
Abstract
Abstract
Background:
Surgical site infection (SSI) is one of the main causes of morbidity and death after surgical intervention. The use of physical barriers, including gloves, drapes, and gowns to reduce SSI after abdominal surgery is long-standing practice. The aim of this systematic review and meta-analysis was to determine the efficacy of ring incision retractors in reducing the risk of SSI in abdominal surgery.
Methods:
PubMed, CINAHL, the Cochrane randomized controlled trials (RCTs) Central Register, and the ISRCTN registry were searched for RCTs in which ring retractors were utilized to reduce SSI in abdominal surgery. The PRISMA guidelines and RevMan 5.3 were used for study selection and analysis. Additional subgroup analyses were performed, including trials using incision class (clean, clean-contaminated contaminated, and dirty) and trials that used the U.S. Centers for Disease Control and Prevention's SSI definition in their protocol.
Results:
A total of 19 RCTs inclusive of 4,229 patients were included. The utility of ring retractors in reducing SSI was suggested by an overall risk ratio of 0.62 (95% confidence interval 0.48–0.81). However, study heterogeneity caused by differences in effect size between individual RCTs, the non-standardized utilization of concomitant measures to reduce SSI, and an overall lack of high-quality trials was found.
Conclusion:
A reduction in SSI incidence with the use of ring retractors is suggested by the findings. However, this result must be treated with caution because in addition to some old trials poor quality and the large number of factors affecting SSI, there were substantial differences between trials in effect sizes in statistical heterogeneity. Further RCTs are needed to confirm this provisional finding.
S
Two main types of ring retractors are available [4] (Table 1). Double-ring retractors; e.g. Alexis® (Applied Medical, Rancho Santa Margarita, CA), are cylindrical, clear plastic devices that are fitted through the incision and held in place by inner and outer rings. For laparoscopic procedures, the plastic sheath can be clipped or plugged using a GelPOINT advanced-access platform to maintain pneumoperitoneum [5] and, in some cases, to aid in specimen retrieval [6]. In the single-ring design, the outer ring is replaced by a plastic sheath that is extended to roll over the incision edges.
Two previous systematic reviews of this topic were discovered during a literature search for this meta-analysis. Eleven of the 19 trials included in the present review also were included in these previous systematic reviews in which non-randomized clinical trials also were analyzed [4,7]. However, since their publication, several further trials have been reported, and their conclusions reached no consensus regarding the utility of retractor usage, with the conclusions ranging from support for retractor use to requests for further studies to answer the question. The aim of this review was to aid in the further evaluation of the effectiveness of ring retractors in halting SSIs, which may reduce morbidity and death.
Patients and Methods
The systematic review and meta-analysis were performed according to the PRISMA guidelines [8]. The protocol was not registered in an online database (Supplement 1).
Eligibility criteria
Databases were searched for randomized controlled trials (RCTs) that compared ring retractors with conventional retractors or surgical drapes in elective and emergency abdominal surgery. We defined abdominal surgery as laparotomy or any operation involving the abdominal and pelvic cavities via trans-abdominal wall incisions. An SSI was defined as the presence of ≥1 of the U.S. Centers for Disease Control and Prevention criteria listed in Table 2 [9]. Trials involving either single- or double-ring retractors were included. Non-randomized trials, systematic reviews, case reports, retrospective studies, case series, and studies involving abdominal surgery for penetrating abdominal injuries were excluded.
SSI = surgical site infection.
Database search
PubMed, Cochrane Library (central register of controlled trials), CINAHL Plus database, and the ISRCTN registry for unpublished registered RCTs were searched between December 19, 2014 and March 3, 2015. The search terms used for the different databases are listed in Table 3.
Study selection
Article titles were scanned to identify studies that compared surgical ring retractors with conventional retractors or surgical drapes vs. no intervention for the outcome of SSI in patients undergoing abdominal surgery. Full abstract review was then carried out for potential studies. Eligible full articles were examined according to the inclusion and exclusion criteria. Figure 1 shows the flow diagram for the search and selection process.
