
Abstract
Abstract
Background:
Repair of large ventral hernia defects is associated with high rates of surgical site occurrences (SSO), including surgical site infection (SSI), site dehiscence, seroma, hematoma, and site necrosis. Two common operative strategies exist: Component separation (CS) with primary fascial closure and mesh reinforcement (PFC-CS) and bridged repair (mesh spanning the hernia defect). We hypothesized that: (1) ventral hernia repair (VHR) of large defects with bridged repair is associated with more SSOs than is PFC, and (2) anterior CS is associated with more SSOs than is endoscopic, perforator-sparing, or posterior CS.
Methods:
Part I of this study was a review of a multi-center database of patients who underwent VHR of a defect ≥8 cm from 2010–2011 with at least one month of follow-up. The primary outcome was SSO. The secondary outcome was recurrence. Part II of this study was a systematic review and meta-analysis of studies comparing bridged repair with PFC and studies comparing different kinds of CS.
Results:
A total of 108 patients were followed for a median of 16 months (range 1–50 months), of whom 84 underwent PFC-CS and 24 had bridged repairs. Unadjusted results demonstrated no differences between the groups in SSO or recurrence; however, the study was underpowered for this purpose. On meta-analysis, PFC was associated with a lower risk of SSO (odds ratio [OR] = 0.569; 95% confidence interval [CI] = 0.34–0.94) and recurrence (OR = 0.138; 95% CI = 0.08–0.23) compared with bridged repair. On multiple-treatments meta-analysis, both endoscopic and perforator-sparing CS were most likely to be the treatments with the lowest risk of SSO and recurrence.
Conclusions:
Bridged repair was associated with more SSOs than was PFC, and PFC should be used whenever feasible. Endoscopic and perforator-sparing CS were associated with the fewest complications; however, these conclusions are limited by heterogeneity between studies and poor methodological quality. These results should be used to guide future trials, which should compare the risks and benefits of each CS method to determine in which setting each technique will give the best results.
V
There are several types of CS—anterior, endoscopic, perforator-sparing, and posterior—and there is little consensus on which technique results in the fewest surgical complications. Anterior CS involves dissection of large lipocutaneous flaps between the subcutaneous fat and the anterior rectus sheath to release the external oblique aponeurosis [3]. Endoscopic CS avoids the creation of large skin flaps by incising the external oblique aponeurosis through a small incision, using a balloon dissector to separate the internal and external oblique muscles, and incising the remainder of the external oblique aponeurosis [4]. Perforator-sparing CS also divides the external oblique aponeurosis, but it preserves the medial blood supply to the skin and fat of the abdominal wall, which largely resides within approximately a 3-cm radius around the umbilicus [5]. Finally, posterior CS enters the retro-rectus space and releases the transverse abdominis, avoiding skin flaps and damage to the medial blood supply [6,7].
In this study, the primary aim was to determine whether bridged repair or primary fascial closure with mesh is associated with fewer surgical site occurrences (SSO) by performing a review of a multi-center database of VHRs as well as by conducting a systematic review of the literature and a meta-analysis. The secondary aims were to determine the type of CS associated with the fewest SSOs. We hypothesized that: (1) Repair of large ventral hernias with bridged repair is associated with more SSOs than repair with primary fascial closure; and (2) anterior CS is associated with more SSOs than endoscopic, perforator-sparing, or posterior CS.
Patients and Methods
Part I
Following Institutional Review Board approval, a retrospective, multi-center database of all patients who underwent VHR from 2010–2011 was assessed. The inclusion criteria included (1) open VHR; (2) mesh reinforcement; (3) defect size ≥8 cm width or loss of domain; and (4) a bridged repair, CS, or both, and (5) follow-up of at least 1 month. Bridged repair was compared with primary fascial closure with mesh, and all types of CS were compared with one another (anterior, endoscopic, perforator sparing, and posterior).
The primary outcome was SSO, which included surgical site infection (SSI), site dehiscence, seroma, hematoma, and incisional necrosis [8]. An SSI was defined by the U.S. Centers for Disease Control and Prevention (CDC) definition [9]. Major SSI was defined as deep and organ space SSI, including mesh infections. Incisional dehiscence was defined as any disruption of apposed surfaces of an incision [10]. Seroma and hematoma were diagnosed by either physical examination or radiologic imaging. The secondary outcome was hernia recurrence, determined either clinically or radiographically.
