
Abstract
Abstract
Background:
We investigated the value of the neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) as markers of mortality in patients with Fournier's gangrene.
Methods:
Records from 62 patients treated for Fournier's gangrene between 2003 and 2014 were reviewed retrospectively. Data were collected regarding medical history, symptoms, physical examination findings, admission laboratory tests, and the extent of body surface area involved (%). Fournier's Gangrene Severity Index score, NLR, and PLR were calculated. The data were assessed separately for surviving and deceased patients.
Results:
Of the 62 patients, 36 survived (58%, group 1) and 26 died (42%, group 2). Parameters that were statistically different between the two groups (p < 0.05) were the NLR, PLR, Fournier's Gangrene Severity Index score, and admission laboratory parameters, including body temperature, heart rate, bicarbonate, albumin, and serum calcium. The average body surface area affected in group 2 was statistically different from that of group 1 (6.0% versus 2.3%, p = 0.001). A high Fournier's Gangrene Severity Index score (>9), high NLR (>8), and high PLR (>140) were associated more frequently with group 2 patients. Multivariable regression analysis showed that high NLR (adjusted odds ratio [OR], 4.66; 95% confidence interval [CI], 1.25–17.3; p = 0.022) and high PLR (adjusted OR, 11.6; 95% CI, 2.7–49.5; p = 0.001) were independent prognostic factors for poor prognosis from Fournier's gangrene. However, the Fournier's Gangrene Severity Index score did not shown any statistically significant effect on mortality (p = 0.086).
Conclusions:
The Fournier's Gangrene Severity Index scoring system was not associated with determining poor prognosis, however, high NLR and high PLR were associated with predictors of mortality in patients with Fournier's gangrene.
F
Several studies have identified possible risk factors for predicting the prognosis of patients with Fournier's gangrene. Proposed prognostic factors include the Fournier's Gangrene Severity Index score, suppressed immunity, and the extent of the body surface involved. Since its development, the Fournier's Gangrene Severity Index score has been used widely for predicting the prognosis of Fournier's gangrene, especially mortality and disease progression. The Fournier's Gangrene Severity Index score has been validated by several studies [4–21]. In fact, because of the lack of tools to determine prognosis from time of admission, the only well-known tool is the Fournier's Gangrene Severity Index score, however, its accuracy remains questionable. Recent studies have attracted attention, using new parameters such as neutrophil to lymphocyte ratios (NLR) and platelet to lymphocyte ratios (PLR) to predict the prognosis specifically of inflammatory disease and ischemic events [22–26]. In this study, we investigate the value of NLR and PLR as indicators of mortality in patients with Fournier's gangrene.
