
Abstract
Abstract
Background:
The risk of exposure of either the patient or the surgeon to communicable disease when the surgical glove is perforated is important. Both patients and the surgical team need to be protected from this risk. Therefore, we intended to determine the efficacy of double gloving in our center.
Methods:
This was a prospective cohort study, involving (randomly selected) surgeons, who wore single or double latex surgical gloves during procedures. Gloves were collected and evaluated for perforations (using air insufflation and water leak methods).
Results:
A total of 1,536 gloves were collected (512 single gloves and 1,024 double gloves), with 78 of 512 gloves perforated, giving a rate of 15.2%. Perforation rate was 15.2% in single gloves, 14.4% in double gloves, 15.5% in emergency operations, and 14.3% in elective surgery. It was highest (30.8%) among registrars in training, particularly when doing any deep (16.0%) surgery. Glove perforation rate was highest (17.4%) among general surgery procedures as opposed to pediatric surgery (14.6%), urology (13.9%), neurosurgery (11.7%), and plastic surgery (10.6%), with (42.1%) index finger injury. In unused (control group) gloves, the rate of perforation was (0.8%). There was a substantial difference in the overall perforation rate between single and double glove sets (15.2% versus 14.4%) (X2 = 1748, p < 0.0001). However, among the double set, total gloves [outer and inner set] analysis revealed a perforation rate of 27.5% (141 of 512). Of this set, the number of inner gloves that perforated as a result of a through and through puncture from outer to the inner gloves gave a rate of 1.17% (six of 512). Thus, the protection offered by double gloves was 98.83% (X2 = 280.9, p < 0.0001) even if the outer gloves were perforated.
Conclusion:
The use of double gloves has more than 90% protection to patient and the surgeon. Therefore, wearing double gloves should be encouraged in surgery.
D
Patients and Methods
Study setting
Ahmadu Bello University Teaching Hospital (ABU Teaching Hospital), Zaria, is a 500-bed-capacity tertiary care hospital in the northwest region of Nigeria, established since 1967 to provide excellent/advanced health care to patients, conduct research, and train specialized as well as intermediate level manpower in Nigeria's health care system. The Department of Surgery had more than 26 trained surgeons spread across sub-specialties of gastrointestinal surgery, breast and endocrine, hepatobiliary, surgical oncology, urology, pediatric surgery, plastic surgery, neurosurgery, cardiothoracic surgery, and accident and emergency surgery, with more than 40 surgical trainees. The hospital has a robust five-suite modular theater with an operating turnover of approximately 15 patients per day.
Trial design
The study involved a cluster of surgeons, first assistants, scrub nurses, and second assistants who were randomly assigned either single glove pattern or double glove pattern during operative procedures.
The surgical gloves
The surgical gloves (Neogloves) used were made of latex (manufactured for Hertfordshire, WD3 1EF United Kingdom by Ideal Medical Industries Co., Ltd, Lutian base, Poyang industrial zone, Poyang, Shangrao, 333100 Jiangxi Prov. China). The same brand was used throughout the study.
Eligibility
The lead surgeon for each team or specialty had the sole responsibility of constituting and declaring the membership of the operating team of every case, except the scrub nurse, who was chosen by the chief peri-operative nurse. The role designation to each member of the operating team was done by the lead surgeon based on skills, competency, and type of operation or case. However, members and the total number of the operating team varied from case to case, but at any time, consisted of the person operating, which may be a trained surgeon/consultant or a surgeon in training (senior registrar or registrar), scrub nurse, and first assistant. In some cases, depending on the complexity of the case, a second assistant may be part of the operating team.
Randomization
A (1:2 ratio), single blinded randomization of glove pattern into either single or double gloves pattern was done in the immediate pre-operative period (30 min to 1 h of every case/operation).
