
Abstract
Abstract
Background:
Reducing surgical site infections (SSI) following median sternotomy remains a challenge for cardiac surgeons. Standard prophylaxis of SSI at our institution includes pre-operative skin disinfection with isopropyl alcohol (IPA). The addition of chlorhexidine gluconate (CHG) has the theoretical advantage of longer antimicrobial activity (>48h), compared with 2 h for IPA alone.
Objectives:
This prospective registry study was conducted to evaluate the effect of combined CHG-IPA (ChloraPrep®) skin antiseptic on the incidence of sternal surgical incision infections after cardiac surgical procedures via median sternotomy.
Methods:
Between September 2011 and November 2013, 3,942 consecutive patients underwent cardiac surgery with median sternotomy at our institution. Among them, 2,985 patients met inclusion criteria and were enrolled in the study. The complete cohort was prospectively divided into two registries. In registry 1 (1,523 patients), CHG-IPA was used to disinfect skin at the thoracic operative site prior to incision. In registry 2 (1,462 patients), single IPA disinfection was used. The primary endpoint was the incidence of post-sternotomy mediastinitis within 30 d of surgery. Secondary endpoints were SSI of any other kind, 30-d survival, and hospital length of stay.
Results:
Both registries were well matched in baseline characteristics and main risk factors. Post-operative data analysis revealed reduction in the rate of post-sternotomy mediastinitis in registry 1 (29 patients, 1.9%) versus registry 2 (62 patients, 4.2%), p = 0.0002. No relevant difference in incidence of other surgical site infections, length of hospital stay, and 30-d mortality was found.
Conclusions:
Skin disinfection with combined chlorhexidine-isopropyl alcohol reduced the incidence of mediastinitis in elective adult cardiac surgery with median sternotomy but did not affect other types of surgical site infections.
R
In the present study, we focused on pre-operative antiseptic skin preparation. Three groups of antiseptic agents are available for disinfection of the incision site: 1) Iodine/iodophors, 2) alcohol solutions, and 3) chlorhexidine. Standard prophylaxis of SSI at our institution includes pre-operative skin disinfection with isopropyl alcohol (IPA). The addition of chlorhexidine gluconate (CHG) has the advantage of longer antimicrobial activity (>48h), compared with 2 h for IPA alone [2]. Therefore, we investigated the influence of combined IPA-CHG disinfection on sternal surgical incision infection rates.
Patients and Methods