Patients and Methods
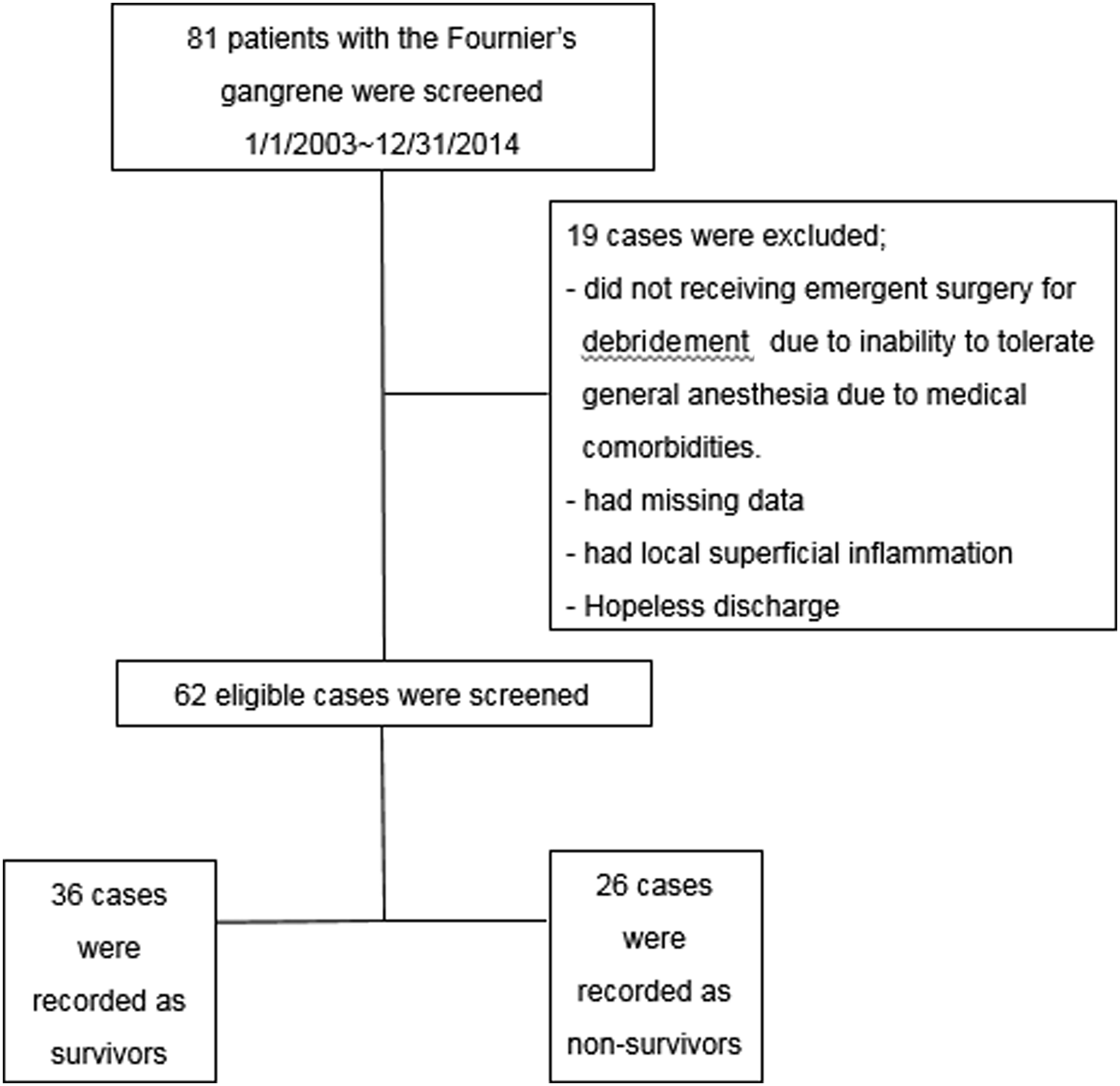
After obtaining approval from our Institutional Review Board, the medical records of 62 consecutive patients admitted to our center with a diagnosis of Fournier's gangrene during the 11-y period between 2003 and 2014 were reviewed retrospectively. The inclusion criteria were as follows: scrotal erythema, swelling, wound discharge, fluctuation, crepitus, and progressive soft tissue necrotizing process that led to gangrene (determined using computed tomography scanning). Nineteen patients who had not received emergent surgery because of medical comorbidities, had missing data, had local superficial inflammation of the perianal or urogenital regions, and patients who did not want any treatment were excluded from the study (Fig. 1). Mortality was defined as disease-related death during the hospital stay and survival was measured in days.
Enrollment and stratification.
Data were collected regarding each patient's age, gender, medical history, or underlying disease; interval between the onset of symptoms; physical examination findings; vital signs; admission laboratory tests; and the percent of body surface area involved. Laboratory findings such as complete blood count, electrolytes, biochemical profiles (such as bicarbonate and albumin), and predisposing factors were recorded during the emergency department evaluation. Most patients underwent an emergency operation for surgical debridement of infected lesions, except for those who could not tolerate general anesthesia because of poor general health. Administration of empiric broad-spectrum penicillin or third-generation cephalosporin and an aminoglycoside (e.g., gentamicin), plus metronidazole or clindamycin, mostly ceftriaxone 2 g/d, metronidazole 1.5 g/d were chosen while awaiting the results of microbiologic cultures on admission to the hospital. Bacterial cultures were obtained during the operation, and the antibiotic regimen was adjusted according to the results of pus culture.
Fournier's Gangrene Severity Index score
Fournier's Gangrene Severity Index score was determined at the time of admission. To calculate this score, nine parameters (temperature, heart rate, respiratory rate, serum sodium, potassium, creatinine, bicarbonate, hematocrit, and white blood cell [WBC] count) were used; the deviation from normal was graded from 0–4. The scores were divided into high (>9) and low (≤9) scores [21].