Intervention
Each member of the operating team, after having been randomly assigned a glove pattern, wore either single glove pattern or double glove pattern during the surgical procedure. Both inner and outer pairs of gloves (for double glove pattern) and pairs of single gloves were tested for perforations after the surgical procedure using two standard methods: The air insufflation (method one) and the water leak (method 2). At the end of the surgical procedure, the observer inspected the participant's hands closely and recorded the presence of blood/fluid or injury on their hands. Members of the surgical team being studied were also asked if they were aware of the occurrence of any glove perforation and associated skin puncture during the operative procedure (for cases that perforation was detected). Records were made of the time of operation, depth and type of surgery, primary surgeon, first assistant, scrub nurse, level of operating surgeon, and specialty. Those who wore double glove pattern were also asked to evaluate the subjective problems of wearing double gloves, which included impairment in tactile sensation and level of comfort.
As control groups, 380 unused gloves (130 single glove pattern and 250 double glove pattern) were tested in an identical fashion for pre-existing leaks and perforations.
Outcomes
The primary outcome measure was glove perforation. The secondary outcome measures were hand contamination with blood/fluid, needle stick, awareness of glove perforation, and the subjective problem of wearing double gloves (tactile sensation and level of comfort).
Analysis
A total of 1536 gloves were collected (512 single gloves and 1,024 double gloves), entered into a spreadsheet and analyzed using SPSS version 20.0 (SPSS Statistics, IBM Corporation, Armonk, New York) and results presented in frequency tables, bar chart, pie charts, and graphs. Level of statistical significance was set at p < 0.05.
Ethical consideration
The ethical committee of the institution approved the study. In addition, verbal permission of participants was obtained after a detailed explanation of the essence of the study, the risks involved including possible contact dermatitis following exposure to the gloves. Assurance was also given that the information derived from the study shall be used solely for the purpose of the research and will not be disclosed or given to a third party. In addition, they were also free to decline to participate or withdraw at any stage of the research.
Results
A total of 118 operations were considered during the study period from May 2013 to December, 2014. Of these total operations, 1,536 gloves (512 single gloves and 1,024 pairs of double gloves) were used. For the single glove pattern, the perforation rate was 15.2% (78 of 512), whereas that of double glove pattern was 14.4% (147 of 1,024). Three hundred and eighty unused (control group) gloves were assessed for evidence of perforation and three (0.8%) were found to have perforated, given a perforation rate of 0.8 (Table 1). There was substantial difference in the overall perforation rate between single and double glove sets (15.2% versus 14.4%) (X2 = 1748, p < 0.0001).
However, among the double set, total glove (outer and inner set) analysis revealed a perforation rate of 27.5% (141 of 512). Of this double set, the number of inner gloves that perforated as a result of a through and through perforation from outer to the inner gloves gave a rate of 1.17% (six of 512). Thus, the protection offered by double gloves was 98.83% (X2 = 280.9, p < 0.0001), even if the outer gloves were perforated.
The characteristics and distribution of perforated gloves based on type of surgery, time of surgery, status of primary surgeon, level of operation, and various specialty is as shown in Table 2. A majority of the perforations occurred during emergency surgery 15.5% (64 of 412), at nighttime 24.7% (70 of 283), when the primary surgeon was a registrar 30.8% (62 of 201) and when the level of surgery was deep 16.0% (99 of 616). General surgery operations recorded the greatest 17.4% (80 of 461) rate of glove perforations, closely followed by pediatric surgery 14.6% (65 of 445).
Eighty-nine (39.6%) gloves had gross evidence of perforation, out of which 47 (20.9% were single gloves, whereas 18.7% were double gloves. One hundred thirty-six (60.4%) gloves had microscopic perforations, out of which 31(13.8%) were single gloves, whereas 105(46.6%) were double gloves. The various sizes of the microscopic perforations are shown in Figure 1 with majority having a perforation of 1–2 mm (microscopic view at power 10). A total of 21 injuries were sustained as a result of various glove perforations; 14 (66.7%) were needle sticks, five (23.8%) instrument injury, one (4.7%) knife cut, and one (4.7%) other. The distribution of injuries to the fingers of the non-dominant hand revealed predominant injury to the index finger (Fig. 2). The duration of the operation appears to have greater influence (sharp increase) on the rate of glove perforation once the duration of the operation exceeded 2 h (Fig. 3). The form of immediate care received following injury is indicated in Figure 4, where the majority of the victims irrigated the injury site with running tap water for 5–10 min before application of direct digital pressure so as to stop the bleeding. None of the victims of needle stick presented or have been reported to have developed a blood-borne disease suspected or attributable to the needle stick.