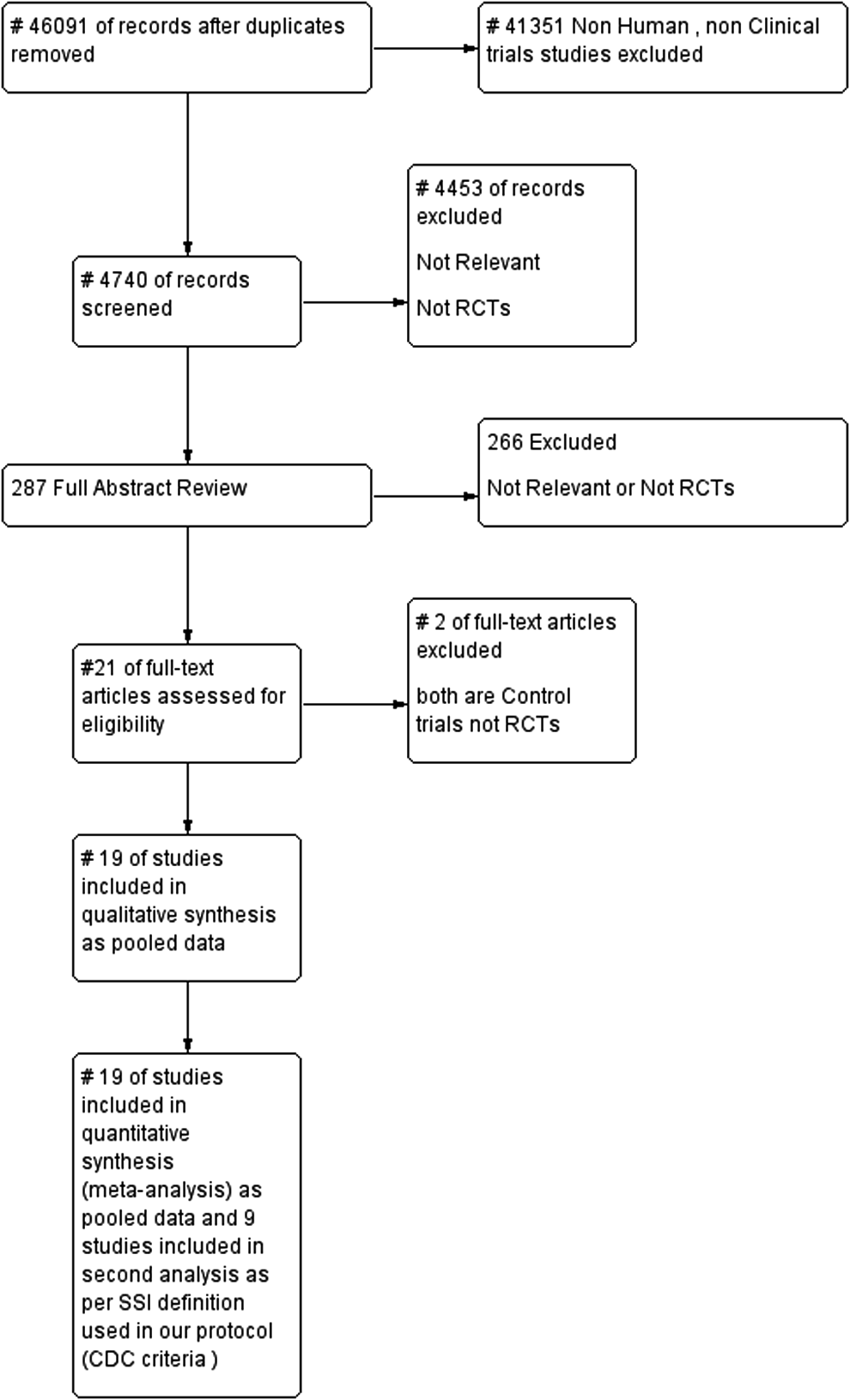
Flow diagram for search and selections processes.
Data extraction
Data were extracted for all studies by the first author. Another author (K. Bashar) ran an independent risk of bias analysis and data accuracy verifications. In addition to the primary outcome, the flowing study design data were recorded: Participants, number and demographics, exclusion and inclusion criteria, secondary outcomes, intervention(s), trial arm, and control groups. Factors that may affect the primary outcome also were recorded. These include: SSI definition used, skin preparation before incision, details of pre-operative and post-operative antibiotic usage, type of operation, and additional preparation used to decrease bacterial load pre-, intra-, or post-operatively. In trials with more than two arms, we included the retractor and control or conventional arms only. Two authors (D.T. and S.A.) were contacted to obtain more information on their studies. Each responded with the requested information on length of followup and incision class.
The Cochrane Collaboration's tool for assessing the risk of bias, RevMan 5.3, was used to evaluate individual studies and to generate a color-coded risk-of-bias table. Where the author did not clearly specify how he or she addressed any of the risk domains, the denotation of “unclear risk” was given. We acknowledge that performance bias is always unclear because of the technical inability to blind the intervention group during an operative procedure.
