
Abstract
Abstract
Background:
The aim of this study was to investigate the effect of door opening rates on air quality in the operation room during hip revision surgery by measuring the number of colony forming units per cubic meter (CFU/m3).
Methods:
During 70 hip revision operations the number of CFU/m3 was measured at four time points. Factors that may influence air quality were recorded, including the number of persons present, duration of surgery, and door opening rates. The measured CFU/m3 was dichotomized as either acceptable (≤20 CFU/m3) or not acceptable (>20 CFU/m3). To determine whether door openings were associated with CFU/m3 values, we used generalized linear mixed models to model the dichotomized repeatedly measured CFU/m3 values.
Results:
The median number of door openings per operation was eight (range, 0–72), the median duration of surgery was 145 min (range, 60–285), and the median number of persons present during surgery was eight (range, 5–10). Adjusted for number of persons in the operation room and duration of surgery, the number of door openings per operation was associated (odds ratio [OR] 1.05 [95% confidence interval {CI} 1.02–1.09]; p = 0.003) with an unacceptable number of CFU/m3.
Conclusions:
In conclusion, a substantial association between number of door openings and an unacceptable number (>20) of CFU/m3 was found. Adjusted for number of persons in the operation room and duration of surgery, every door opening increased the odds of unacceptable CFU/m3 values by 5%. Number of persons present during surgery and duration of surgery were not related to CFU/m3.
T
Intra-operative bacterial contamination has been related to the occurrence of periprosthetic infection [5]. Intra-operative contamination of the incision may occur with the patient's skin flora or with the commensal flora of the operating room personnel through instruments and other materials [6]. In addition, studies have shown that most airborne bacteria reach the incision area via the hands of the surgical personnel or by the instruments used [7,8].
Several studies have investigated the presence of airborne bacteria in the operating room, factors that influence their numbers, and their role in intra-operative infection, all with different conclusions [5,9–13]. To minimize periprosthetic infection, it was proposed by the Hospital Infection Society Working Party on Infection Control in Operating Theatres (HISWPICOT) that during high-risk operations, such as orthopedic implant surgery, the number of colony forming units (CFUs) in the air should not exceed 10 CFU/m3 at 30 cm distance from the incision and not exceed 20 CFU/m3 directly around this zone [14]. In non-high–risk surgery, a maximum of 180 CFU/m3 is allowed. The recommendations of the HISWPICOT has also been adopted in The Netherlands, however, strict rules on maximum CFU or rules on discipline in the operating room are not available.
In this study we investigated the effect of door opening rates on air quality in the operation room during hip revision surgery by measuring the number of CFU/m3. It was hypothesized that minimizing the number of door openings would lead to reduced numbers of CFU during surgery.
Patients and Methods
Setting
This multi-center observational study evaluated air quality in the operating room during revision hip arthroplasties and was embedded in another study on bone grafts [15]. Between February 2009 and December 2011, a total of 70 revision hip operations with bone impaction grafting (BIG) were performed and included. The study was performed at the Departments of Orthopaedics at the Radboud University Medical Center in Nijmegen and the Reinier de Graaf Hospital in Delft, The Netherlands. In Nijmegen, 59 operations were monitored; the remaining 11 operations were in Delft. The study was approved by the local Medical Ethics Committees and written informed consent was obtained from all patients.
Both operating rooms were equipped with turbulent-flow ventilation systems with high-efficiency particulate air (HEPA) filters, which are 99.97% efficient in removing airborne particles of 0.3 mm or larger. In Nijmegen, the HEPA filters are replaced every 6 months and maintenance work on the system is carried out periodically. The operating room is under positive pressure in relation to the adjacent rooms (5 Pa); air temperature and humidity are set at 18°C and 56%–60%, respectively. In Delft, the HEPA filters are replaced every 12 months. The operating room is under positive pressure in relation to the adjacent rooms (15 Pa); air temperature is set at 18°C and humidity at 50%–65%. In Delft, exhaust body suits were used by the operating team.