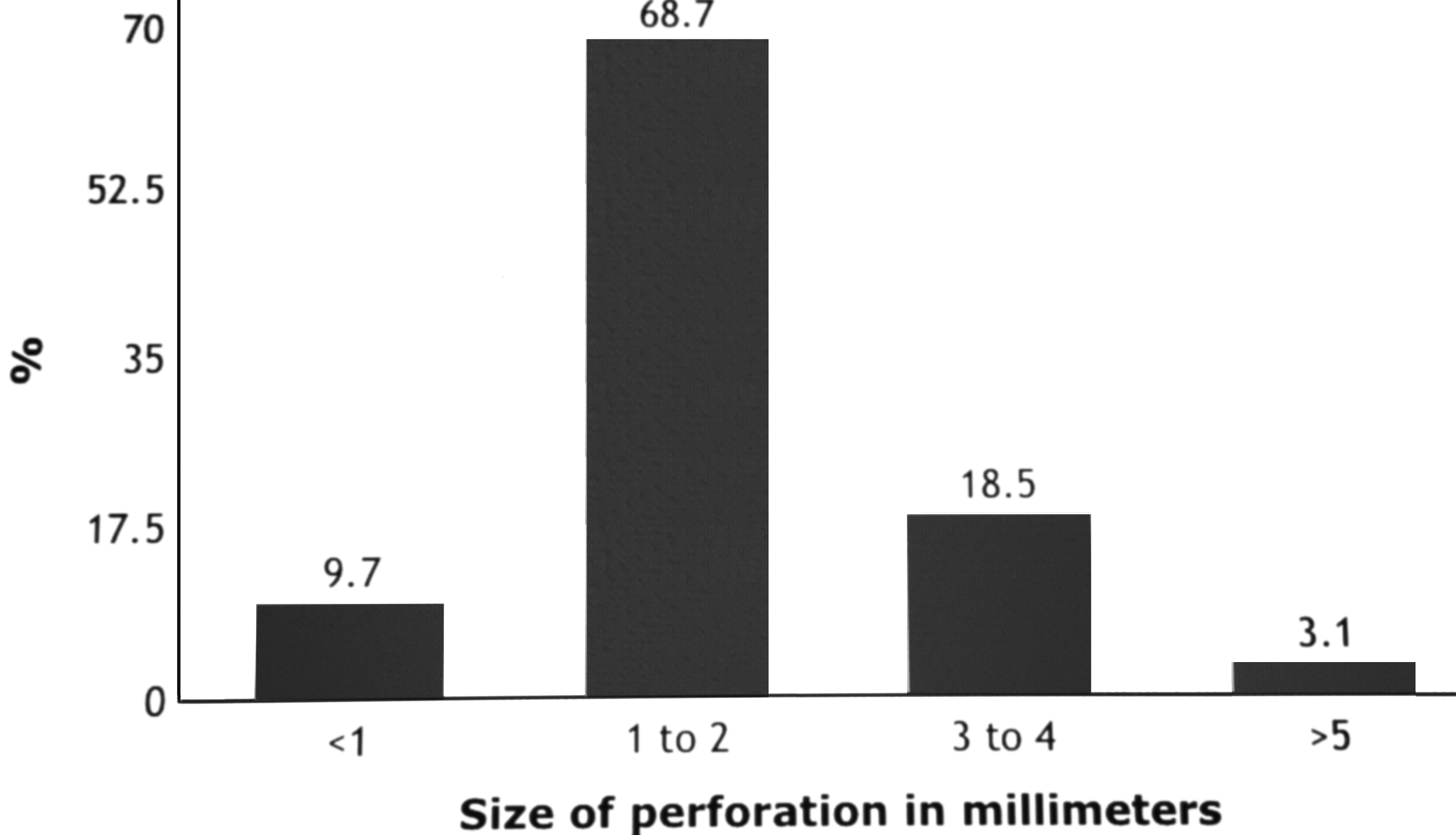
The size of microscopic evidence of glove perforation.