Publication bias
Funnel plots were created for the visual assessment of any asymmetry in the distribution of studies by size and their effect measures around the average, which may highlight differences between studies and the possibility of publication bias.
Statistical approach
RevMan 5.3 also was used to analyze the pooled data from all studies. The risk ratio (RR) was calculated using a random-effect model with the 95% confidence interval (CI). The CI alignment in the forest plot visually aids in the assessment of consistency within studies. The χ2 test was used to assess statistical heterogeneity. As the χ2 test is lower powered when small trials are included, the I2 test was used to quantify inconsistency across studies, and the results were evaluated against p values from the χ2 test [10].
Additional analyses
Additional subgroup analyses were performed for:
1. Studies classified by incision type (clean, clean-contaminated, contaminated, and dirty) to evaluate the effect of the degree of contamination on the incidence of SSI. 2. Studies that used the CDC definition for SSI as a standardized method.
Results
Study selection
After the exclusion of two trials lacking randomization [11,12], 19 studies were included in our systematic review [11–33]. Three of the fully reviewed studies required translation (Silva et al. in Spanish [32], Batz et al. in German [15], and Brunet et al. in French [11]). We first included all studies that used any of the CDC SSI criteria to perform pooled data analysis and then identified trials that used the CDC criteria for a subgroup analysis. In RCTs with more than two arms, we included only the retractor arm and the control or conventional arm.
Characteristics of the studies
The characteristics of the RCTs included are provided in Table 4. Factors that may influence the SSI rate in the studies are listed in Table 5. Four trials were multi-center, the remainder being single center. Differences in age and other inclusion/exclusion criteria were evident between the studies (see Table 4).
Studies that used the Centers for Disease Control and Prevention (CDC) criteria for surgical site infection (SSI) in the sub-analysis are marked *.
ASA = American Society of Anesthesiogists, LOS = length of stay; RCT = randomized controlled trial.
CDC = U.S. Centers for Disease Control and Prevention; IV = intravenous; LRTI = lower respiratory tract infection.
