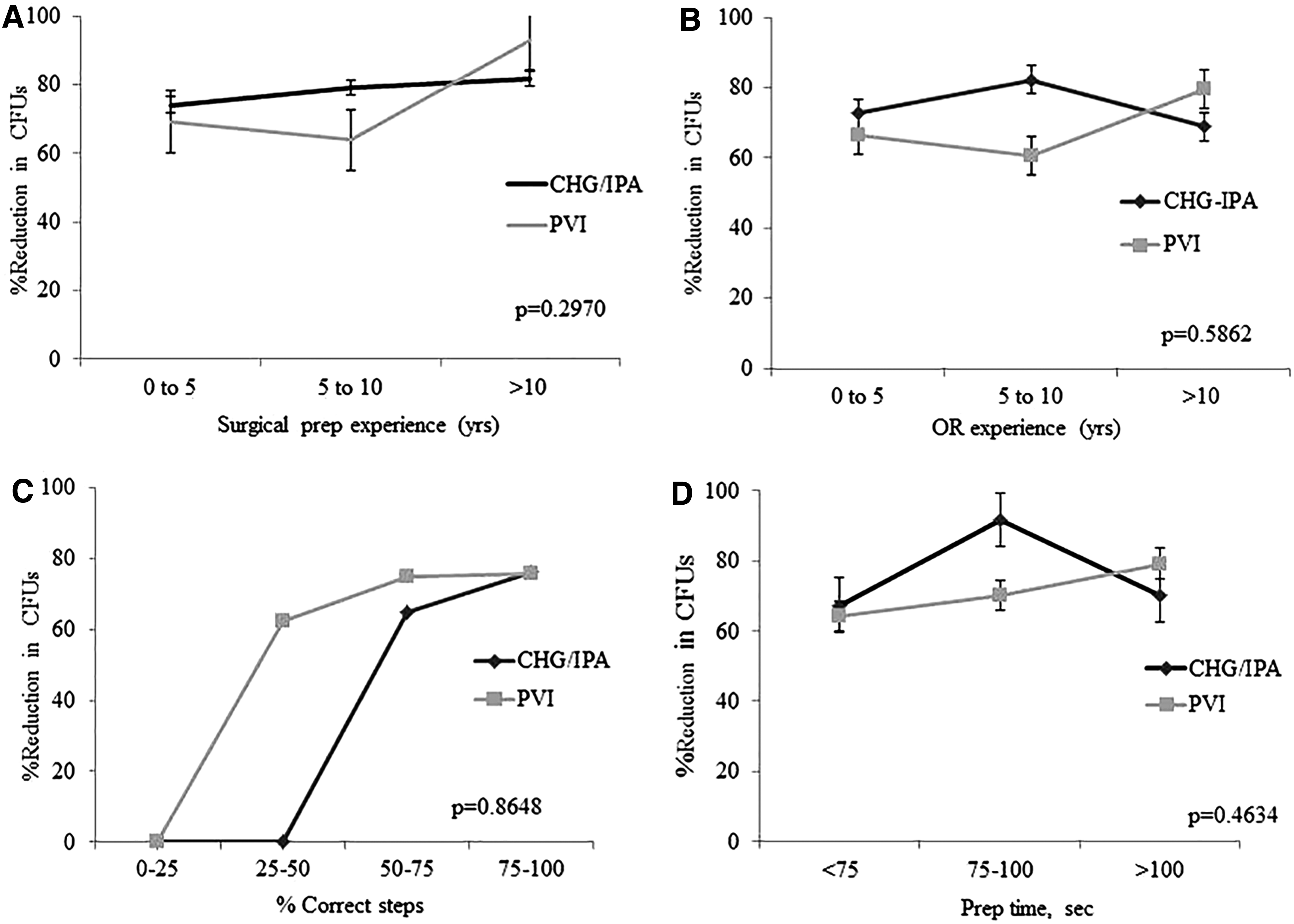
Average bacterial CFU counts are shown in Table 3. No statistically significant difference was found between CHG-IPA and PVI (p > 0.05). All sites showed a reduction in CFUs 30 min after preparation, neither agent reliably reduced bacterial burden to zero. The decrease in CFUs at 30 min between CHG/IPA and PVI also did not differ substantially based on years of prep experience, OR experience, percentage of correct steps, or total prep time (p 0.2970–0.8648) as shown in Figure 2. A linear correlation of subject experience for both types of surgical preps revealed that increased experience with surgical skin preparation did not affect compliance or reduction in skin bacterial counts (Fig. 3).