Study design
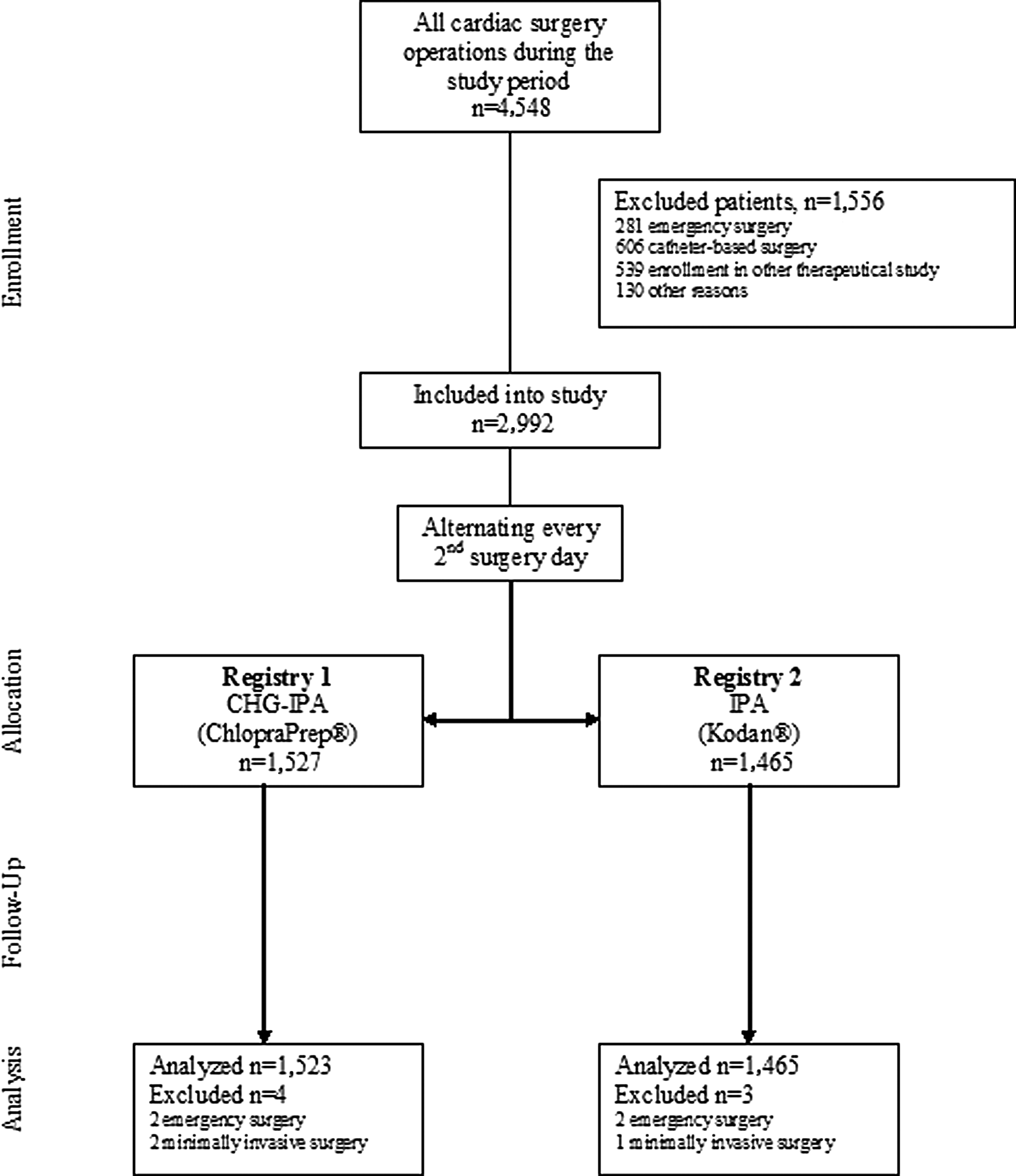
This prospective, controlled, registry study included patients undergoing cardiac surgery with median sternotomy in our institution between September 2011 and November 2013 (27 mo). A total of 4,548 patients underwent cardiac surgery during the study period. One thousand five hundred fifty-six patients were excluded because they failed to meet study criteria (Table 1). A total of 2,992 patients met the inclusion criteria and were enrolled into the study (Fig. 1). All study participants gave informed consent prior to surgery. The study was approved by the Ethics Committee of the Medical Faculty, Technical University Dresden, Germany (ref: EK 216072012).
Study design.
The study group was prospectively divided into two registries by alternating the application of skin disinfection every second surgery day, regardless of the institutional operation schedule. After 30-d follow-up, 1,523 patients were analyzed in registry 1 and 1,465 patients were analyzed in registry 2. Four patients were excluded from the analysis because the surgery status unexpectedly changed to emergency and three operations were performed minimally invasive, which was originally not planned.
Peri-operative tactics
Pre-operative preparation of the surgical site included standard preventive procedures such as shower and hair removal with the clipping machine on the day of operation. During introduction of general anesthesia, antibiotic prophylaxis with cefuroxim 1.5g IV was applied 30 min prior to the operation. Antiseptic solution was applied on the skin surface of the surgical site directly before the skin incision. In registry 1, combined IPA-CHG (ChloraPrep® 26 mL applicator with 70% IPA and 2% CHG; CareFusion, San Diego, California) was used. According to the manufacturer recommendation, the area of skin incision was “scrubbed” for 30 sec, followed by “painting” of the antiseptic on the whole surgical area. In registry 2, single IPA (Kodan® with 55% IPA; Shuelke, Norderstedt, Germany) antiseptic was applied three times on the whole surgical area.
After effective time of skin antiseptic, the surgical area was covered with sterile dressing. Median sternotomy was performed with a standard technique. After cardiac procedure and control of hemostasis, sternal closure was completed according to the institutional standard using eight wires. The surgical incision was then closed in layers in the usual manner, using suture or clips for skin closure. The surgical incision was covered with a sterile dressing.