Participants
There were 4,229 patients in the 19 trials. The sample size ranged from 50 patients in the smallest, single-center trial (Batz et al. [15]) to 735 in the largest, multi-center trial (Pinkney et al. [19]).
Interventions
Twelve trials used single-ring retractors, whereas seven used double rings. One of the double-ring groups used a modified Alexis retractor (Ozer et al. [16]), whereas another made the retractor locally using two rings and surgical gloves (Silva et al. [32]). All others used standard double-ring retractors.
Outcomes
All trials designated SSI as the primary outcome. The SSI definition and the reporting and duration of post-operative follow-up were substantially different in various trials.
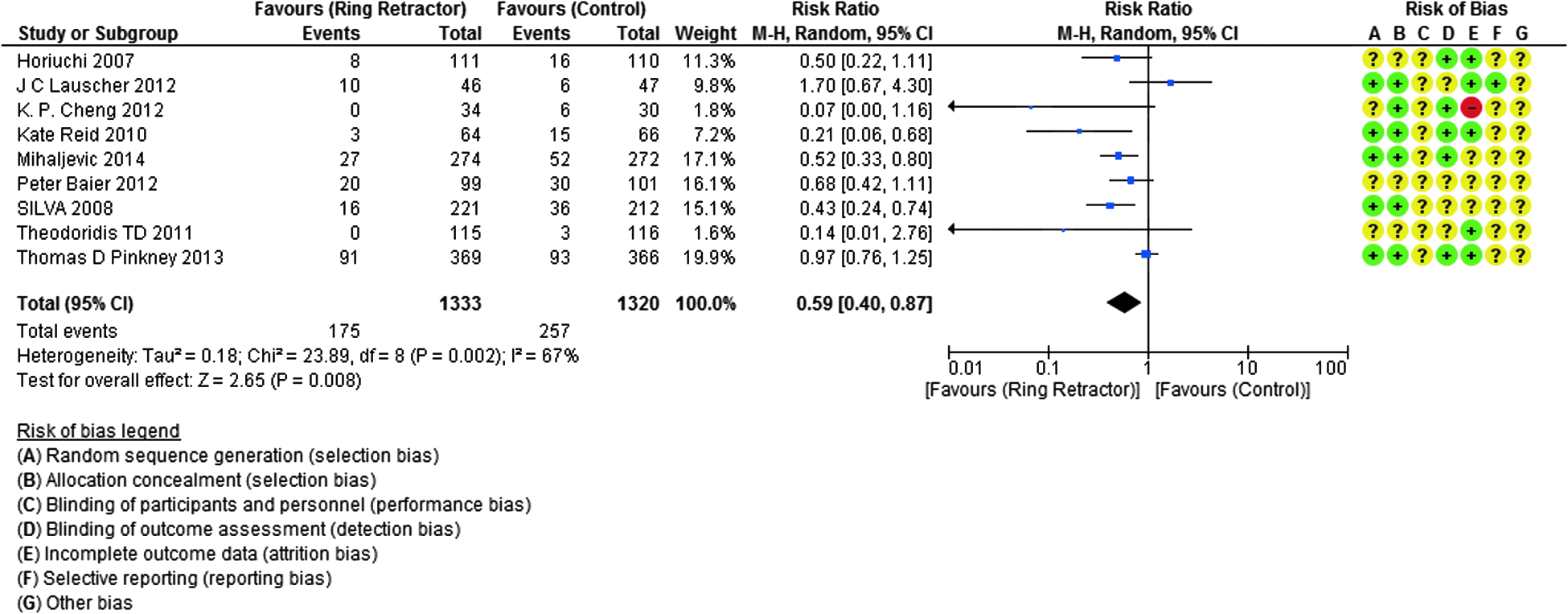
We performed a subgroup analysis inclusive of the nine trials that specified the CDC criteria as the definition of SSI (Fig. 6). One trial (Lauscher et al.[22]) used modified CDC criteria by physical examination at 10 d and telephone followup at 1 and 6 mos.
Control group
The designation of the control group was assigned to the cohort without intervention with ring retractors. Conventional drapes and retractors were used according to the different hospital protocols.
Reported confounders that may influence SSI rates
Antibiotic usage
There was substantial variation between trials in antibiotic usage in the pre-operative, intra-operative, and post-operative periods. There was not enough documentation for antibiotic usage comparing the control and intervention groups. Some trials did not specify their prophylactic antibiotic dose and timing (n = 7), and others used antibiotics according to surgeon preferences or intra-operative findings (n = 2). We summarize these findings in the first column of Table 5.
Preparation
The main skin preparation material was povidone-based solution. Other trials added extra skin closing techniques to decrease contamination. At least one trial used locally applied antibiotics. Additional preparations were applied to decrease the bacterial load: Bowel preparations, washout, and change of contaminated gloves in addition to other methods, especially in colorectal surgery.
Surgical interventions
Trials included patients undergoing appendectomy (n = 4), colorectal resection (n = 6), a gastrointestinal procedure (n = 3), a mixed abdominal operation (n = 5), and cesarean section (n = 1).