Patient demographics and co-morbidities, hernia characteristics, operative details, and outcomes were compared. The patient demographic data recorded were age, gender, and race. All variables were defined using the American College of Surgeons National Surgical Quality Improvement Project (ACS NSQIP) definitions or the European Hernia Society definitions; all other variables have been defined and reported [11–14].
Statistical analysis
Categorical data were analyzed using the χ2 test. Parametric continuous data were analyzed using a two-tailed t-test or analysis of variance (ANOVA). Non-parametric continuous data were analyzed using the Kruskal-Wallis rank test. Scheffe's method was used for post-hoc comparisons of multiple groups of continuous data where p < 0.05 on ANOVA.
Part II
Search strategy
Following registration of the study on PROSPERO (registration number CRD24015020308), a review of the MEDLINE, Embase, and Cochrane databases was performed. ClinicalTrials.gov and bibliographies of articles that met the inclusion criteria were reviewed. The search included all publications through April 2015. The Medical Subject Heading terms used were hernia OR abdominal wall reconstruction AND “component separation” OR “components separations” OR bridge OR bridged). The searches were subject to the following limits: (1) English-language articles; (2) human studies; and (3) adult subjects. Only comparative studies were included. Systematic reviews, meta-analyses, letters, pediatric studies, laparoscopic repairs, technique manuscripts, and non-VHR papers were excluded. The references of all selected articles were reviewed for additional citations not captured by the search strategy. Ventral Hernia Outcome Collaborative members were queried for additional references.
Studies were assessed and evaluated by two independent abstractors. Any disagreement was arbitrated through discussion with a third reviewer. Study quality was evaluated using the Methodological Index for Non-Randomized Studies (MINORS) [15]. Only studies with MINORS scores >10 were included, which is a cutoff that has been used in other systematic reviews [16]. Studies were classified into the following categories: (1) Comparing bridged repair with primary fascial closure with mesh (both groups with or without CS); and (2) comparing two or more types of CS. The primary outcome was SSO, and the secondary outcome was hernia recurrence. Articles were reviewed, and two independent abstractors collected primary and secondary outcome data. Study design, number of patients, body mass index (BMI), hernia area, type of repair, mesh type, mesh location, type of CS, and follow-up duration also were recorded. Heterogeneity was assessed methodologically by comparing patient BMI, hernia area, mesh type, mesh location, percentage of patients with CS, and follow-up duration between studies. A funnel plot was created to assess for publication bias.
Statistical analysis
A pooled analysis was performed to compare bridged repair with primary fascial closure and to compare the four types of CS. Pooled data came from the articles identified through the systematic review, as well as the data from part I of this study. Pairwise meta-analysis was performed to compare all direct treatment using fixed-effects and random-effects models. Heterogeneity was assessed using the heterogeneity p value. A multiple-treatment meta-analysis was performed to compare the different CSs. Anterior CS was the reference treatment to compare other CSs by estimating fixed effects and random effects models in the Bayesian framework.
Results
Part I
Of 393 open VHRs with a defect width ≥8 cm, 24 bridged repairs and 84 repairs with primary fascial closure met the inclusion criteria (Fig. 1). There were differences between the groups in ethnicity, gender, BMI, and whether the case was an emergency (Table 1).

Flow chart of patients. CS = component separation.
ASA = American Society of Anesthesiologists; COPD = chronic obstructive pulmonary disease; CS = component separation; DM = diabetes mellitus; SD = standard deviation; SSI = surgical site infection.
On unadjusted analysis, there was no statistically significant difference in SSO between bridged and primary fascial closures (45.8% vs. 26.2%; p = 0.065); however, the difference was substantial clinically (Table 2). There was no difference in the rate of SSIs or recurrences. The study was underpowered to detect a statistically significant difference between various kinds of CS for all outcomes (Table 2).
Bridged includes with and without CS.
CS includes anterior, endoscopic, perforator-sparing, and posterior.
CS = component separation; SSI = surgical site infection; SSO = SSI, dehiscence, seroma, hematoma, necrosis.
Part II
The initial search identified 765 references, but only 13 articles (including the current study) met the criteria for inclusion (Fig. 2). Four articles compared bridged repair with primary fascial closure with mesh, with or without CS. Ten compared different types of CS (Fig. 2). All of these had a MINORS score >10. There were some differences in patient and operative characteristics between the studies (Table 3) [17–22]. A funnel plot showed an even distribution of positive and negative studies (Fig. 3).