Percent reduction in bacterial CFUs 30 min after prep vs. surgical prep experience
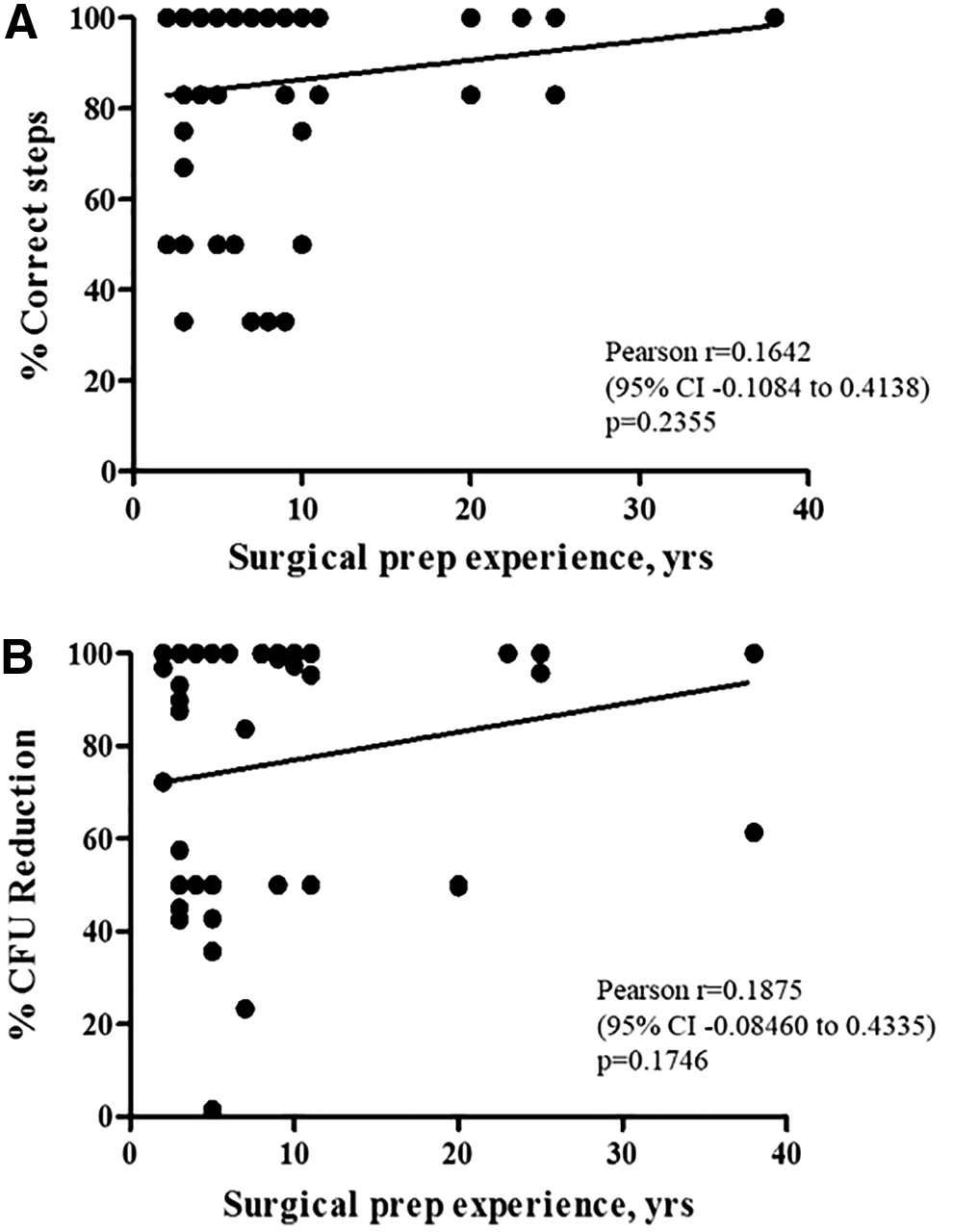
Linear correlation comparing healthcare provider experience level to protocol compliance for
CHG/IPA = chlorhexidine gluconate-isopropyl alcohol; CFU = colony forming units; PVI = povidone-iodine.