Risk of bias assessment
We conducted a risk-of-bias assessment for the individual studies using the Cochrane assessment tool within RevMan 5.3 to produce a color summary and graph (Figs. 2 and 3).

Risk of bias assessment for all trials combined. Color image is available online at www.liebertpub.com/sur
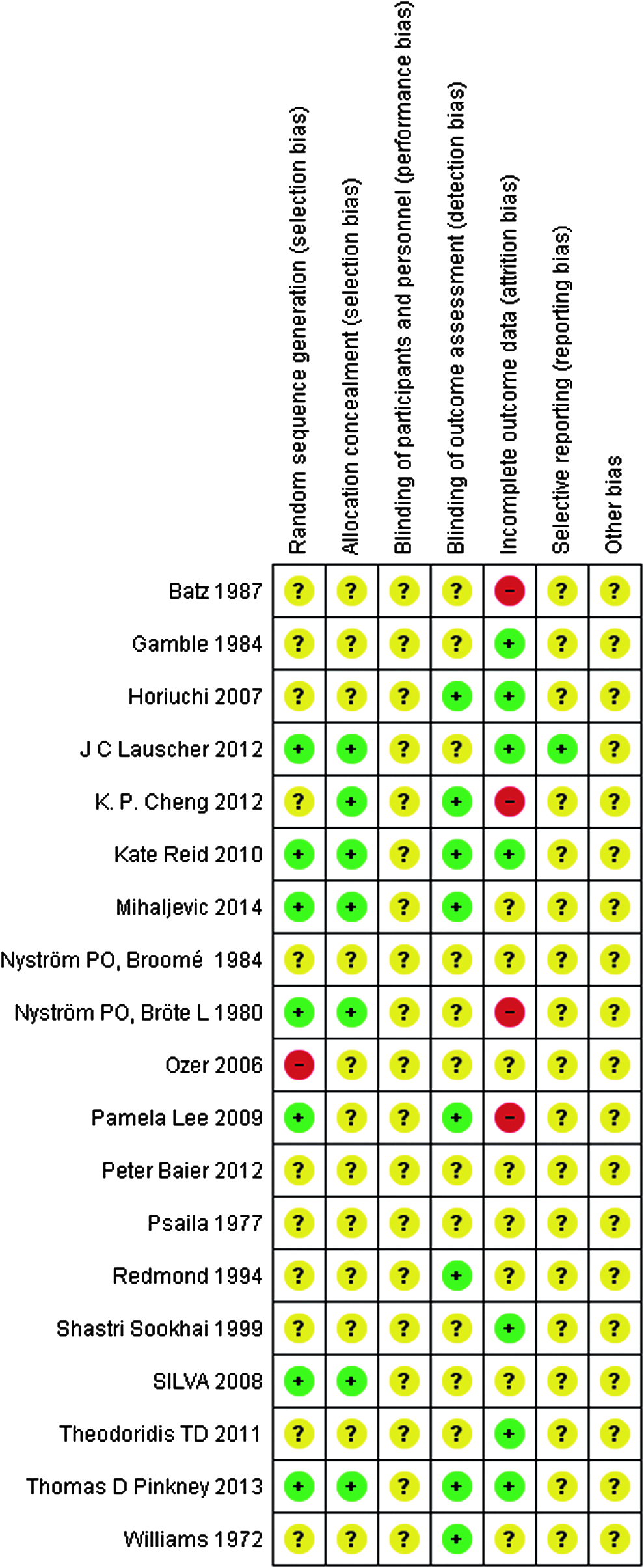
Summary of risk of bias assessment for individual trials. Color image is available online at www.liebertpub.com/sur
Random sequence generation
Most of the studies, especially the older trials, demonstrated an unclear to high risk of bias. One trial used alternating patient assignment to the two arms of the trial (Ozer et al. [16]).
Allocation concealment
Whereas six of the trials addressed this issue, in the majority of the trials, there was no clear information about blinding. We agree that blinding is technically difficult or impossible, given the nature of the tested intervention. However, the risk of favoring one arm is obvious.
Blinding of outcome assessment
Eight of the studies assigned blinded assessors.
Attrition bias
Six studies succeeded in preventing attrition, whereas four studies showed a high risk of bias because of number discrepancy. The rest of the studies showed unclear risk because of the number of patients lost to follow-up or, in one case, a crossover of patients between the two study arms after the study was started [13].
Selective reporting
The risk of selective reporting was unclear in all the trials.
Other bias
The risk of other biases is unclear in all studies because of the large numbers of confounders of SSI.
Publication bias
A funnel plot was created to assess the risk of publication bias (Fig. 4). The overall asymmetry can be explained by differences in study sizes and their effect measures. The asymmetry observed in the left lower aspect of the plot accommodates three studies (Cheng et al. [17], Ozer et al. [16] and Theodoradis et al. [18]). All these are small and favored the ring retractor, suggesting publication bias. However, all three trials were within the 95% CIs, suggesting low precision of effect estimate to cause this asymmetry. The RR (95% CI) were 0.07 (0.00, 1.16), 0.10 (0.01, 1.83), and 0.14 (0.01, 2.76), respectively.
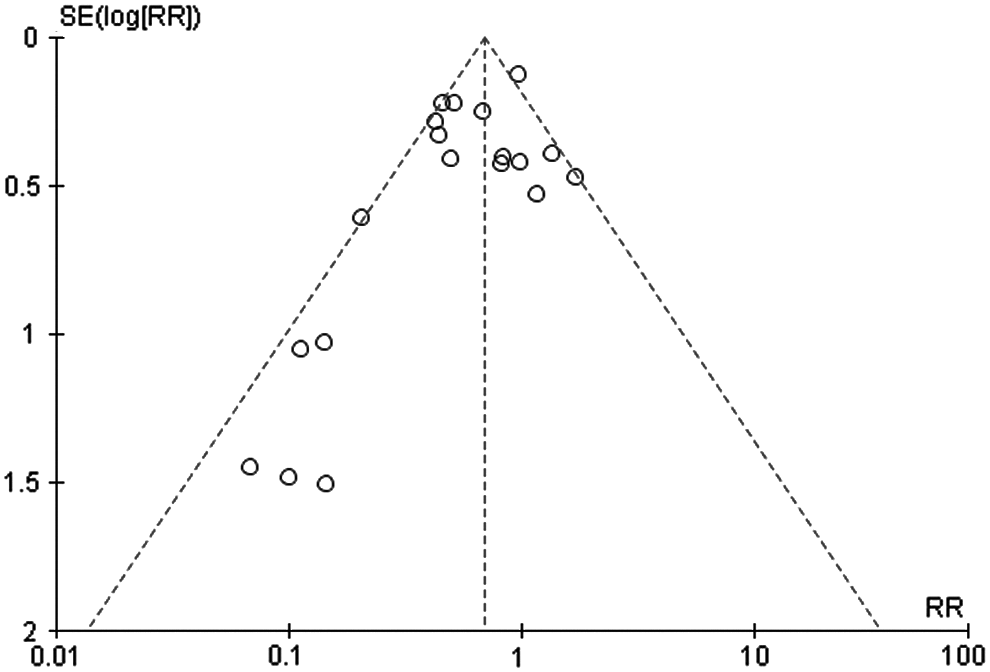
Funnel plot of comparison of ring retractor vs. control for the outcome of surgical site infections.