Onsite observations
Factors that may influence the air quality were recorded, including date, time, operating room identification number, positioning of the air sampling filter (place and angle), air temperature, the number of persons present, the duration of surgery (minutes), and door opening rates (and when possible, reasons for doors being opened).
Air quality measurements
The number of CFU/m3 was measured four times during surgery: Directly after incision; directly after opening of the container of the allograft bone; at the time the allograft bone was first used in the procedure; and again 10 min later.
Two hundred liters of air with an airflow rate of 100 L/min was aspirated with the High Flow Microbial Airborne Sampler (RCS High Flow, Kregliner Europe, Antwerp, Belgium) containing an RCS strip with Tryptic Soy Agar (TSA, Kregliner Europe, Antwerp, Belgium). Patients were in the lateral position and the device was placed at a distance of approximately 1.5 m from the incision. During measurements, the orthopedic surgeon stepped aside, allowing the researcher to perform the measurements without anything between the device and the incision. The RCS High Flow Sampler was positioned horizontally at wound height and directed toward the wound.
The numbers of CFUs on the RCS strips were counted manually after 48 h of incubation at 30°C and converted to number of CFU/m3.
Follow-up
The medical files of all patients were reviewed, including clinical, radiologic, and laboratory findings, to assess the occurrence of an infection post-operatively.
Data analysis
Outliers in CFU/m3 were defined as values higher than the 95th percentile. These outliers were removed and considered as missing data. According to the proposal of the HISWPICOT, 20 CFU/m3 is the maximum acceptable number of CFUs during high-risk operations. Therefore, CFU/m3 was dichotomized as either acceptable (≤20 CFU/m3) or not acceptable (>20 CFU/m3). To determine whether door openings were associated with CFU/m3 values, we used generalized linear mixed models to model the dichotomized repeatedly measured CFU/m3 values. Using these models, the effects of covariates (door openings/operation, persons in the operation room/operation, and the duration of surgery) on the probability of occurrence of the event (i.e., >20 CFU/m3) can be studied effectively. We considered a given operation room's observations to be non-independent so we nested the surgeries within hospital. A random intercept for each hospital was fit in order to control for an individual hospital effect. Odds ratios for covariates without interactions were calculated as the exponential of the estimated coefficient for that parameter and confidence intervals were calculated using the standard errors of the coefficients.
All statistical analyses were performed using R version 2.1.3 (R Foundation, Vienna, Austria) with package lme4. p values <0.05 were considered statistically significant.
Results
One surgical procedure was excluded because the patient was intra-operatively resuscitated, resulting in severe violation of all sterility protocols. Therefore, 69 hip revision operations were analyzed. The results of the observations and measurements during the 69 hip revision operations are summarized in Table 1.
CFU/m3 = colony forming units per cubic meter.
The median number of door openings per operation was eight (range, 0–72), the median duration of surgery was 145 min (range, 60–285), and the median number of persons present during surgery was eight (range, 5–10). Figures 1, 2, and 3 represent plots of the duration of surgery against the median number of CFU/m3, the total number of people present in the operating room, and the total number of door openings, respectively.