Surgical incision management
After surgery, all patients were examined daily for signs of infection. If any sternal surgical incision abnormality was observed, a trained surgical incision nurse monitored and recorded the surgical incision status for 30 d or longer if necessary. Surgical site infection was reported when any of the following criteria was met: Localized swelling, erythema, secretion, or surgical incision dehiscence. Post-sternotomy mediastinitis (PSM) was defined according to U.S. Centers for Disease Control and Prevention (CDC) criteria, which includes sternal instability with positive bacterial culture from mediastinum [3].
Data collection and estimation of sample size
Pre-operative, intra-operative, and post-operative data for all patients were prospectively collected and retrospectively analyzed. The primary endpoint was the incidence of PSM up to the 30th post-operative day after the index surgery. Secondary endpoints were SSI of any other kind, 30-d survival, and hospital length of stay. Sample size calculations (alpha = 0.05; beta = 0.2, reduction of incidence to 2/3) determined that at least 1,470 patients per group would be required for statistically significant comparison of endpoints.
Statistical methods
Statistical analysis was performed with the JMP 7.0.1 software (SAS Institute Inc., Cary, North Carolina) using the χ2 test, Student t-test, and Fisher exact test. Continuous variables were presented as mean value ± standard deviation (SD), while binary data were presented as percentage of the study population. A p < 0.05 was considered statistically significant in reference to all study data.
Results
Patient characteristics
The analysis of demographic and pre-operative data showed that both registries were well matched in baseline characteristics and pre-operative risk factors (Table 2). Estimated risk of major surgical site infection was similar in both registries.
Continuous variables are presented as the mean value ± standard deviation (SD); binary data are presented as percentage of the study population.
BMI = body mass index; COPD = chronic obstructive respiratory disease.
Estimated probability of major infection according the calculation of Fowler et al. [7].
Peri-operative data
Peri-operative parameters are listed in Table 3. Neither the type of surgery, frequency of single, or bilateral mammary artery harvesting, nor surgery duration and post-operative blood loss differed substantially between registries.
Number of transfused units of erythrocyte concentrates per patient during hospital stay.
Outcome