Pooled data analysis
The studies ranged from having an unclear to a high risk of bias. We first calculated RR with 95% CI for the pooled data from all studies using random-effect models (Fig. 5). We then performed the same analysis for the trials that specified the use of CDC criteria to define SSI (Fig. 6). The nine studies that fulfilled the CDC criteria are more recent and addressed more risk-of-bias domains compared with the older studies. The overall results were RR 0.62, 95% CI 0.48, 0.81 and RR 0.59, 95% CI 0.40, 0.87 for the CDC sub-group with no marked differences between the two, both favoring ring retractors.
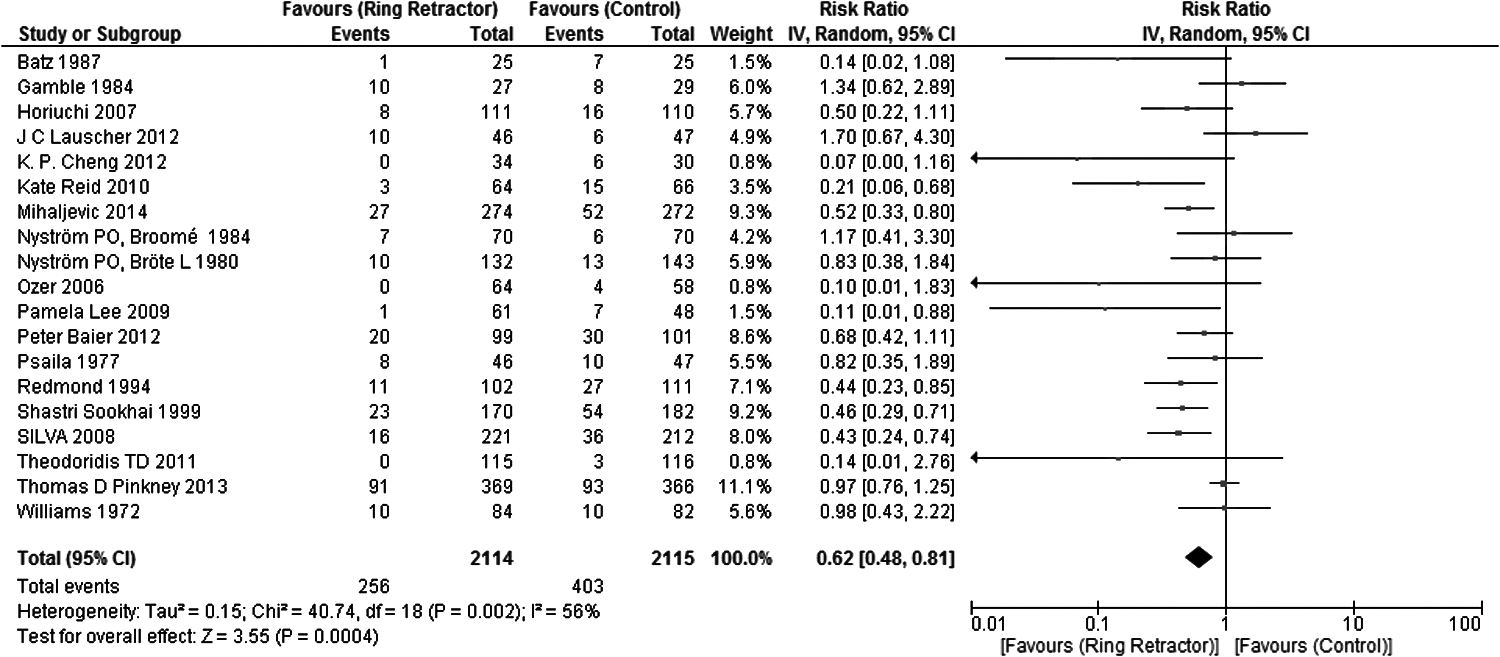
Forest plot of comparisons of all studies inclusive of ring retractor vs. control groups for the outcome surgical site infections.
