
Abstract
Abstract
Background:
Doripenem is approved by the Food and Drug Administration for the treatment of patients with complicated intra-abdominal infections and complicated urinary tract infections. While studies have described the pharmacokinetics/pharmacodynamics (PK/PD) of doripenem in the critically ill, no study has described the probability of target attainment profile among trauma patients with sepsis.
Patients and Methods:
This study was a prospective, open-label, pharmacokinetic study in the surgical intensive care unit (SICU) at Grady Health System. Thirty trauma patients with sepsis admitted to the SICU received doripenem 1 g infused over 4 hours every 8 hours for three doses. Blood samples were taken just before and after the third dose. A two-compartment model was fit to the data using non-parametric population PK modeling software. Embedded with the final PK model, a Monte Carlo Simulations (MCS) was performed to determine the PK/PD profile of doripenem 1 g, infused over 4 hours, every 8 hours after administration of the first and fourth doses.
Results:
Overall, the model fit the data well, and mean (standard deviation) clearance and volume of the central compartment were 16.9 (11.4) L/h and 28.5 (16.0) L, respectively. In the MCS analyses, doripenem 1 g, infused over 4 hours, administered every 8 hours, conferred >90% probabilities of achieving 30–50% time greater than the minimum inhibitory concentration (30–50% T>MIC) for MICs ≤2 mg/L after infusion of both the first and fourth doses. The MCS indicated that more intensive doripenem dosing schemes should be considered for organisms with MIC values in excess of 2 mg/L.
Conclusions:
This is the first study to describe the doripenem PK/PD in critically ill patients with trauma. Among these patients, the MCS analyses suggest that current dosing strategies may be ineffective when the MIC value for the infecting pathogen is expected to be above 2 mg/L.
D
For critically ill patients with trauma, it is especially important to maximize the PK/PD profile. Critically ill patients are highly vulnerable to infections with gram negative bacteria with high MIC values, and published data suggest that these patients often require more intensive dosing schemes because of their altered physiology [7–9]. Although critically ill trauma patients tend to be younger and have fewer comorbidities, they are often hypermetabolic and are frequently administered aggressive fluid resuscitation resulting in increased renal clearance of drugs and larger volumes of distribution [7,9]. Thus, it is often difficult to reliably achieve critical PD targets, such as fT>MIC, with standard dosing regimens in critically ill patients with trauma.
Although other studies have evaluated the PK/PD of doripenem in the critically ill, there are no studies to date describing the PK/PD in the critically ill trauma population with sepsis [3–5]. The primary objective of this study is to evaluate the PK and PD of doripenem in a population of critically ill trauma patients with sepsis. As part of this examination, we examined the probability of target attainment (PTA) profile after the first and fourth doses to determine the need for loading doses in this population.
Patients and Methods
This was a prospective, open-label, steady-state pharmacokinetic study of critically ill trauma patients with sepsis. Patients were recruited from Grady Health System (Atlanta, GA), a level I trauma center. Inclusion criteria were: age ≥18 years, admission to the Emory surgical intensive care unit (SICU) service for greater than 24 hours, and a diagnosis of sepsis that necessitated empiric antimicrobial therapy [10]. Patients were excluded from the study if they had acute or chronic renal dysfunction (urine output less than 0.5 mL/kg/h or calculated creatinine clearance (CL
The study was approved by the Institutional Review Board (IRB), and written informed consent was obtained from the patient or a legally authorized representative (LAR) if the patient was unable to give informed consent because of his or her medical condition before initiation of any study procedure. Verbal consent was obtained in patients with IRB permission in special circumstances when the LAR was unable to physically come to the hospital to provide written informed consent.