Extent of body surface involvement
The percentage of the body area affected by Fournier's gangrene was calculated based on a nomogram used routinely to assess the extent of burn injuries. The penis, scrotum, and perineum represented 1% of the surface area, and ischiorectal fossae represented 2.5% each [27].
Assessment of NLR and PLR
The NLR and PLR were used as markers of subclinical inflammation. Using peripheral blood samples, the ratios were calculated by dividing the number of neutrophils by the number of lymphocytes to obtain the NLR, or by dividing the number of platelets by the number of lymphocytes to generate the PLR. The NLR and PLR were calculated based on laboratory findings from emergency department evaluations at the time of admission. We selected the median values of NLR and PLR as cutoff values. The values were validated by receiver operating characteristic curve.
Statistical analysis
Statistical analyses were performed using the IBM SPSS software package version 21.0 (Statistical Package for Social Sciences, IBM, Armonk, NY) and MedCalc software version 15 (MedCalc Software bvba, Ostend, Belgium). Mortality was defined as disease-related death during the hospitalization period. Differences in clinical parameters and predisposing factors between group 1 and 2 patients were compared using the Student t-test and the χ2 test. Multivariable logistic regression analyses were used to identify a prognostic factor. Cutoff values were validated using a receiver operating characteristic (ROC) curve. The statistical significance was set at p < 0.05 for all analyses.
Results
As determined from bacterial cultures, the most common pathogens were Klebsiella spp. (21%), Staphylococcus spp. (16.1%), Escherichia coli (8.1%), Streptococcus spp. (8.1%), and Pseudomonas spp. (6.5%) (Table 1). Of the 62 patients, 36 (58%) survived and were categorized as group 1; 26 (42%) died and were categorized as group 2. Etiologic factors for mortality in the total non-survivors (n = 26) were septic shock (n = 23), disseminated intravascular coagulation (n = 1), chronic kidney disease aggravation (n = 1), and hepatic failure caused by liver cirrhosis (n = 1). Sixty-one patients (98.3%) were male and one was female (1.7%). The most common predisposing factors in both groups were diabetes mellitus (33.8%), alcohol abuse (19.3%), previous operation history (16.1%), paraplegia (12.9%), and chronic renal failure (1.6%). The predisposing factors were not different between the two groups (p = 0.085, Table 2). The patients' ages (57.1 ± 14.4 versus 56.2 ± 13.0 years, p = 0.808) and time of onset (7.1 ± 7.2 versus 4.9 ± 6.7 days, p = 0.230) did not differ between the groups (Table 2). However, several admission laboratory parameters, including body temperature (36.7°C ± 0.7°C versus 37.2°C ± 0.9°C, p = 0.009), heart rate (81.8 ± 11.0 versus 97.9 ± 15.4 beats per minute, p = 0.001), bicarbonate (22.7 ± 4.6 versus 17.7 ± 5.8 mEq/L, p = 0.001), albumin (2.8 ± 0.7 versus 2.4 ± 0.5 g/dL, p = 0.024), and serum calcium (4.3 ± 0.5 versus 3.1 ± 0.7 mEq/L, p = 0.001) were statistically different between the two groups. Operation interval (in days) for survivors was 0.3 ± 0.6 and for non-survivors 0.2 ± 0.4 (p = 0.152).
Student t-test.
Chi-square test.
SD = standard deviation; WBC = white blood cell count; ALP = alkaline phosphatase; LDH = lactate dehydrogenase; CRP = C-reactive protein; NLR = neutrophil to lymphocyte ratio; PLR = platelet to lymphocyte ratio.
The average affected body surface area in group 2 was greater than that of group 1 (6.0 ± 1.9 versus 2.3 ± 1.5%, p = 0.001). The NLR (7.2 ± 3.2 versus 16.5 ± 10.1, p = 0.001), PLR (124.5 ± 43.6 versus 221.4 ± 136.5, p = 0.002), and Fournier's Gangrene Severity Index score (4.1 ± 3.7 versus 7.9 ± 4.1, p = 0.001) were also different between the two groups. A high Fournier's Gangrene Severity Index score (>9), a high NLR (>8), and a high PLR (>140) were more often associated with group 2. Receiver operator characteristic analysis showed that areas under the receiver operating characteristic curve (AUROC) of NLR and PLR were 0.860 and 0.787, respectively (p = 0.001, p = 0.001, respectively; Fig. 2). Multivariable regression analysis showed that a high NLR (adjusted odds ratio [OR], 4.66; 95% confidence interval [CI], 1.25–17.3, p = 0.022) and a high PLR (adjusted OR, 11.6; 95% CI, 2.7–49.5; p = 0.001) were independent prognostic factors of mortality from Fournier's gangrene, whereas the Fournier's Gangrene Severity Index score had no significant prognostic value (adjusted OR, 5.41; 95% CI, 0.78–37.1; p = 0.086; Table 3).