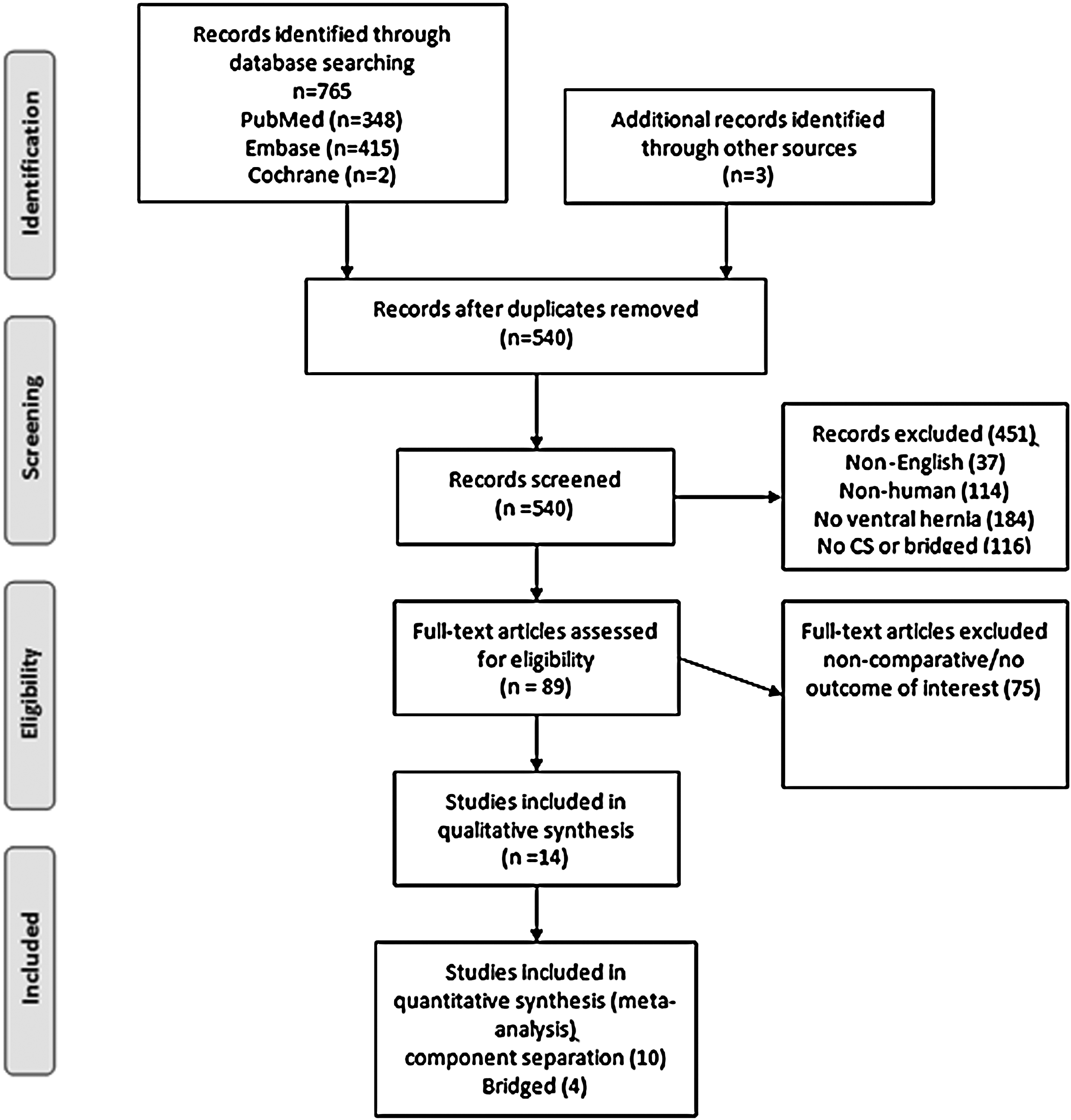
Systematic review search results.