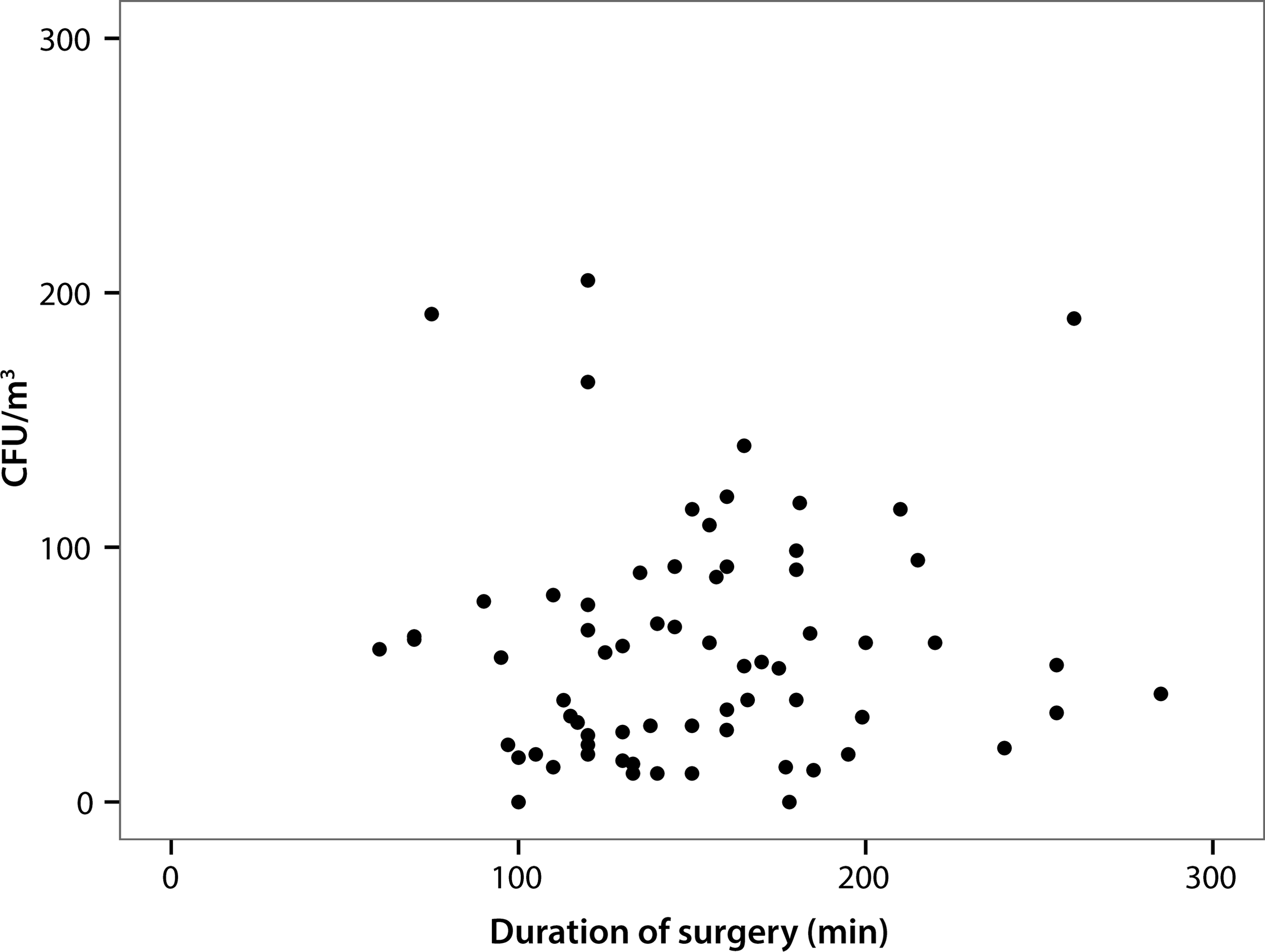
Duration of surgery versus median number of colony forming units per cubic meter (CFU/m3).

Duration of surgery versus total number of persons present during surgery.