A summary of post-operative findings is presented in Table 4. Incidence of PSM was 1.9% (29 patients) in registry 1 (IPA-CHG) and 4.2% (62 patients) in registry 2 (IPA). Observed PSM was substantially lower in registry 1 (p = 0.0002). There were no substantial differences in the incidence of other SSI, in-hospital length of stay, 30-d mortality, or overall SSI-associated death between the registries. Most SSI were caused by coagulase negative staphylococci, followed by Staphylococcus aureus (Fig. 2). Pathogens identified did not differ substantially between groups.
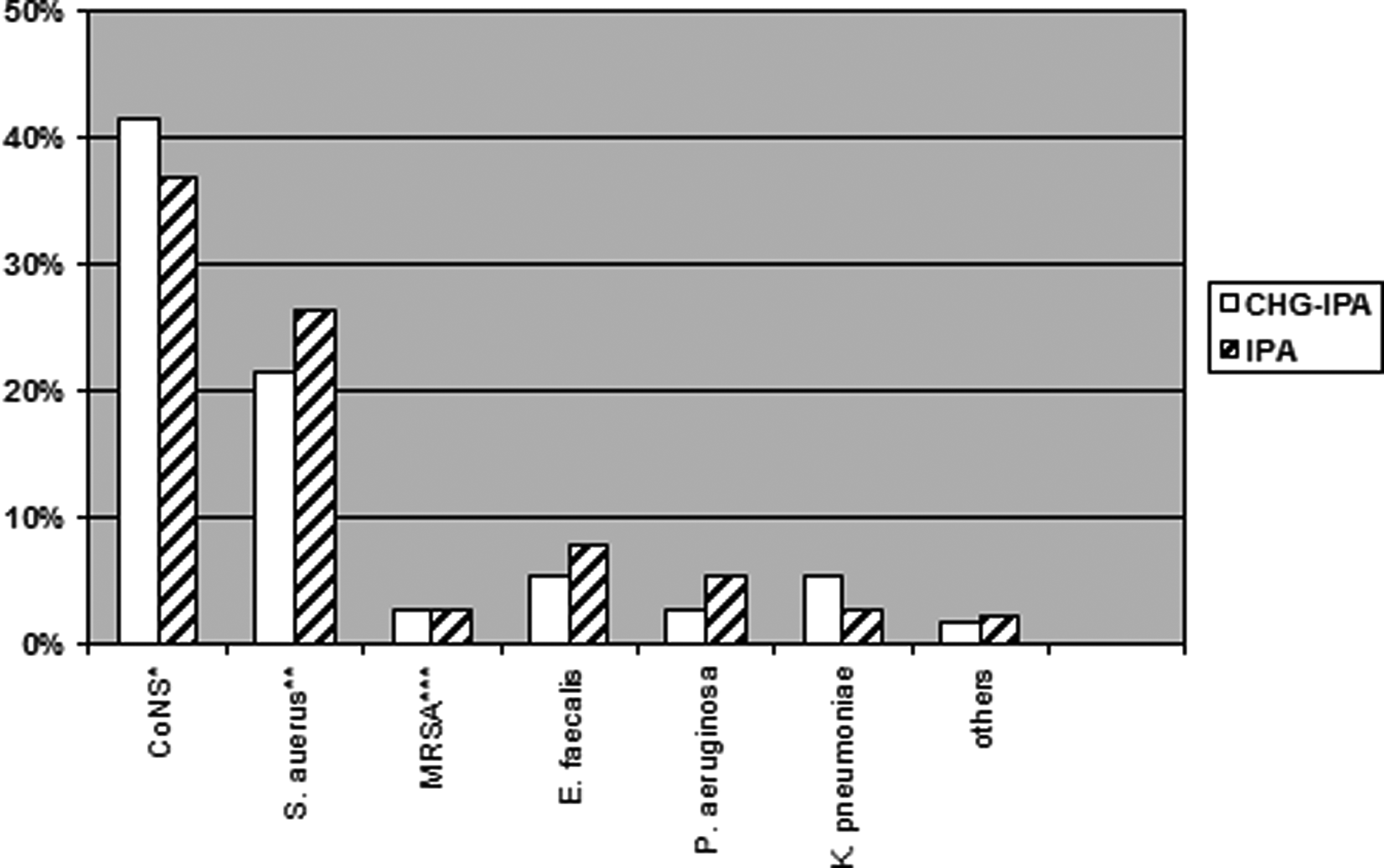
Pathogens causing SSI. Multiple pathogens in one patient possible. No significant difference between cohorts (p = 0.7033). *Coagulase negative staphylococci. **Methicillin sensitive Staphylococcus aureus. ***Methicillin resistant Staphylococcus aureus.
SSI = surgical site infection
Any deviation from normal sternal surgical incision healing documented by surgical incision nurses, excluding mediastinitis.
All-cause death on the day 30 after surgery.
Overall in-hospital death in patients with SSI.
Discussion
Given the large number of skin antiseptics and many factors influencing development of SSI, there is a lack in evidence for the most appropriate pre-operative skin disinfection agent. Neither the CDC nor the Robert Koch Institute in Germany issued a clear recommendation for which single antiseptic or combination of agents should be used for pre-operative skin preparation.
The level of surgical field contamination is a major factor determining the incidence of SSI. The CDC divides surgical procedures into four classes with regard to contamination: 1) Clean, 2) clean-contaminated, 3) contaminated, and 4) dirty or infected surgery [4]. Although cardiac surgery is categorized as a clean surgery, patients are increasingly at high risk for SSI development [1].
In clean surgery, several randomized trials evaluated the effectiveness of different types of skin antiseptics. In the 2013 Cochrane Collaboration comprehensive review, 13 prospective controlled trials were included involving a total of 2,623 participants [5]. Only one study demonstrated a substantial reduction in SSI with use of chlorhexidine in alcohol compared with iodine antiseptic [6]. However, the study lacked detailed description of interventions and was classified as being at unclear risk of bias. In the Cochrane meta-analysis, comparison of mixed antiseptic treatment suggested that alcoholic solutions, and especially 4% chlorhexidine in 70% alcohol, had the greatest probability of being effective, but the quality of evidence was judged as low because of the limited number and size of studies [5]. In our study, we calculated the expected incidence of PSM at 3.2% (using the calculation of Fowler et al. [7]) and conducted a trial with nearly 3,000 patients to reach appropriate statistical power for this endpoint.