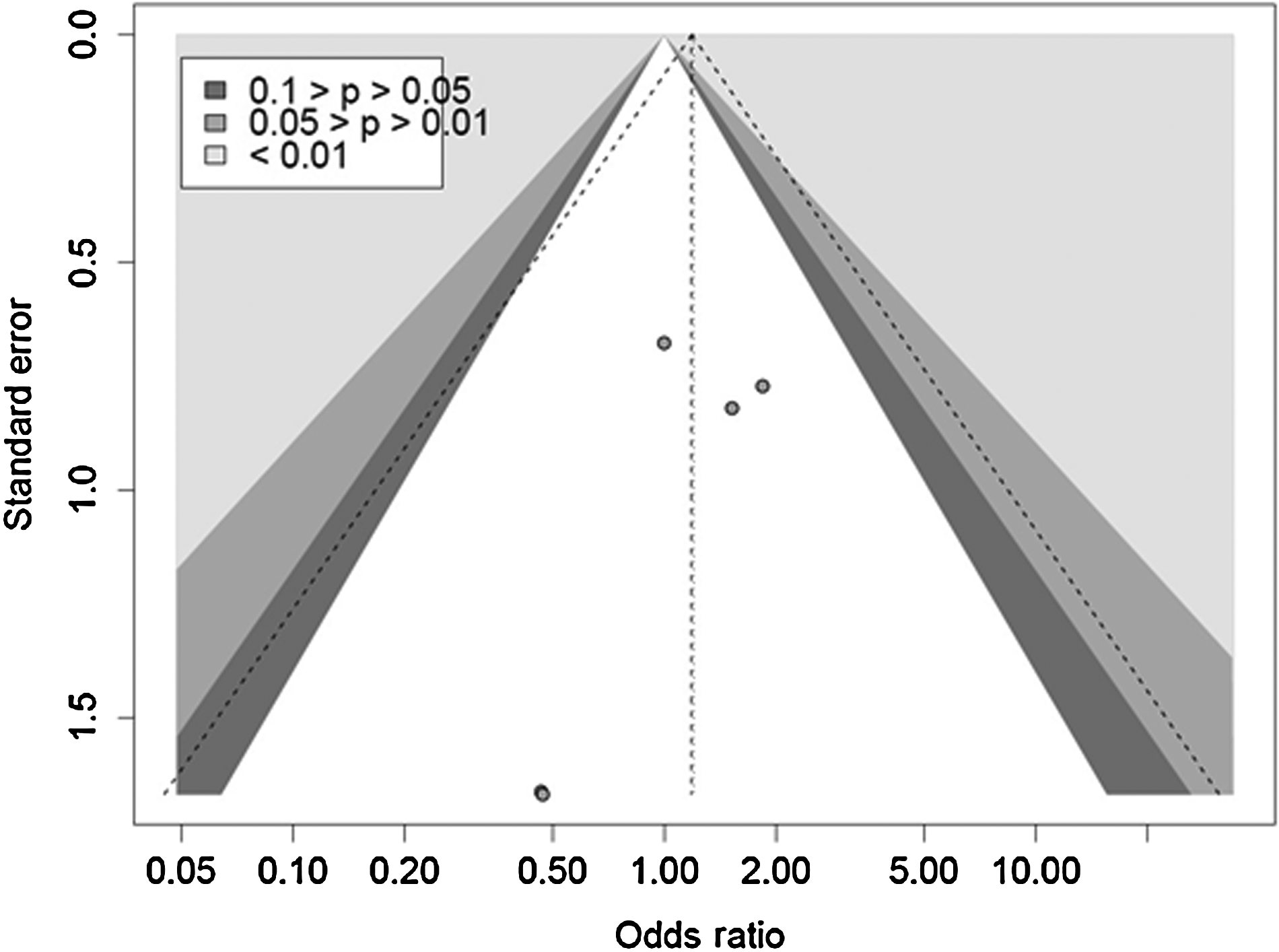
Funnel plot demonstrating even distribution of positive and negative studies.
Three studies reported the SSO rates for VHR with bridged repair or primary fascial closure (Table 3). The pooled rate of SSO was 37.4% (range 30.0%–45.8%; n = 91) for bridged repair and 24.1% (range 12.5–26.2%; n = 319) for primary fascial closure. Four studies reported on recurrence after VHR with bridged or primary fascial closure. The pooled recurrence rate was 49.0% (range 25.0%–72.7%; n = 102) for bridged repair and 11.1% (range 7.7%–18.2%; n = 341) for primary fascial closure.