Interventions and measurements
Patients received doripenem 1000 mg every 8 hours over 4 hours for three doses. Blood samples were collected from an indwelling intravenous catheter immediately before initiation of the third dose (time 0), and 5, 6, and 8 hours after the start of the third dose infusion. All blood samples were collected in non-anticoagulant (red-top) tubes. The samples were allowed to clot, and the serum was obtained by centrifugation within 15 minutes of collection. The serum samples were stored at –70°C until assayed by a validated high performance liquid chromatography methodology with a correlation coefficient of ≥0.998, slope of 0.0575 ± 0.0037 (mean ± standard deviation [SD]), and intercept of 0.0013 ± 0.0057 (mean ± SD) [12]. After completion of the 24-hour study period, doripenem was discontinued, and patients were administered the standard SICU empiric antibiotic of choice.
Data collection
The following data points were collected for each patient: demographic information (age, gender, and weight), allergies, serum creatinine (SCr), CLCR, temperature, heart rate, respiratory rate, white blood cell count, Sequential Organ Failure Assessment (SOFA) score, Injury Severity Score (ISS), hospital length of stay (LOS) before study enrollment, exact time of blood withdrawals in relation to dose administration.
Pharmacokinetic data analysis
All data were analyzed in a population PK model by use of big non-parametric adaptive grid (BigNPAG) [13]. The PK model was parameterized as a two-compartment model with zero-order infusion and first-order inter-compartmental transfer and elimination. The inverse of the estimated assay variance was used as the first estimate for weighting, and the analysis was performed with adaptive gamma. On attaining convergence, Bayesian estimates for each patient were obtained using the “population of one” utility within BigNPAG.
Mean, median, and modal values were used as measurements of the central tendency of the population parameter estimates and were evaluated in the maximum a posteriori probability (MAP) Bayesian analysis. Scatter plots were examined for individual patients and the overall population. Goodness of fit was assessed by regression with an observed versus predicted plot, coefficients of determination, and log-likelihood values. Predictive performance was based on weighted mean bias and bias-adjusted weighted mean precision.
Post hoc exploratory analyses were completed to examine the relations between individual Bayesian-posterior doripenem clearance estimates and estimates of renal function using several different equations. The renal function estimates included: CL
Monte Carlo Simulation (MCS)
Embedded with the final population PK model, a 5000-subject MCS using ADAPT 5 was performed for a prolonged 4-hour infusion of doripenem 1000 mg administered every 8 hours for four doses [20]. The population simulation without process noise option was used, and log-normal distributions of PK parameters were selected. The fractions of simulated subjects who achieved 30%, 40%, and 50% T>MIC were calculated for the range of doripenem MICs from 0.25–8 mg/L. Because early appropriate therapy is a key determinant of clinical outcomes for patients with serious infections, this analysis focused on the probabilities of achieving 30–50% T>MIC after the first dose (hours 0–8 post-initial dose) and fourth dose (hours 24–32 post-initial dose) [21,22].
The MCS was also used to evaluate the predictive performance of the final population PK model. We simulated the prolonged 4-hour infusion of doripenem 1000 mg administered every 8 hours for four doses using the mean parameter vector values, then dispersed the patients’ data points around the simulated points. The fidelity by which the concentration-time curves mirrored the raw data was assessed by visual inspection.
Results
Thirty patients were enrolled between May 2010 and June 2011, and data were collected and evaluable for 27 patients. Baseline data are provided in Table 1. The study cohort was predominately male (81%), and the mean (SD) age was 43.6 (15) years. Nearly 90% of patients were receiving mechanical ventilation, and the average CLCR was 135.1 mL/min. The mean (SD) SOFA score was 5.2 (1.8), and the average (SD) LOS in the ICU before enrollment was 35.3 (39.5) days.
SD = standard deviation; No. = number; ISS = Injury Severity Score; SOFA = Sequential Organ Failure Assessment; CL
Population pharmacokinetic analysis
The mean (SD) population parameter estimates identified by BigNPAG are shown in Table 2. The predictive performance of the PK model after the Bayesian step is displayed in Table 3. Using the population mean parameter values as the measure of central tendency, the overall fit of the model to the data was good, and the observed-predicted plots were highly acceptable.