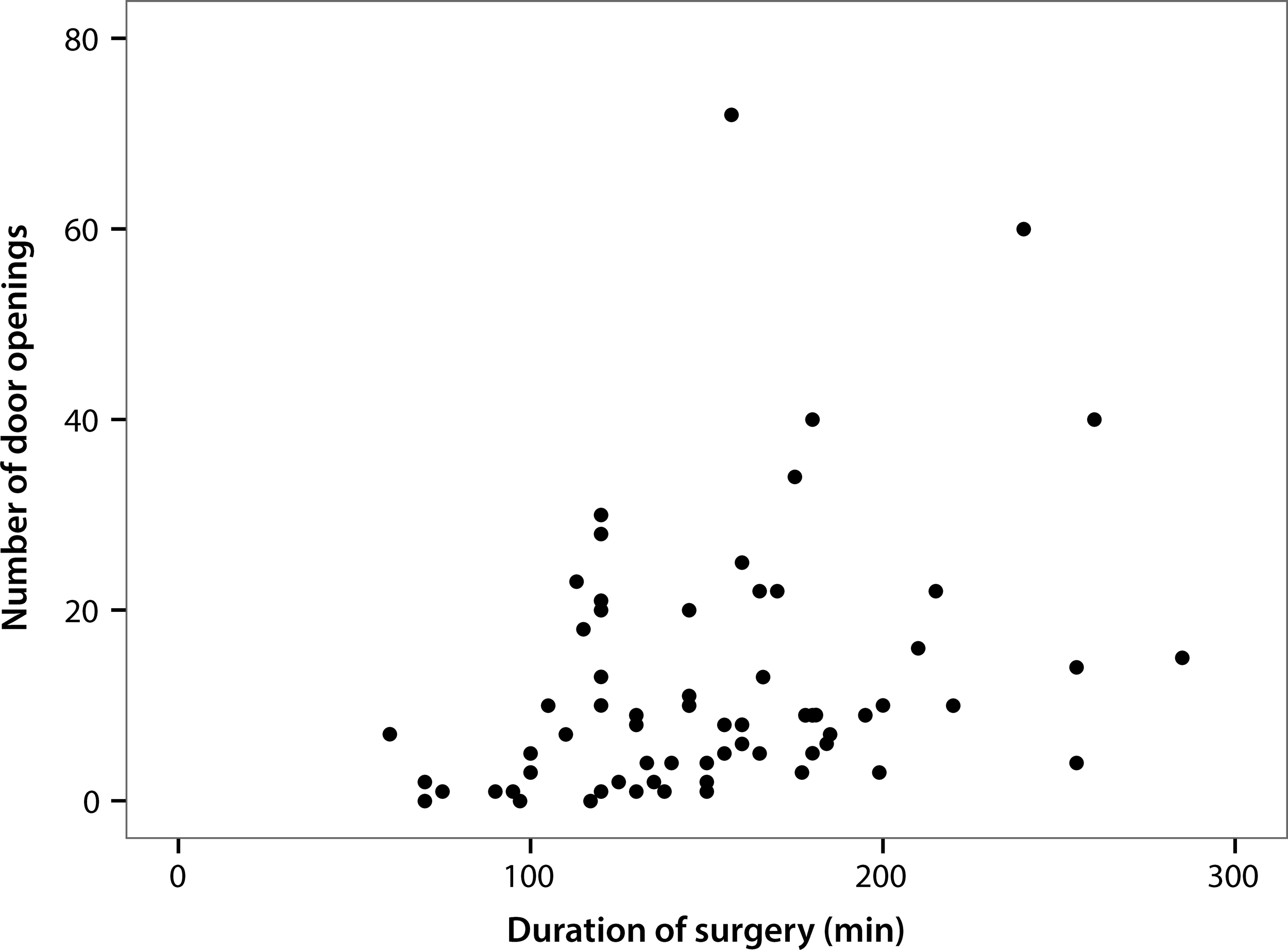
Duration of surgery versus total number of door openings.
There was a large range in the total number of CFU/m3 measured per individual surgery. Directly after incision, in 23 (35.4%) of 65 operations an acceptable number of ≤20 CFUs/m3 was measured. Directly after opening the container of the allograft bone, ≤20 CFUs/m3 were measured in 14 (22.2%) operations. At the time the bone graft was first used in the procedure and 10 min later, an acceptable number of CFU/m3 was measured in 17 (26.2%) and 19 (29.2%) of 65 operations, respectively.
Adjusting for number of persons in the operation room and duration of surgery, the number of door openings/operation was associated (OR 1.05 [95% CI 1.02–1.09]; p = 0.003) with the odds of >20 CFU/m3 (Table 2). The number of persons in the operating room per operation (OR 1.02 [95% CI 0.72–1.45); p = 0.9) and duration of surgery (OR 0.99 [95% CI 0.99–1.00]; p = 0.1) were not associated with the odds of an unacceptable number of CFU/m3.