Distribution of injury to the fingers of the non-dominant hand.
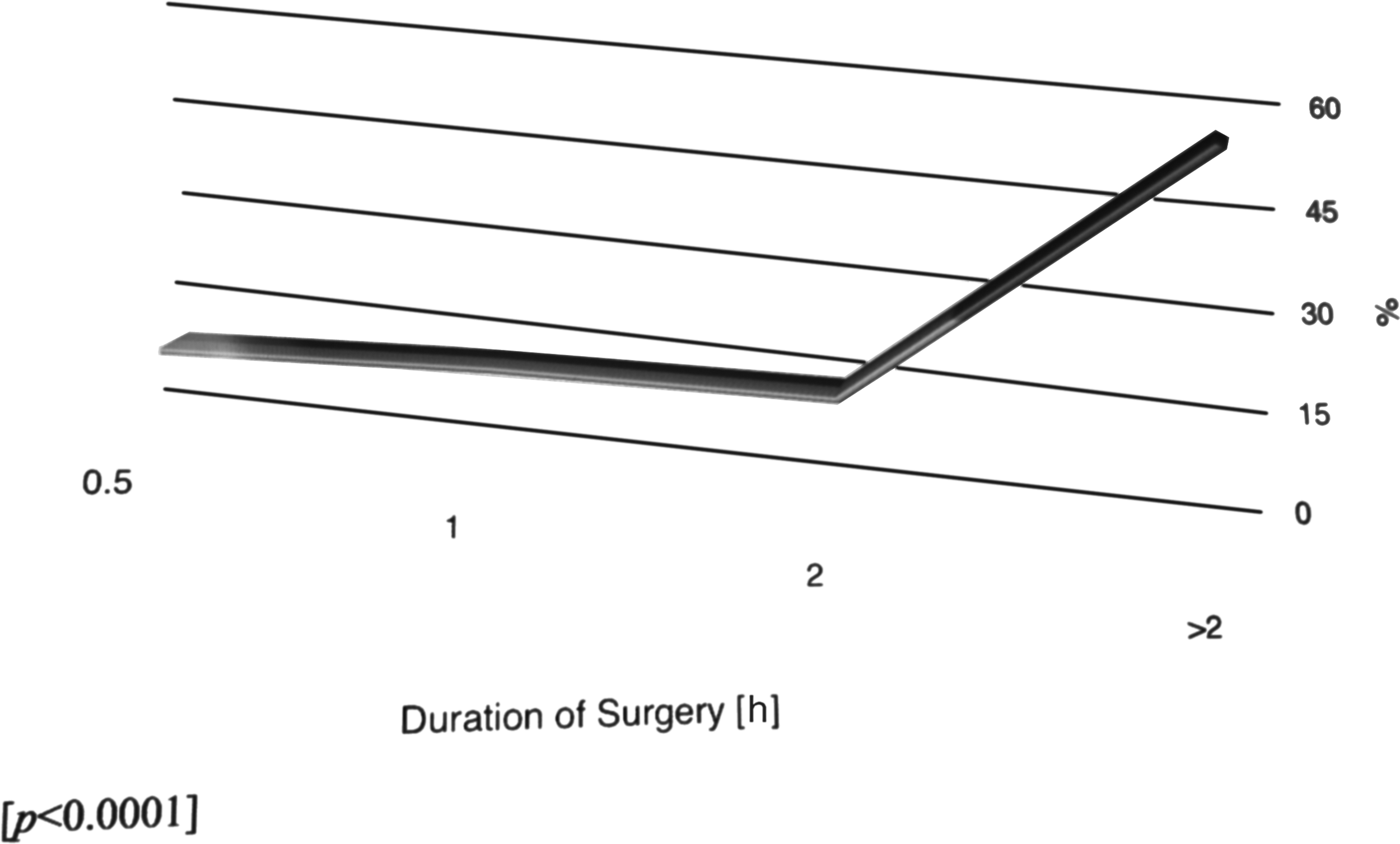
Rate of glove perforation versus duration of surgery.