SD = standard deviation; Vc = volume of the central compartment; CL = clearance of the central compartment; kcp = microtransfer rate constant from the central to the peripheral compartment; kpc = microtransfer rate constant from the peripheral to the central compartment.
Best-fit regression for the observed-predicted plot after the Bayesian step.
Coefficient of determination for the best-fit linear regression line for the observed-predicted plot after the Bayesian step.
The simulated concentration-time serum curve from the mean parameter vector values from the final population PK model for doripenem 1000 mg, infused over 4 hours, administered every 8 hours is shown in Figure 1. As shown in Figure 1, the raw data points from study subjects are generally evenly dispersed around the simulated concentration-time curve. Most importantly, as doripenem is a characteristic T>MIC antibiotic, doripenem concentrations at the midpoint and end of the dosing interval were well captured around the central tendency.
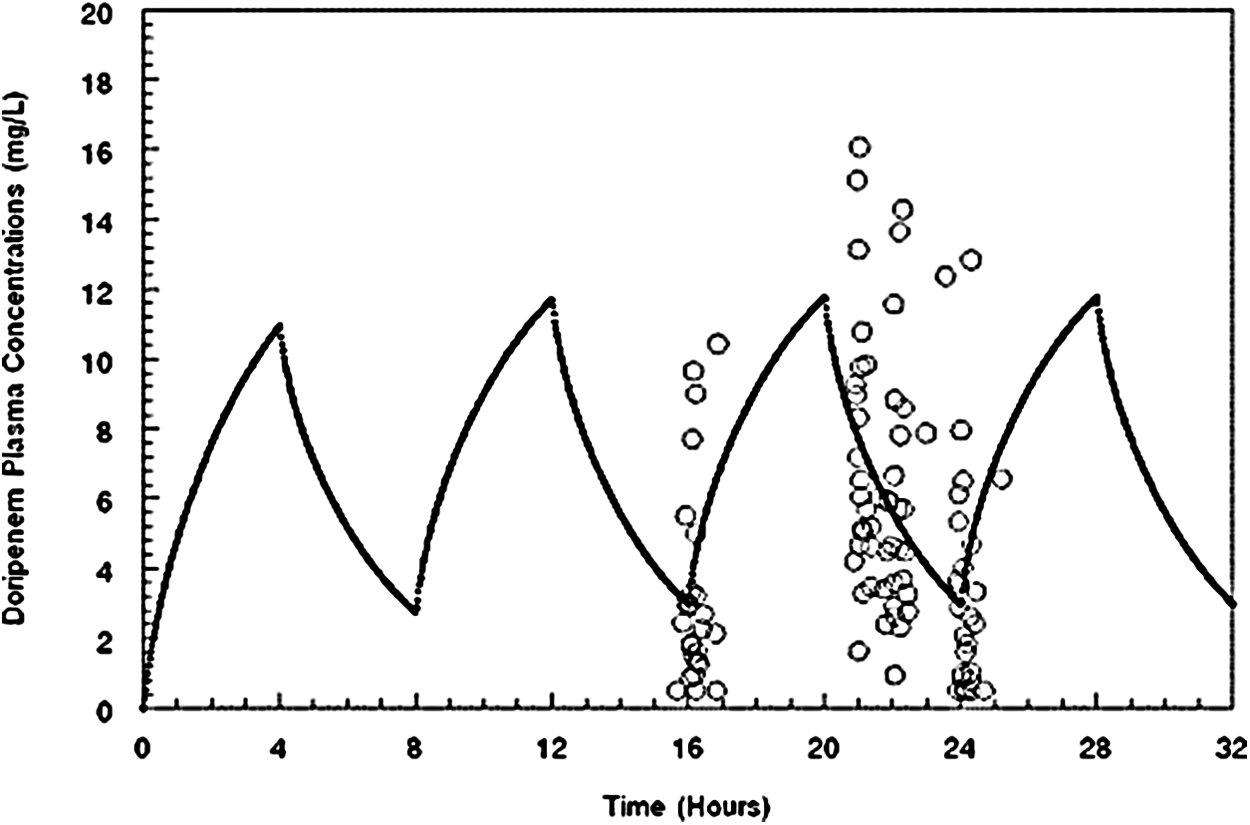
Concentration-time profile of doripenem 1 g administered every 8 hours as a 4-hour infusion as calculated from the mean parameter vector. Empty circles are observed concentrations from critically ill patients with sepsis.