OR = odds ratio; CI = confidence interval; CFU/m3 = colony forming units per cubic meter; NS = not significant.
Follow-up
Mean follow-up of all patients was 28 mo (±14.6), with a minimum follow-up of 13 mo. Mean age at operation was 67.4 y (standard deviation [SD] 10.9). Fifty-six percent of the patients were females. One patient developed an infection post-operatively (1.4%). This infection was caused by coagulase-negative staphylococci (CoNS) and Enterobacteriae. The numbers of CFU/m3 measured during this particular surgery were 5, 15, 10, and 15 for the four time points, respectively, and the number of door openings was four.
Discussion
In this study we measured the numbers of CFU/m3 during 69 hip revision arthroplasties in combination with BIG. It was hypothesized that a reduced frequency of door openings per operation leads to a reduced number of CFU during surgery. Our results show that adjusting for number of persons in the operation room and duration of surgery, every door opening increases the odds of an unacceptable CFU (> 20 CFU/m3) by 5%. This finding is in accordance with the results of Andersson et al. [16] who found that 34% of the variance in CFU/m3 was explained by traffic flow during surgery, however, their numbers of door openings per hour were much greater. Several studies suggested a relation between traffic flow and the risk of infection [17–19], however, other studies reported no significant association between door openings and the number of CFU/m3 [13,20].
In our study, a median number of eight door openings per operation were observed during the revision operations. In both hospitals doors were allowed to be opened only if strictly necessary. The number of door openings is low compared with other studies [16–19,21,22].
The HISWPICOT proposed a maximum of 20 CFU/m3 at a distance of more than 30 cm of the incision during implant surgery. When this criterion of ≤20 CFU/m3 was taken as reference, six (8.7%) of 69 operations met this criterion during all four measurements. Air quality measurements performed by Andersson et al. [16] and by Stocks et al. [13] during joint arthroplasties also exceeded the recommended concentration of ≤10 CFUs/m3, although their mean values were lower compared with our results. As stated by Dharan and Pittet [23], it is not easy to achieve these limits because various factors influence the bio-burden during a surgical procedure. In contrast, Ahl et al. [24] did find mean results that did not exceed the proposed limits. They even stated that when wearing body exhaust clothes, it is possible to achieve numbers <1 CFU/m3.
Ritter [25] suggested reducing the number of people present during the operation and reducing the operating time to decrease the number of bacteria in the air. This was supported by Ong et al. [26] who also concluded that procedure duration is a substantial risk factor for infection. However, we did not find a relation between the numbers of CFUs/m3 and the duration of surgery or number of persons present in the operating room. The number of persons present during the hip revision operations in our study was consistently relatively high because both hospitals are teaching hospitals. This might explain the absence of a relation between number of persons present and the numbers of CFU/m3. Andersson et al. [16] stated that the duration of the operation in relation to the total CFU concentration is of clinical relevance, because the total CFU concentration increases with increasing duration of surgery, thereby exposing the incision to an increased total number of CFU and increasing the risk of infection.
One patient developed an infection in our study. Remarkably, the number of door openings during this procedure and the number of CFU/m3 were low. A potential limitation of our study is that we only measured the total numbers of door openings and people present in the operating room throughout the operation and did not perform these measurements at each of the four time points. This prevented us from analyzing the association between door openings and numbers of CFU/m3 in more detail.
Conclusion
A significant association between the number of door openings and an unacceptable number (>20) of CFU/m3 was found. Adjusted for number of persons in the operation room and duration of surgery, every door opening increased the odds of unacceptable CFU/m3 values by 5%. The proposed maximum of ≤20 CFU/m3 during high-risk operations by the HISWPICOT was often exceeded in this study, although only one patient developed an infection post-operatively. The number of persons present during surgery and the duration of surgery were not related to CFU/m3.
Footnotes
Acknowledgments
This study was funded by Bislife, The Netherlands.
Author Disclosure Statement
N.M.C.M. and R.M.B. are employees of Bislife, The Netherlands.