Eight studies reported on the SSO rate for VHR with different CS methods (Table 3). The pooled SSO rate was 38.9% (range 28.6%–64.7%, n = 265) for anterior, 26.6% (range 25.5%–29.2%, n = 79) for posterior, 20.6% (range 5.6%–40.0%, n = 102) for endoscopic, and 9.2% (range 3.1%–25.0%, n = 130) for perforator-sparing CS. Nine studies reported on the recurrence rate after VHR with CS (Table 3). The pooled recurrence rate was 14.3% (range 0–27.3%, n = 287) for anterior, 8.9% (range 3.6%–20.85%, n = 79) for posterior, 11.3% (range 0–27.3%, n = 124) for endoscopic, and 10.0% (range 3.5%–25.0%, n = 130) for perforator-sparing CS.
On pairwise meta-analysis, primary fascial closure was associated with lower odds of SSO and recurrence than bridged repair (Table 4) [23–28]. The heterogeneity p value was 0.229 for SSO, indicating no statistically significant heterogeneity; however, the heterogeneity p value for recurrence was 0.012, suggesting heterogeneity of the studies.
Recur = recurrence; SSO = surgical site occurrence; any incisional complication.
Among the different CS methods, there was no difference identified for SSO or hernia recurrence (Table 4). The heterogeneity p values were all >0.05, indicating no statistically significant heterogeneity.
Utilizing multiple-treatments meta-analysis and a Bayesian framework, endoscopic and perforator-sparing CS had the highest probabilities of having the lowest rates of SSO and hernia recurrence, whereas anterior and posterior CS techniques had the lowest likelihood of being the best treatment (Table 5).
p < 0.1 indicates significant heterogeneity.
CI = confidence interval; OR = odds ratio; SSO = surgical site occurrence.
Discussion
In this study, combining data from a multi-center database with the literature demonstrated primary fascial closure with mesh to be associated with lower odds of SSO and recurrence than bridged repair. Of the CS methods, the endoscopic and perforator-sparing techniques had the highest probability of yielding the best results (lowest rates of SSO and hernia recurrence). However, there was substantial clinical heterogeneity between studies, and the interpretation of pooled and meta-analysis results should be approached cautiously. Furthermore, there was a lack of high-quality randomized controlled trials, and included studies had significant selection bias. Although these results cannot provide a definitive answer, they may be used to guide future trials.
Bridged repair has a number of theoretical flaws. For example, mesh is exposed to both skin/subcutaneous tissue and intra-abdominal contents, leaving it susceptible to infectious complications. With primary fascial closure, a layer of fascia and muscle often covers the mesh, depending on the site of its placement. In addition, because of LaPlace's law (wall tension is proportional to the radius and inversely proportional to wall thickness), recurrence rates may be higher with a bridge repair. The mesh may act like a “sail in the wind” [29]. For these reasons, bridged repair has fallen out of favor with many ventral hernia surgeons, and the growing trend is to re-approximate the fascia to recreate a functional abdomen [2]. The likelihood of achieving higher-quality evidence and completing a randomize trial of open repairs comparing bridged and primary fascial closure is low because of the lack of clinical equipoise. However, there are several ongoing clinical trials comparing laparoscopic bridged repair with repair with primary fascial closure [30–32]. Data from these trials, when available, may provide further guidance on the issue of bridged vs. primary fascial closure. However, generalizing these results to open repairs must be done with caution. Until these trial data are available, the data presented here may represent the best evidence available to answer this question. When it is safe and feasible, primary fascial closure appears to yield superior outcomes compared with bridged repairs in open VHR. In the acute setting, depending on the degree of contamination, patient stability, and volume status, less may be better. Skin closure alone or bridged repair to temporize the situation may be the safest choices.
The use of CS occasionally is needed to achieve primary fascial closure. When comparing different types of CS, anterior separation yielded the highest rates of SSO and recurrence. This may be attributable to the large lipocutaneous flaps created during anterior CS, as skin flaps are predictive of SSI and SSO [11]. In addition, site infections predict hernia recurrence [33]. However, it is unclear if there are settings in which anterior CS may still play a role. Many surgeons believe that full anterior CS yields the greatest amount of release and medialization of the rectus complex. In young, non-smoking patients with a normal vascular supply, anterior CS may retain a role for repair of large defects where additional advancement on each side may make a difference in achieving primary fascial closure.