The relations between individual Bayesian-posterior doripenem clearance estimates versus different renal function equation-based estimates are displayed in Figures 2A–E. No demonstrable relations were noted between the individual Bayesian-posterior doripenem clearance estimates and the different renal function equation-based estimates. In the regression analyses, the R2 ranged between 0.07 and 0.21 for all comparisons. As shown in Figures 2A–E, the individual Bayesian-posterior doripenem clearance estimates were also similar for the patients with an estimated renal function estimate >130 mL/min relative to those with an estimated renal function estimate <130 mL/min.
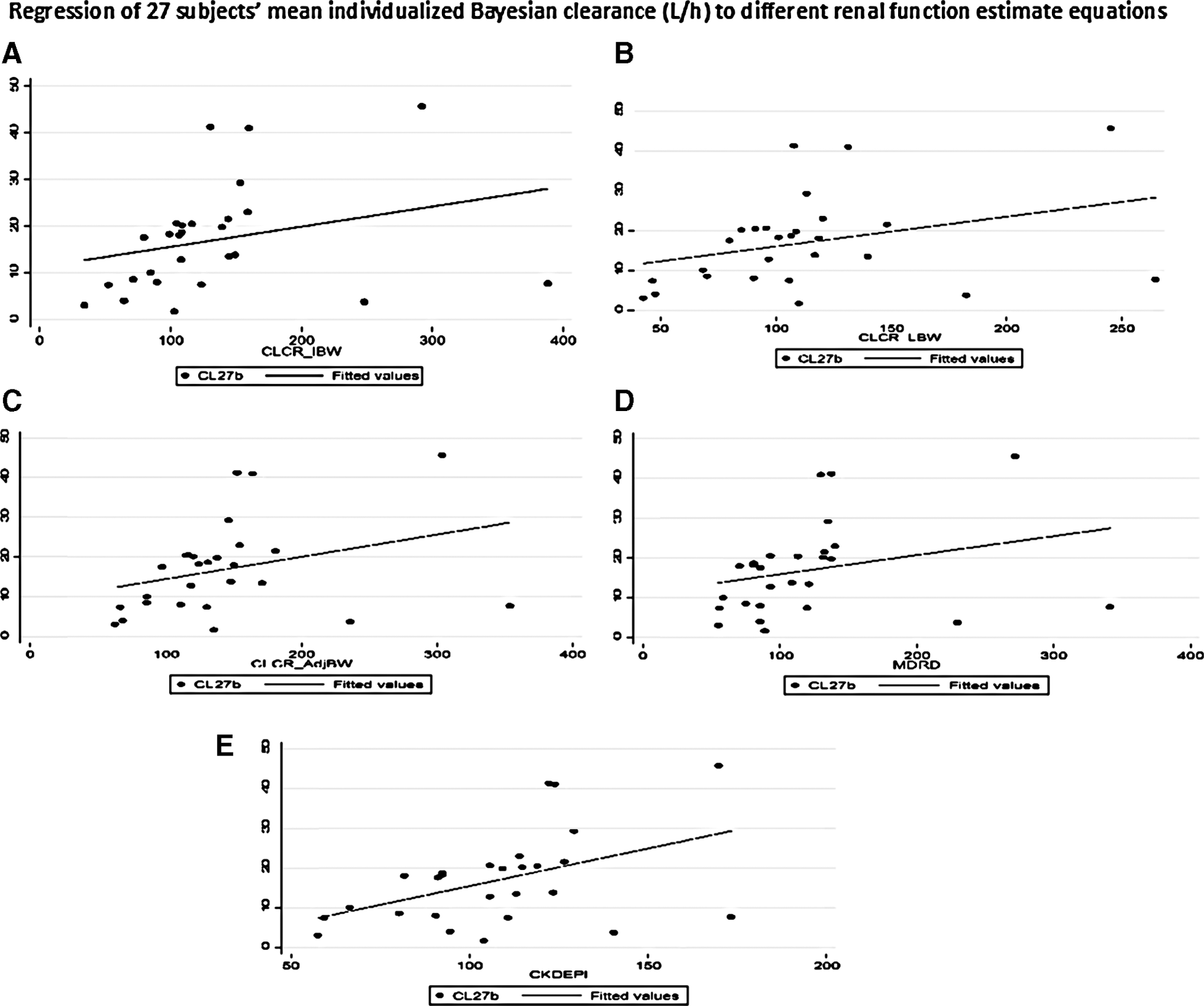
Regression of 27 subjects’ mean individualized Bayesian clearance (L/h) to different renal function estimate equations. (
Probability of target attainment analysis
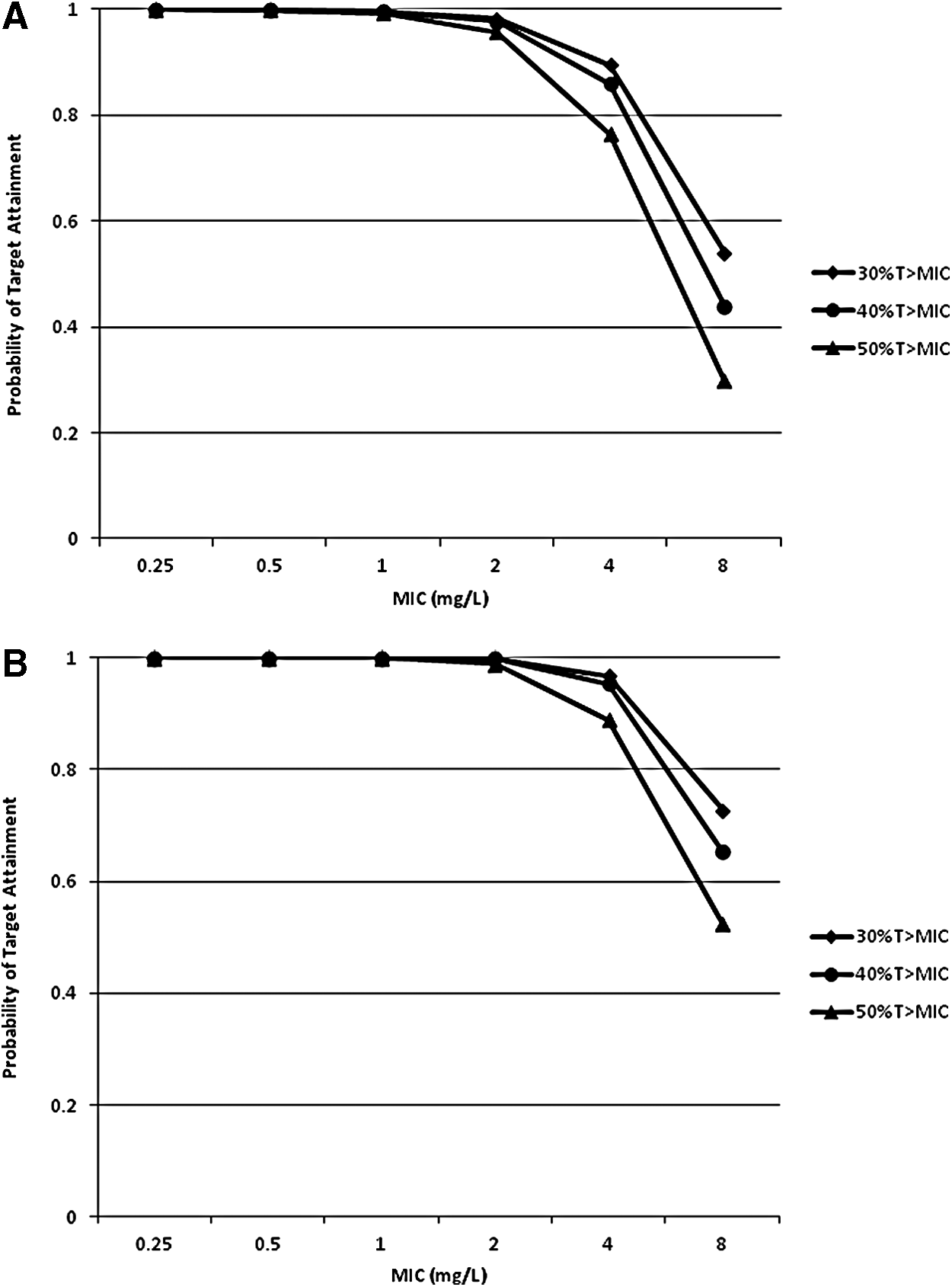
The PTA analyses are displayed in Figures 3A and 3B. With the first dose simulations (Fig. 3A), the probability of achieving 30–50% T>MIC exceeded 95% for MIC values ≤2 mg/L (range of MIC values considered susceptible by Clinical and Laboratory Standards Institute, or CLSI). At an MIC value of 4 mg/L, the probability of achieving 30% T>MIC was 90% while the probabilities of achieving 40% and 50% T>MIC were 86% and 76%, respectively. The probability of achieving 30–50% T>MIC was less than 60% at an MIC value of 8 mg/L.