Discussion
Surgical site infections (SSI) pose an enormous financial burden on the US healthcare system and routinely complicate patient outcomes after surgery [12,13]. HCWs have a critical role in reducing these infections. Previous studies have addressed which type of surgical prep provides the most optimal outcomes [9,11,14,15]. However, only a few studies have addressed the effect of HCW protocol adherence when performing surgical prep [7–9]. This study was the first to our knowledge that specifically addresses the role this plays on preoperative antisepsis. We found that the majority of experienced HCWs who routinely perform preparation of surgical sites did not correctly adhere to the recommended steps. We also observed that protocol adherence decreased based upon the complexity of the surgical prep. Experience level was not found to correlate with greater protocol adherence or decreased skin bacterial counts.
The majority of previous investigations on surgical prep have focused on which product provides the best outcomes. The current consensus in the literature favors CHG-IPA when compared with PVI [9,11,14,16]. However, it is unknown what role provider compliance plays in product effectiveness. A previous study by Magalini et al. proposed that CHG-IPA offered easier and faster preparation, which could contribute to its improved performance compared with PVI [9]. This conclusion is similar to our study results as we found that all participants scrubbed for the minimum recommended prep time of 30 sec with CVG-IPA, but none of the participants completed the recommended prep time of 5 min with PVI.
There is a dearth of medical literature focused on the quality of surgical prep performed by HCWs in the OR. Similar to our results, a previous study by Sullivan et al. found that surgeon experience level did not affect the quality of surgical prep [7]. A study by Sessa et al. determined that nurse education level positively correlated with knowledge of proper surgical prep techniques. They found that 62.6% of nurses self-reported appropriate disinfection procedures for surgical incisions [8].
There are several limitations to our study. Our small sample size was a limiting factor in the power of the study. However, it is likely that our results could be generalizable to the healthcare profession, which could be confirmed by larger studies. Power is also a limiting factor in comparing the performance of surgical residents (n = 5) to OR personnel. The absence of a substantial difference between these two groups obviated its inclusion in our results, though a study with larger number of residents may be able to demonstrate a substantial effect relative to profession. Another potential issue was the observational nature of this study. Although we did attempt to minimize the Hawthorne Effect within our study design, it is likely that this still influenced the results as subjects were aware they were being monitored. However, subjects still do not perform well despite being watched, which is also an interesting conclusion. Finally, another potential limitation of this study is our use of “critical steps” determined by the senior author. Surgical preps are required by the Food and Drug Administration to list sequential steps for use. However, we believe that some of these steps are not necessary to the performance of the prep and we attempted to control for this by examining operator compliance with steps that are critical for performance of surgical prep.
Conclusions
Our study demonstrates a lack of protocol compliance by experienced HCWs when performing preoperative antisepsis. Compliance was found to be improved when performing “critical” steps. No correlation was found between level of experience with protocol compliance or reduction in the skin bacterial burden. These results suggest that protocol compliance could be improved with simplified instructions. Further studies are needed to help design targeted interventions at the level of healthcare providers which will reduce the incidence of SSI.
Footnotes
Author Disclosure Statement
The authors disclose that the funding for this research was provided by an investigator-initiated grant by CareFusion.