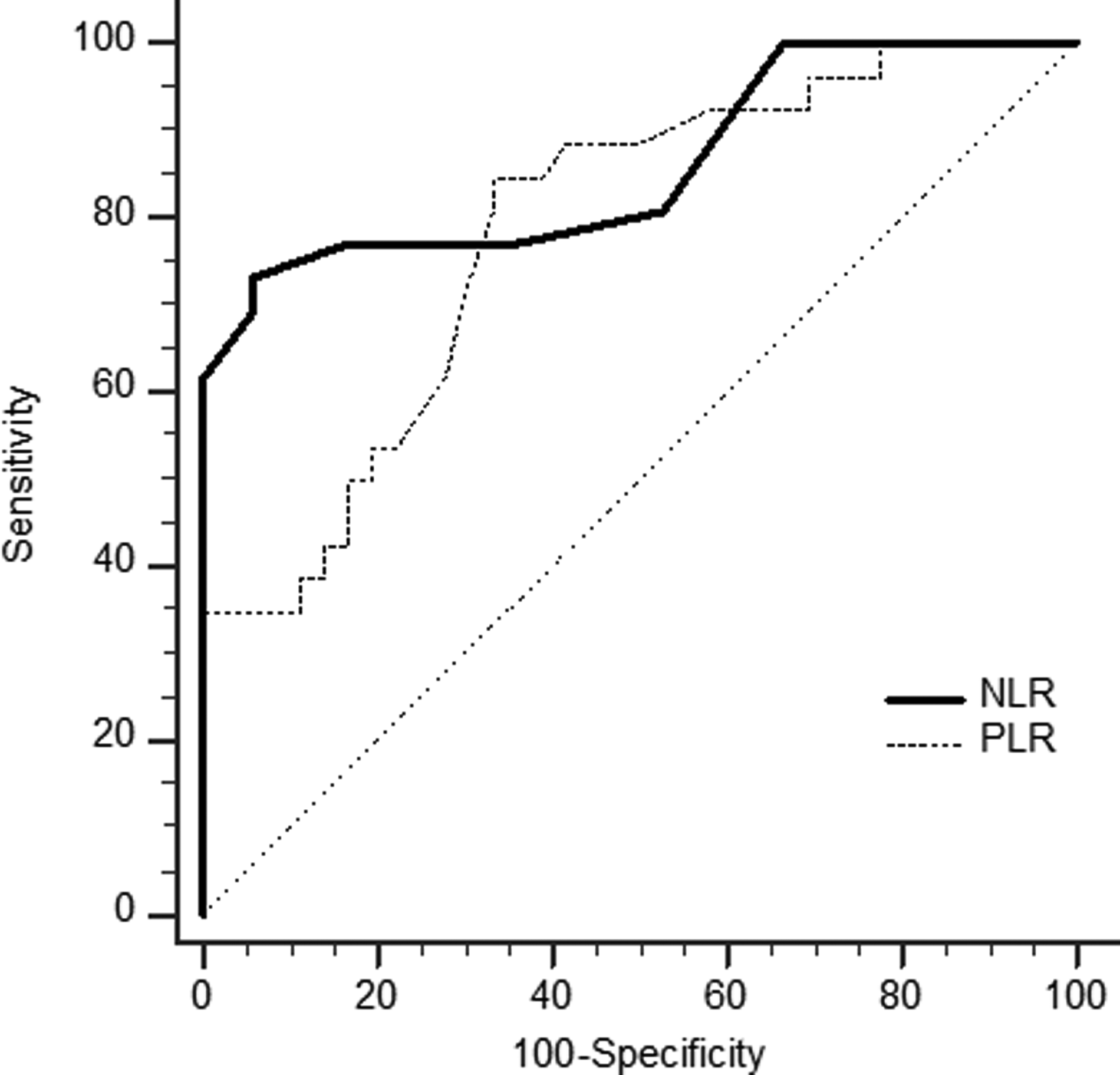
Receiver operator characteristic curve for neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR). (For NLR; area under the curve = 0.860, p = 0.001, sensitivity = 76.9%, specificity = 63.8%, positive predictive value = 60.6%, negative predictive value = 79.3%, For PLR; area under the curve = 0.787, p = 0.001, sensitivity = 84.6%, specificity = 66.6%, positive predictive value = 64.7%, negative predictive value = 85.7%.)