(
A modestly improved PTA profile for doripenem 1 g, infused over 4 hours, administered every 8 hours, was observed after the fourth dose (Fig. 3B). Similar to the first dose simulations, the probability of achieving 30–50% T>MIC exceeded 95% for MIC values ≤2 mg/L. Subtle improvements in the PTA profiles between the first and fourth dose simulations were noted at MIC values of 4 and 8 mg/L. The probabilities of achieving 30–50% T>MIC, however, were still less than 80% at an MIC of 8 mg/L with the fourth dose simulations.
Discussion
The primary objective of this study is to characterize the PK/PD profile of doripenem in a population of critically ill trauma patients with sepsis. These data are timely given the suboptimal outcomes observed with doripenem relative to imipenem among patients with augmented renal function, a population highly consistent with our study cohort, in the recent ventilator-associated pneumonia (VAP) randomized clinical trial [23]. Overall, there were several notable findings in this investigation. Compared with studies conducted in healthy volunteers, higher mean estimates of clearance and central volume of distribution were noted in this study. The elevated clearance among trauma patients is most likely related to their augmented renal function; the higher volume of distribution is likely because of the administration of aggressive fluid resuscitation for sepsis.
Our mean estimates and coefficients of variation for volume and clearance aligned closely with several other studies conducted in medical ICUs among patients with documented infections and augmented CL
NPNA = nosocomial pneumonia; VAP = ventilator associated pneumonia; CUTI = complicated urinary tract infection.
All data presented as mean (standard deviation) unless otherwise noted.
Although the highly variable estimates of clearance and volume of distribution observed suggest that therapeutic drug monitoring may be warranted in this patient population, the MCS analyses indicate that doripenem 1 g, infused over 4 hours, administered every 8 hours, had a highly favorable PTA profile against the range of MIC values considered susceptible by CLSI. Given recent data suggesting that loading doses are needed for prolonged beta-lactam infusions, we evaluated the PK/PD profile after the first dose (hours 0–8 post-initial dose) and at steady state conditions (hours 24–32 post-initial dose). As shown in Figures 3A and 3B, the probabilities of achieving 30–50% T>MIC exceeded 90% for MIC values ≤2 mg/L. Modest differences in the PTA profiles were noted at an MIC value of 4 mg/L, and both were suboptimal at an MIC value of 8 mg/L.