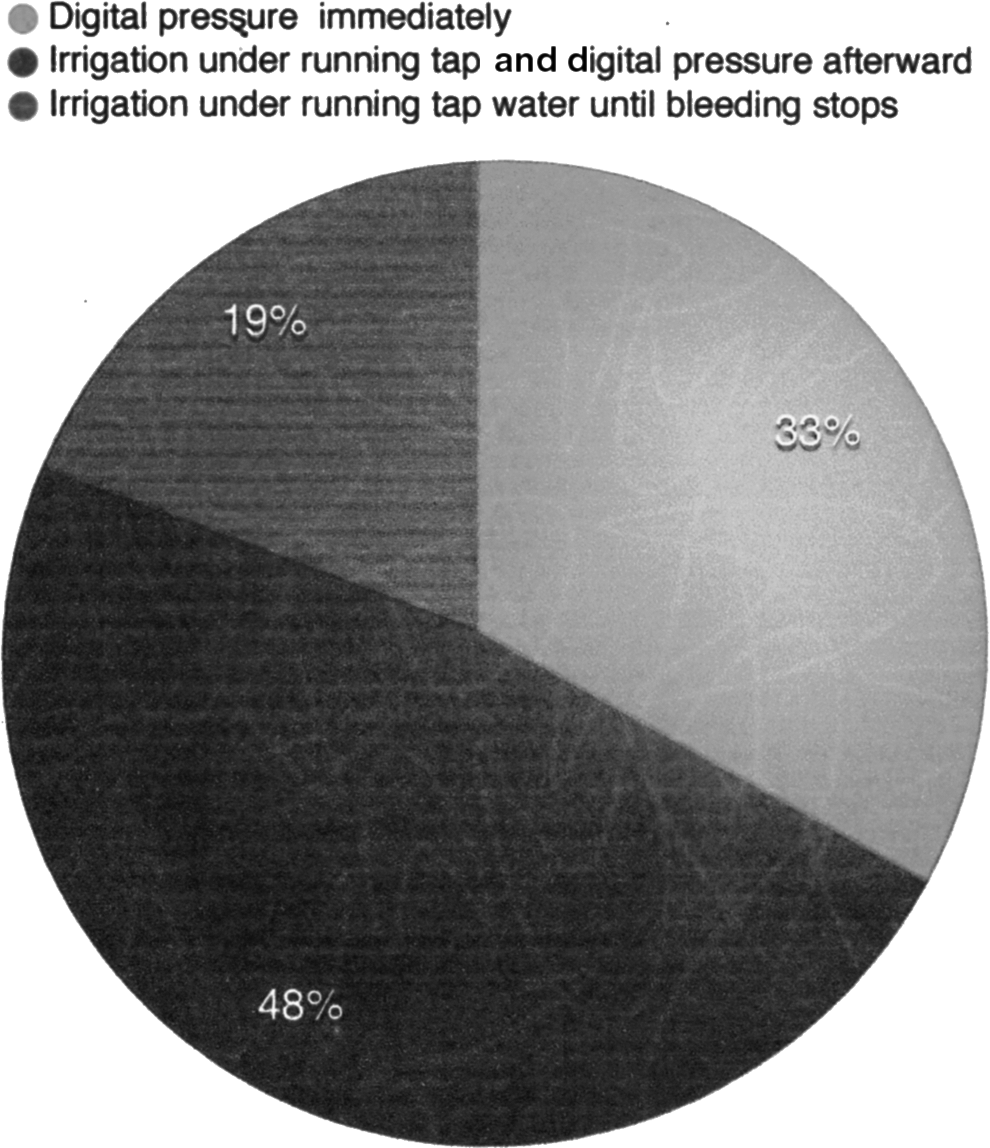
Pie chart showing the form of immediate care received following needle prick.