CI = confidence interval; PLR = platelet to lymphocyte ratio; NLR = neutrophil to lymphocyte ratio.
Discussion
In this study, we determined that the NLR and PLR are independent prognostic factors associated with mortality in Fournier's gangrene. Fournier's gangrene is an acute, rapidly progressive, and potentially fatal infective necrotizing fasciitis that affects the external genitalia, perineal, or perianal regions, and is caused by the synergistic effects of aerobic and anaerobic organisms. Fournier's gangrene primarily affects men but can also occur in women and children. There have been many efforts to treat Fournier's gangrene, however, despite advances in antimicrobial drugs, surgical techniques, and intensive care facilities, Fournier's gangrene still has a high mortality rate of 20%–50% [11,12]. Organisms such as E. coli, Klebsiella spp., Pseudomonas spp., Streptococcus spp., and Staphylococcus spp. are the primary pathogens that infect patients with Fournier's gangrene [28], with multiple studies reporting E. coli as the predominant bacterial agent. However, in this study and that of Laor et al. [19], Klebsiella spp. and Staphylococcus spp. were the most prevalent organisms infecting patients with Fournier's gangrene.
The high mortality of Fournier's gangrene reflects the aggressive nature of the infection and the destructive effects of the accompanying predisposing factors, such as advanced age, diabetes mellitus, chronic renal failure, delay in treatment, evidence of systemic sepsis at presentation, extent and depth of involvement, Fournier's Gangrene Severity Index score, and many others [8–13]. The roles of these and other parameters that influence the prognosis of patients with Fournier's gangrene remains controversial. Similar to other reports, this study found that 42% of patients died from disease-related complications. For this reason, early acquisition of patient information, including their general condition, underlying diseases, and laboratory findings at admission, is important for early intervention and prediction of the prognosis. In our study, previous well-known predisposing factors such as diabetes mellitus, alcohol abuse, paraplegia, previous surgery, and chronic renal failure were also involved. The most common predisposing factor was diabetes mellitus. Chemotaxis, phagocytosis, neutrophil function, disorders of humoral immunity, and cellular digestion caused by a reduced T-cell response are impaired in patients with diabetes mellitus, leading to an increase in susceptibility to infections [29,30]. In this study, 21 patients (33.8%) had diabetes mellitus, supporting an association between diabetes mellitus and Fournier's gangrene, whereas factors other than diabetes mellitus had no significant association with the occurrence of Fournier's gangrene.
Taviloglu et al. [14] suggested that female gender, the presence of underlying malignant disease, and diabetes mellitus were associated with increased mortality from Fournier's gangrene; however, many patients with Fournier's gangrene in this study had diabetes mellitus and it did not correlate with mortality. Clinical parameters at admission, including advanced age, extent of disease, opening of a diverting colostomy, low hematocrit, low albumin concentrations, elevated blood urea nitrogen, elevated serum creatinine, and elevated alkaline phosphatase concentrations have been reported as prognostic factors for Fournier's gangrene [15,16].
In our study, body temperature, heart rate, bicarbonate, albumin, total serum calcium, and the extent of the body surface affected were all indicators of poor prognosis. Serum albumin reflects the state of visceral protein and has been combined with anthropometric measures to indicate a patient's nutritional status. Therefore, a low albumin concentration is regarded as an indicator of a patient's poor general condition caused by malnutrition. Low bicarbonate is considered a state of metabolic acidosis caused by decreased renal function, and calcium imbalance is also caused by renal failure. In metabolic acidosis, production of interleukins by macrophages is stimulated and lymphocyte function is suppressed, leading to increased inflammation and impaired immune response. Therefore, the chemotactic properties and bactericidal capacity of leukocytes are reduced [17,18]. Laor et al. [19] developed the Fournier's Gangrene Severity Index score and identified nine factors (temperature, heart rate, respiratory rate, serum sodium, potassium, creatinine, bicarbonate concentrations, hematocrit, and WBC count) associated with poor prognosis for patients with Fournier's gangrene. The nine parameters are graded from 0 to 4 based on severity, with a higher score in the non-surviving group than in the surviving group. When a Fournier's Gangrene Severity Index score of 9 is set as a threshold, 75% of patients with a score >9 are predicted to die and 78% of patients with a score <9 are predicted to survive.