In clean-contaminated surgery, a large randomized trial comparing povidone-iodine with chlorhexidine-alcohol in 849 patients [8] showed a 41% risk reduction of SSI in the alcohol-chlorhexidine group. This was the first study with a high level of evidence showing a substantial advantage of chlorhexidine in alcohol against iodine.
Dissimilar to the U.S., alcoholic solutions, rather than iodine, are more commonly used in Germany. Although both agents have a broad antimicrobial spectrum [9], alcohol possesses more rapid action compared with iodine [10]. Chlorhexidine has the advantage of persistent activity despite exposure to body fluids and residual activity for up to 48 h [2].
At our institution, IPA was a standard pre-operative antiseptic. We hypothesized that the addition of CHG to IPA would help to reduce SSI, especially the incidence of PSM. The present single-center, prospective cohort study was conducted during 27 mo and included a majority of patients undergoing cardiac surgery with median sternotomy. Both registries were well matched regarding known pre-operative and intra-operative risk factors (Table 2 and 3).
After the operation, sternal surgical incisions were precisely monitored by surgical incision nurses and a senior cardiac surgeon (TW). Any sign of abnormality was documented and specifically classified as an SSI. For the purpose of this study, observed SSI were divided into post-sternotomy mediastinitis according to CDC criteria [3] and SSI of any other kind. Surgical site infection of any other kind included any other deviation from normal surgical incision healing, documented by surgical incision nurses.
Management of surgical incision infections followed institutional standards. All deep SSI were treated surgically in general anesthesia using temporary vacuum-assisted closure (VAC™). Majority of documented SSI of other kind was a temporary secretion from the surgical incision or minor skin dehiscence, which resolved without further therapeutic action. Some patients with superficial infections (25%) required local surgical therapy with or without temporary superficial VAC.
There was a relatively high expected incidence of major sternal infection, as predicted by Fowler combined score [7] in the study population. Calculated risk of PSM reached 3.1% and 3.2% for registry 1 and 2, respectively. After analysis of 30-d follow-up the major finding of this study was shown: Observed PSM rate was substantially lower in registry 1 (1.9%) versus 4.2% in registry 2, p = 0.0009. Surprisingly, SSI of any other kind were not different among groups (11.2% vs. 10.5%; p = 0.5441). Decrease in mediastinitis in CHG-IPA cohort was obviously not because of effect on single specific bacteria, as the spectrum of isolated species was similar in both groups of patients with positive bacterial culture (Fig. 2).
From overall 91 patients suffering from mediastinitis, five patients (5.5%) died during the hospital stay (three patients in registry 1 and two patients in registry 2). We did not observe a substantial difference in 30-d survival and mean in-hospital length of stay.
Limitations of the study
The main limitation of this study is its non-randomized design because of funding reasons. Nevertheless, registries were well comparable regarding patient demographics and risk factors. Another study limitation was the difference in alcohol concentration between the two products. In registry 1, 70% IPA and 2% CHG were used, whereas in registry 2, 55% single IPA antiseptic was used. On the basis of available data, it is not possible to conclude whether the reduction in the mean PSM rate in registry 1 was because of the use of CHG, the greater alcohol concentration, or the additive effect of CHG with IPA.
Conclusions
The findings of this prospective cohort study support the hypothesis that pre-operative skin disinfection with chlorhexidine in alcohol (ChloraPrep) compared with alcohol only (Kodan) effectively reduces the rate of post-sternotomy mediastinitis in cardiac surgery. Further studies are required to evaluate the role of alcohol concentration and to compare chlorhexidine in alcohol versus chlorhexidine in iodine in cardiac surgery.
Footnotes
Acknowledgments
The authors thank Gisela Behr and her team for documentation.
Author Disclosure Statement
All named authors have seen and agreed to the submitted the version of the paper and the material is original, unpublished, and has not been submitted elsewhere. All of us disclose any commercial associations that might create a conflict of interest by submitting this manuscript. There is no funding for this research.