Discussion
Surgical gloves are well known to provide a mechanical barrier against communicable diseases. Caillot et al. [1], Osman and Jensen [2], and Thomas et al. [4] have reported that gloves could prevent the transmission of micro-organisms not only from the hands of a surgeon to the patient, but vice versa. Pitten et al. [6] and Korniewicz et al. [7] in their respective studies reported that the integrity of the surgical gloves depends on a number of factors ranging from the manufacturer to the duration of wearing, duration and type of surgery performed, and the role of the staff within the surgical team. Similarly, a U.S. Centers for Disease Control and Prevention (CDC) report from 2003 [8] on infection control, and publication number 2004-146 [9] stated that during an operation, any of these factors may be breached and therefore predisposes gloves to a perforation. In addition, once perforation occurs, the integrity of surgical gloves is compromised immediately, which often leads to substantial transmission of micro-organisms from patient's body to the surgeon and vice versa. Tanner et al. [10,11] and Lemaire et al. [12] in their respective studies demonstrated that pooled data from the literature have indicated an average probability of transmission after needle stick exposure of 0.2%–0.5% for HIV-1, 30% for hepatitis B, and between 5% and 10% for hepatitis C. These are common blood-borne infections that are often associated with the risk of glove perforation.
In our study, we found a sharp increase of rate of glove perforations once the operation exceeded 2 h. This was similar to the finding reported by Partecke et al. [13] where a sharp increase of rate of glove perforation was noted once duration of the operation exceeded 3 h. Duration of the operation has been noted to have great influence and thus increases the risk of glove perforation. Laine et al. [14,15] and Harnoss et al. [16] have also reported that the longer the duration of operation, the greater the risk of perforation. In fact, it has been postulated that this may likely be so, because of a low optimal attention that often results from fatigue as the operation progresses. In our study, most of the perforations occurred because of accidental needle stick, though other perforations were because of instruments tearing the gloves. The high risk of glove perforation in prolonged operations has attracted major attention and concern among surgeons—so much so that many have reported and thus, have suggested that gloves should be changed every hour and as long as the operation lasts. Partecke et al. [13] advised that there should be a change of gloves once the operation is likely to exceed 2 h. However, the high economic consequences of frequent change of gloves at every 1 or 2 h period may actually prevent a practical and realistic adherence to this principle, particularly where there is no insurance and in low and middle income societies.
In many cases the perforation of the glove is discovered only when the gloves are removed and blood stain is noted on the hand. Shailesh et al. [17], Hübner et al. [18], and Florman et al. [19] have noted that glove perforation occurs commonly without the wearer's knowledge. It is not surprising, therefore, that in our study, in the majority of the cases of glove perforations recorded, the wearers were not aware of the instance in which it happened except persons/surgeons whose fingers of the non-dominant hand were stuck by a needle. A study done by Dodds et al. [20] demonstrated that this occurs as much as 12% to 17% of the time.
Na'aya et al. [21] and Misteli et al. [22] noted in their reports that surgical glove perforation is often associated with injury to the fingers, particularly those of the non-dominant hand of a surgeon. In our study, we found 21 cases of such injuries and the most common finger affected was the index finger. The most common immediate care received by victims was irrigation under running tap water for 3–5 min before application of digital pressure to arrest bleeding. In fact, in a CDC report of 2003 [8], a non-touch (allow needle stick wound under running tap water) option was recommended because it was assumed that squeezing the tissue during digital pressure would enhance further spread of micro-contamination into the blood circulation, and thus increase the risk of blood-borne infection. Fortunately, in this study, none of the cases presented or have reported to have developed a blood-borne disease suspected or attributable to the needle stick. Perhaps this may lend additional support to the earlier reports [11,12] of low incidence of blood-borne diseases following needle stick or the effectiveness of subsequent and prophylactic care that was often given to victims by the hospital infection control committee.