From a PK/PD perspective, the similar PTA profiles between first dose and steady-state simulations are not surprising. A loading dose serves a two-fold purpose: (1) to rapidly achieve concentrations that mimic concentrations at steady-state conditions and (2) to maximize total exposure (e.g., maximum serum concentration and area under the curve) at the onset of therapy. These are not critical concerns for short half-life drugs such as beta-lactams where the interest is maintaining T>MIC for as long as possible during the dosing interval (e.g., time-dependent activity). Loading doses are only required for antibiotics with long terminal half-lives and whose bactericidal activity is concentration-dependent. Further, even though overall clearance is generally higher among trauma patients with sepsis, the half-life is often prolonged because of their elevated volumes of distribution. As clearance = volume of distribution × Ke and half-life = 0.693/Ke, the net effect of this is similar PK/PD profiles with the first and fourth doses.
Although the MCS data are reassuring, there are several things to consider. First, the favorable PTA profile was only observed for MIC values ≤2 mg/L. In clinical practice, it is not uncommon to encounter an infection from a gram negative organism with a doripenem MIC value in excess of 2 mg/L. Given the rising rates of resistance across many gram negative pathogens, many clinicians are often required to use antibiotics for organisms with MIC values in excess of the susceptibility breakpoints [24–34]. In these circumstances, it would be prudent to consider the risk versus benefit of empirically using more intensive doripenem dosing schemes than the one evaluated in this study.
Second, these simulation studies focused on concentrations in the blood stream. Blood stream concentrations are not always indicative of concentrations at the site of infection, particularly for infection involving the lower respiratory tract [35]. For doripenem, the median epithelial lining fluid/plasma penetration ratio among patients with VAP is only ∼30% [36]. Because the critical drug-pathogen interaction is the same regardless of the site of infection, the only way to achieve a favorable T>MIC profile in the lower respiratory tract with doripenem is to again consider the risk versus benefit of administering a higher doripenem dose (>1 g) over prolonged periods [37,38].
This PK/PD study focused on PD targets associated with maximal bacterial killing and clinical success [37,38]. The next frontier in PK/PD is identifying antibiotic dosing schemes and drug combinations that minimize the emergence of resistance [39]. The existing data suggest that PD targets that prevent resistance to carbapenems are typically 2–4-fold higher than PD targets for success [40–43]. Further study is still needed in the area of resistance suppression, but the current data suggest that obtaining the PK/PD target against the range of MICs encountered clinically is not likely with the doripenem dosing scheme examined in this analysis and that more intensive dosing schemes will be required. Another limitation to note is that the CL
Last, this study was completed in a critically ill patient population that required a sparse sampling approach. Four blood samples were acquired that included measurement before initiation of the third dose (time 0), and 5, 6, and 8 hours after the start of the third dose infusion. Although a more robust sampling scheme with collections during infusion would have been preferred, we chose to better characterize the elimination phase of this time-dependent antimicrobial. This was important, because our objective was to determine the probability of time above the MIC. Ultimately, the PK/PD profile of time-dependent beta-lactam antibiotics is driven by the elimination phase because of the short half-life.
Conclusions
The current study demonstrates that, as expected, critically ill patients with trauma have higher clearance rates and volumes of distribution for doripenem compared with healthy volunteers. Moreover, because of such drastic alterations in the PK in this population, 1 g doses infused over 4 hours and administered every 8 hours are required to achieve reliably the PD targets associated with maximal bactericidal killing for gram negative pathogens with MIC values considered susceptible by CLSI. If pathogens with higher MICs (>2 mg/L) to doripenem are encountered, or if the infection involves the lower respiratory tract, our data suggest that the risk versus benefit of using more intensive doripenem dosing schemes should be considered. Because this is a PK/PD study, all findings need to be evaluated prospectively in the clinical arena.
Footnotes
Author Disclosure Statement
This study was funded by Ortho McNeil Janssen Scientific Affairs