The operations with the lowest reported rates of complications were endoscopic and perforator-sparing CS. Endoscopic CS was the best treatment to avoid SSO, whereas perforator-sparing was the best treatment to avoid recurrence. However, these techniques are not without their limitations. Many surgeons have abandoned endoscopic CS because of the reportedly limited release, high lateral seroma rate, and technical challenges [25]. For perforator-sparing CS, often, the central perforators are part of the redundant skin that will need to be resected. The release may be limited in inexperienced hands, and large flaps are created that risk seroma formation [24]. Often, this technique is paired with other techniques to reduce the risk of seromas but carry their own set of risks such as SSI [34,35]. In addition, these results are limited by selection bias, as the patients who received endoscopic or perforator-sparing CS were different from those receiving anterior CS.
There are few comparative data on posterior CS, limiting the accuracy of conclusions from this study. Compared with all other techniques, posterior CS has the advantage of avoiding undermining of the skin. The ability to achieve wide mesh overlap may result in low recurrence rates. Posterior CS is associated with other challenges, including technical difficulty in performing the procedure, the risk of damaging the posterior sheath and allowing bowel to contact mesh, and the risk of denervating the rectus complex. Despite this, many surgeons have identified a significant role for posterior CS in their practices. As only two studies in the systematic review included posterior CS, further studies in this area are warranted [26].
There are limited data comparing the types of CS, suggesting a need for further research. Although randomized controlled trials are considered the gold standard of clinical research, there are several obstacles to overcome prior to embarking on a trial comparing methods of CS. First, surgeon expertise may limit the ability to conduct an unbiased trial. Many surgeons are most comfortable with one particular method of CS, and it may not be feasible to randomize patients to a different type. A potential solution would be to consider an expertise-based randomized trial, where patients are randomized to undergo intervention A or B performed by a clinician with expertise in intervention A or intervention B. In this situation, clinicians perform only procedures in which they are experts [36]. This type of trial may avoid cross-over and bias that may be introduced by unblinded surgeons in conventional randomized controlled trials. It also may be more ethical to enroll patients in a study where an expert will be performing their procedure no matter which intervention they are randomized to undergo. This study design may increase the feasibility of surgical studies.
Deviance Information Criterion (DIC) 58.3.
DIC 45.5.
SSO = surgical site occurrence.
Another challenge to studying CS is accruing an adequate sample size. In order to determine the method of CS with the lowest rate of SSOs, we would need a total sample of 152 patients to detect the difference observed in this study for the two best methods, endoscopic and perforator-sparing CS (alpha = 0.05, beta = 0.20; treatment difference 20.6% vs. 9.2%). In our multi-institutional database, including seven centers with treatments given over two years, only 84 patients met the criteria for inclusion, suggesting that a sample size of 152 may not be feasible. Furthermore, most of the studies included in this review were small and underpowered because of the low number of patients undergoing CS. This might be overcome by looking at alternative outcomes, such as patient-centered outcomes, to limit the sample size needed. Patient-centered outcomes address concerns that are most relevant to patients. There has been increasing emphasis on measuring patient-centered outcomes in comparative effectiveness research, yet there are few studies addressing patient-centered outcomes in a procedure as common as VHR. In addition, multiple centers could participate in the study to increase enrollment.
This study has several limitations. First, the methodologic and statistical heterogeneity in parts of this study may limit significantly the ability to combine studies and draw conclusions. As such, these results are intended to guide future trials rather than to provide definitive answers. Furthermore, all of the studies included were retrospective and subject to selection bias. The conclusions reached are limited by the quality of the data included. Next, there is a risk of publication bias, as negative studies tend to be published less frequently, and only English-language studies were included. However, a funnel plot demonstrated an even distribution between positive and negative studies (Fig. 3).
Conclusions
In this meta-analysis of open VHR, primary fascial closure was associated with fewer SSOs and recurrences than was bridged repair. Although the data are poor, in the absence of a randomized trial, this may be the best available evidence. As such, primary fascial closure should be achieved when safe and feasible. Furthermore, endoscopic and perforator-sparing CSs were associated with the lowest rates of SSO and recurrence, whereas anterior CS uniformly had the worst results; however, these findings are limited by heterogeneity between studies and low methodologic quality. These results may best be used as a guide for future studies by suggesting which interventions should be studied and which outcomes should be compared. Future studies should compare the amount of release obtained by each type of CS and the risks and benefits of each approach in similar patients, hernias, and clinical settings.
Footnotes
Author Disclosure Statement
This work was supported by the Center for Clinical and Translational Sciences, which is funded by National Institutes of Health Clinical and Translational Award UL1 TR000371 and KL2 TR000370 from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.