Forest plot of comparisons between studies using Centers for Disease Control and Prevention criteria to define SSI with ring retractor vs. control with the outcome of surgical site infection.
Additional Analysis
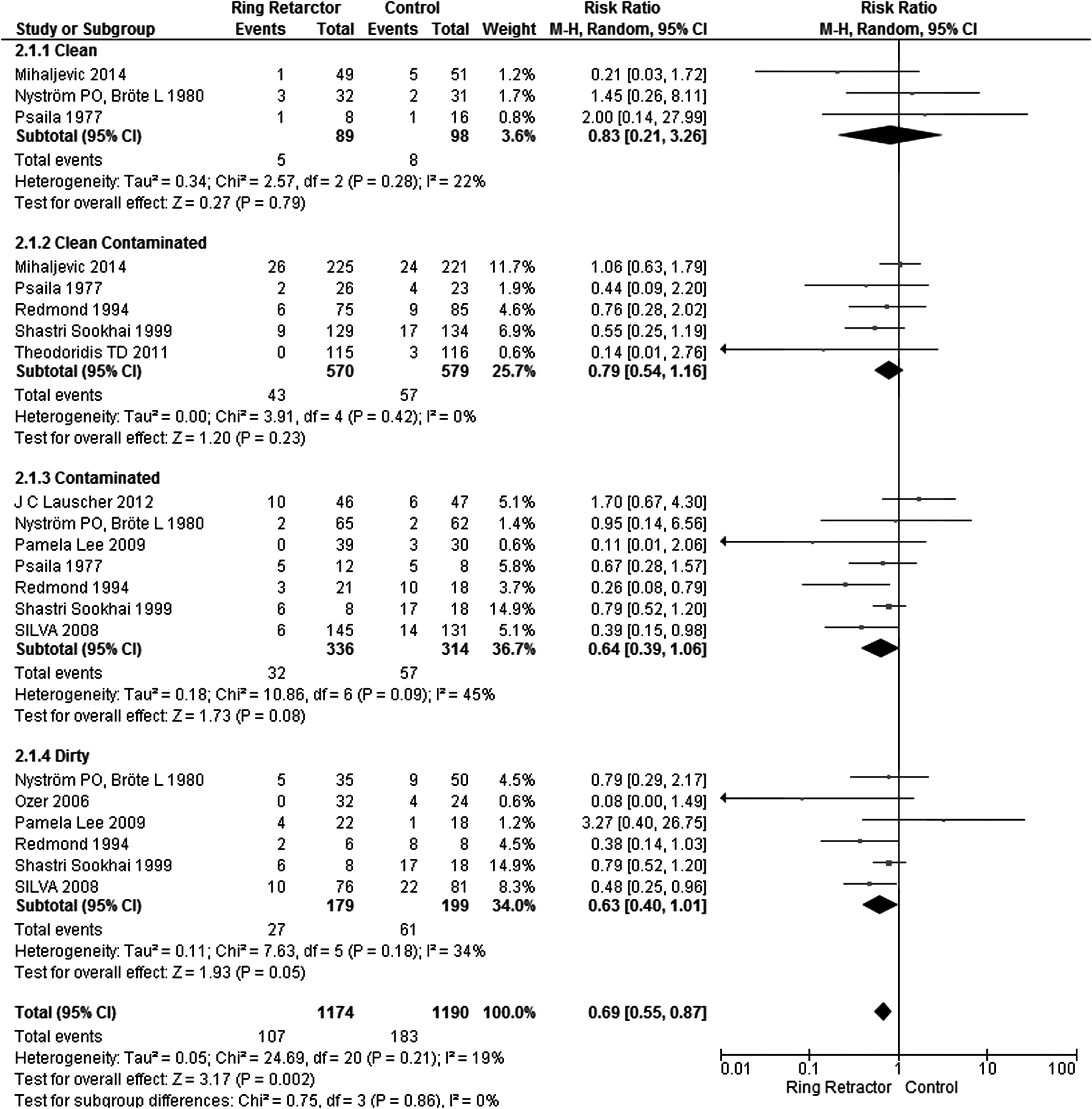
We conduct sub-group analysis for studies by incision classification (Fig. 7). When no information was provided or surgery could not be categorized under any class, the data were not analyzed.