Tuncel et al. [20] showed that the Fournier's Gangrene Severity Index score was not related to prognosis and that the extent of body surface affected and specific parameters such as serum albumin and alkaline phosphatase are more important for predicting mortality. In our study, a high Fournier's Gangrene Severity Index score (>9) was generally associated with the non-surviving group, however, multivariable regression analyses found this not to be statistically significant (p = 0.086). In general, time to operation is considered one of the important parameters in determining prognosis in cases of infectious disease requiring surgical treatment. However, this study did not show statistical significance (p = 0.152). There was no significant difference between the time of onset between survivor and non-survivor, but survival time was shortened, which may be associated with fatal infection.
Recently, several investigators have reported the utility of NLR and PLR as new predictors for inflammatory disease and ischemic events, including Fournier's gangrene. Kahramanca et al. [22] showed that higher NLR and PLR were more effective than the Fournier's Gangrene Severity Index score at predicting the prognosis and mortality rate for Fournier's gangrene. The NLR and PLR were higher in patients who required more than one debridement than in single-debridement patients; however, there was no significant difference in the Fournier's Gangrene Severity Index score between the two groups. Ishizuka et al. [23] reported that a higher pre-operative NLR concentration (>8) can predict severe acute appendicitis. Azab et al. [24] investigated the value of the PLR after non-ST elevated myocardial infarction and showed that a higher PLR (≥176) correlated with a higher mortally rate. Celikbilek et al. [25] showed that increased NLR is a marker of poor prognosis and death in ischemic cerebrovascular disease. In addition, Taşoğlu et al. [26] found that use of the NLR and PLR can predict a limb's survival length in patients with critical limb ischemia. Patients with an elevated NLR (≥3.2) and PLR (≥160) had shorter limb survival (22 mo) than patients with a lower NLR and PLR (60 mo). Myocardial infarction, appendicitis, ischemic cerebrovascular disease, critical limb ischemia, and Fournier's gangrene cause tissue necrosis; the fact that the pathologic causes are considered similar for these diseases supports the use of the NLR and PLR as predictors of disease outcome. Because our study used multivariable regression analysis to demonstrate a relation between a high NLR and PLR and mortality in Fournier's gangrene patients, we consider these parameters good prognostic factors in Fournier's gangrene patients. Salciccioli et al. [31] reported that NLR was prognostic in intensive care unit patients, but not in subgroup analysis of patients with sepsis. However, our results suggested that NLR associated with poor prognosis of Founier's gangrene. This may have influenced clinical characteristics of patients and features of Founier's gangrene in our study. In addition, Kumar et al. [32] reported that early empiric combination antibiotic therapy with two antibiotics of different mechanisms of action is associated with superior outcomes than monotherapy in the treatment of severe infectious disease patients. The use of antibiotics also influenced prognosis of Founier's gangrene.
This study has several limitations. First, because of the retrospective nature of the study and the small number of patients, the hematologic and biochemical parameters were not representative of all patients with Fournier's gangrene. Second, the cutoff values of the NLR and PLR have not been established; therefore, we used a median value for each parameter. However, the value of each parameter has moderate sensitivity, specificity, positive predictive value, and negative predictive value. Third, a single tertiary referral hospital participated in the study. Fourth, surgeries were not performed by the same surgeon nor was the same technique used for all study patients. Fifth, the value of Fournier's Gangrene Severity Index score would have been impacted by the small number of patients. Despite these limitations, this study remains important for estimating the utility of the NLR and PLR in Fournier's gangrene.
In conclusion, a high NLR (>8) and a high PLR (>140) are valuable prognostic factors for mortality in patients with Fournier's gangrene. These scores can be determined by readily available and inexpensive tests, and could be ideal biomarkers for predicting outcome in patients with Fournier's gangrene. Therefore, patients with high NLR and high PLR should receive more active management. To clarify these findings, a prospective and multi-institutional study is needed.
Footnotes
Author Disclosure Statement
No financial support was received for this study. The authors have no conflicts of interest to report.