Carter et al. [23], Barbosa et al. [24], and Driever et al. [25] stated that puncturing of gloves during surgical procedures has been found to occur at rates of 11%–43% depending on the surgical procedures being undertaken. Lancaster and Patrick [26] reported that the puncture rate increases in gloves worn for longer than 3 h. The consequences of glove perforations include injury to the victim, and transmission of infection to surgeon or patient, including high risk of surgical site infection. In our study, the rate of surgical site infection was low and did not correlate well with the rate of glove perforations. However, we noted in cases in which a member of the surgical team had glove punctures, more patients had surgical site infections than in those patients in whom no glove puncture was observed. We were not certain if the slight increase in the rate of surgical site infection was a true reflection of the punctured gloves because we could not rule out the possibility of other risk factors of infection in these patients. The nature of the operation being carried out is probably a substantial factor affecting glove perforations. This is evidenced from the result of our study in which more perforations were found among general surgery procedures and when the surgery was quite deep. In a study done by Laine et al. [27,28], they found orthopedic surgery to have the highest incidence of glove perforation, closely followed by gastrointestinal surgery. However, in the same study, vascular, urology, and thoracic surgery were found to have comparatively low perforation rates [26]. In our study, plastic and neurosurgery procedures were found to have comparatively low rates of glove perforation, probably because most of the procedures in these subspecialties are often carried out quite meticulously.
Caillot et al. [29] and Harnoss et al. [30] have reported that visual detection of glove perforation is often not reliable. In our study, few gloves had gross evidence of perforation, whereas the majority were only detected microscopically. A study on the electronic evaluation of the value of double gloving by Caillot et al. [29] concluded that without the electronic detection, a large majority of glove perforation would remain undetected by the surgical team.
Jamal et al. [5] and Florman et al. [19] have established from their studies that double gloving is an effective method to reduce the surgeons' potential risk of contracting bodily fluids. In our study, double gloving (wearing two pairs of gloves) substantially reduced the perforation rate of the inner glove by more than 90%. Thus, this reduces the risk of contamination by bodily fluids to the barest minimum. This finding is similar and is supported by the one reported by Tanner et al. [10], where they found a substantial reduction of the rate of perforation of inner glove compared with single gloving.
To enhance comfort and sensitivity, which is the most common challenge experienced by double gloving, Osman and Jensen [2] and the CDC report of 2003 [8] have recommended a test of different options for double gloving in order to avoid hand-fatigue or other discomforts. Even though sizing of gloves depends on individual needs, when double gloving, Lain et al. [14] and Harnoss et al. [16] have reported and thus suggested three common practices that have been shown to be fairly acceptable and common among operating staff. For instance, with size 7.5 + 7.5 −, wearing two gloves with similar sizing, with size 7.5 + 8.0 −, the outermost glove is half a size larger, whereas with size 7.5 + 7.0 −, the outermost glove is half a size smaller.
Limitations
Other factors, such as open versus laparoscopy surgery and the use of electro-cautery devices in dissecting soft tissue and muscles, may have great influence on the rate of glove perforations. However, in our study population, laparoscopy surgery and the use of electro-cautery devices were optional and infrequent, so we could not consider these factors. Perhaps there is a need to consider these factors in subsequent and similar studies so as to lay bare or further elucidate all possible mechanisms and risks of glove perforations in surgery.
Conclusion
The use of double gloves has more than 90% protection to both the patient and the surgeon. Therefore, wearing double gloves during an operation is useful, particularly in the present generation where the manufacturer, having understood the value of double gloving in surgery, have started designing gloves that support not only double gloving, but also can reach the elbow region of a surgeon.
Footnotes
Author Disclosure Statement
No competing financial interests exist.