Forest plot of comparisons of studies by classification of incisions with ring retractor vs. control for the outcome surgical site infections. Color image is available online at www.liebertpub.com/sur
The ring retractor seems to be more effective in the dirty-incision group, but there was no substantial evidence of this, with the pooled effects almost touching the no-effect line. In the random effects model, the clean incision group had an RR of 0.83 (95% CI 0.21, 3.26), the clean contaminated group had an RR 0.79 (95% CI 0.54, 1.16), the contaminated group had an RR of 0.64 (95% CI 0.39, 1.06), and the dirty group had an RR of 0.63 (95% CI 0.40, 1.01).
Discussion
Summary of evidence
This systematic review of 4,229 patients involved in 19 RCTs provides some evidence that SSI is reduced by using ring retractors. The overall pooled effects favored ring retractors (RR 0.62; 95% CI 0.48, 0.81), and limiting the RCTs to those that used the CDC criteria produced a similar effect size (RR 0.59; 95% CI 0.40, 0.87).
The incision classification sub-group analysis suggests that retractors may be more effective in relation to the degree of contamination. Contaminated and dirty procedures showed more benefits from using ring retractors than did the clean and clean contaminated procedures, but the numbers are small (Fig. 7).
These results should be treated with caution, as there is significant heterogeneity in the pooled results. This may be attributable to differences in RCT quality (see risk of bias in Fig. 3), differences in populations of patients in terms of incision contamination (Fig. 7), and differential use of antibiotics in terms of type, administration time, duration, and management protocol of SSI (see Table 5).
Context of previous studies
Two previous systematic reviews collectively included 11 of the 19 studies we reviewed [4,7]. Another systematic review published on March 27, 2015, after our final search, includes 16 trials [14]. The conclusion of these reviews ranges from the need for more high-quality RCTs [7] to support for the use of the retractors in non-trauma abdominal operations [4] and suggesting strong evidence of site protector effectiveness compared with standard care [14].
In our review, there was significant variation between trial inclusion/exclusion criteria, skin preparations, use of antibiotics, bowel preparation before colorectal surgery, and length of followup. The SSI definition was not unified among trials, and only nine trials used the CDC criteria. Other trials used a wide variety of clinical findings to define SSI (see Table 4), with one trial [15] depending mainly on overt pus and microbiologic findings.
Interestingly, the trials extend from 1972 to 2014, and we observed significant improvements through time in terms of design, identifying confounders, and addressing risks of bias. Overall quality assessment of the trials ranges from moderate to a high risk of bias (see Figs. 2 and 3). The observed funnel plot asymmetry can be attributed to the number of small trials favoring ring retractors [16–18], with one of the large trials touching the no-effect line [19].
Clinical implications of results
Our review suggests some benefit for ring retractors in the reduction of SSI. The device has been used clinically for a long time with a good safety profile, but we need more studies to test these results. We need to standardize antibiotic usage protocols, skin preparations, other infections confounders (e.g., diabetes mellitus, immunosuppressive drugs), and type of procedure.
Strengths and weaknesses of this review
The main weakness of our systematic review is the poor quality of most of the trials. Abdominal surgery includes a range of interventions that may add more SSI confounders, depending on the intra-operative findings, duration, and how much manipulation was done during surgery. In addition, combined procedures in five trials (upper and lower gastrointestinal), unclear randomization methods in 11 trials, and non-standardized usage of antibiotics, added to the fact there was no or scattered documentation for these confounders among the studies (with the exception of more recent trials), cast a shadow on SSI risk stratifications and hence create a need for caution dealing with these results.
The strength of this review is the inclusion of randomized trials only in accordance with PRISMA guidelines, which may reduce the risks of bias usually observed more in other types of studies. In addition, there was no language restriction, as we translated reports from German, Spanish, and French. The authors were directly contacted for further information when needed, and we got a 66% response rate.
Implications for future research
We believe that this result may provoke more research in this area, and more surgeons may be interested in exploring the potential effectiveness of ring reactors in reducing SSI.
Conclusion
Ring retractors appear to reduce the risk of SSI. However, this result must be treated with caution because most of studies we examined were of poor quality. In addition, there are substantial differences between trials in effect sizes, which results in statistical heterogeneity. Further RCTs are needed to confirm this provisional finding.
Footnotes
Author Disclosure Statement,Funding,and Acknowledgment
The authors declare no conflict of interest. The first author, K. Ahmed, is supported by National University of Ireland Galway.
We acknowledge the great help from research librarians in James Hardiman Library National University of Ireland Galway.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.