
Abstract
Abstract
Background:
Pyomyositis (PY) is a primary infection of the skeletal muscles, leading to inflammation of the muscle fibers followed by pus formation and even necrosis in late stages. Because of overlap in presentation of intermuscular abscess (IM) and PY, the exact incidence and severity of PY is under-appreciated.
Patients and Methods:
We conducted a prospective analytical study in a tertiary care center in North India from October 2011 to January 2013, recruiting patients with abscesses involving the chest wall, abdomen (parietal wall including back), and extremities. Subcutaneous, hepatic, intra-abdominal abscess, and secondary abscesses were excluded. Primary PY was defined as a primary infection of skeletal muscle without any foci from adjacent skin, soft tissue, or bone. Clinical, radiologic, pathologic, and operative findings suggested diagnosis; loss of striations and lymphocytic infiltration in the muscle fibers was confirmatory. The chief outcome variables were death and length of hospital stay.
Results:
Thirty patients with a mean age of 29.5 y (IM: 29.7 ± 16.7, PY: 25.28 ± 17.6) were classified as IM (18/30, 60%) or PY (12/30, 40%). Most PY occurred in the lower limb (41.7% had multi-site involvement); most had a history of trauma or immunocompromised state. Fever, tachycardia, tachypnea, hypotension, pallor, and hyperesthesia were significantly higher (p < 0.05) in PY. Mean Sequential Organ Failure Assessment (SOFA) score was 0.33 for IM, 2.5 for PY. Staphylococcus aureus was predominant in both groups; however, all four patients with methicillin-resistant S. aureus (MRSA) were in the PY group. Both deaths also occurred in the PY group. The mean duration of hospital stay was 3.22 ± 1.11 d for IM and 10.27 ± 2.32 d for PY patients (p = 0.03).
Conclusion:
PY is a specific and potentially fatal infection, which is common in our country and must be differentiated from IM. A high index of suspicion and early institution of specific antibiotics followed by operation is therapeutic.
P
Data from case series of PY are mostly available from temperate countries, where the microbiologic and clinical aspects differ from what we observe in our daily practice. We conducted a study of 30 patients who presented with overlapping features of IM and PY and studied the clinical presentation, biochemical, and hematologic parameters, antibiotic profile, and the outcome in terms of death and recovery. An attempt was made to objectively differentiate PY from other abscesses.
Patients and Methods
This prospective analytical study was conducted in the department of surgery of a tertiary care teaching hospital in North India from October 2011 to January 2013. Patients with a clinical diagnosis of abscess involving the chest wall, abdomen (parietal wall including back), and extremities were included in the study. Subcutaneous, hepatic, intra-abdominal abscess, and abscess secondary to underlying pathology such as osteomyelitis or septic arthritis were excluded. For the purpose of the study, primary PY was defined as a primary infection of skeletal muscle without any foci from adjacent skin, soft tissue, or bone. Clinical, radiologic, pathologic, and operative findings were used to support the diagnosis [3,7]. An IM was defined as a cavitary collection of pus between skeletal muscles [8,9]. The final differentiation was based on the involvement of muscle fibers on histopathologic examination in the form of loss of striations and lymphocytic infiltration (Fig. 1).
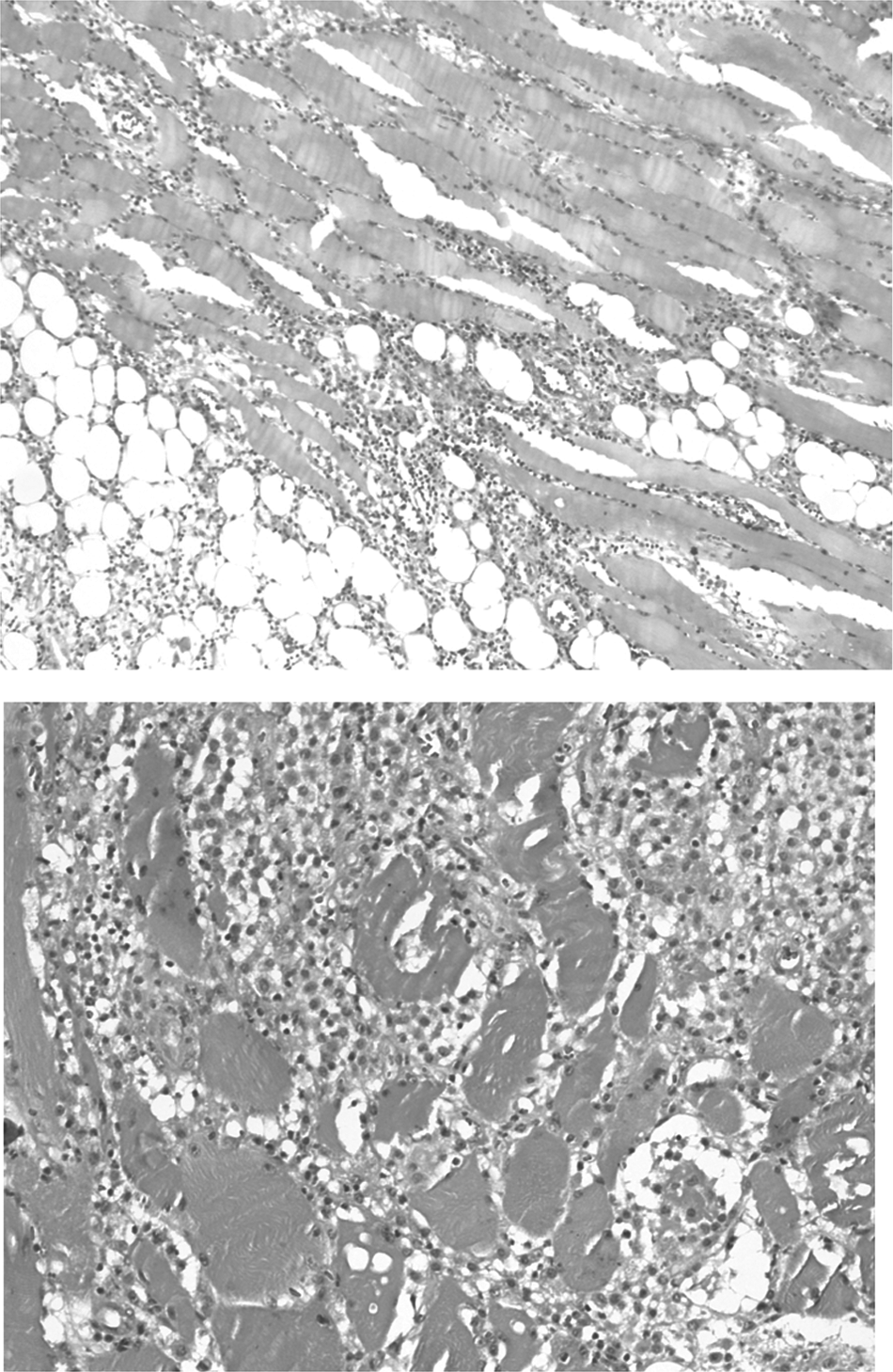
Muscle tissue from patients with pyomyositis has been stained with hematoxylin and eosin and are seen 10x (left) and 40x (right). Note the loss of striations and dense infiltration of lymphocytes.
After admission, patient characteristics including age, gender, duration of symptoms, social background, co-morbidities, risk factors, history of intravenous drug abuse, symptoms and signs at presentation were recorded. The following hematologic and biochemical parameters were also recorded: Hemoglobin and blood cell counts, pH, serum sodium and potassium, blood urea, serum bilirubin, serum levels of liver enzymes, serum creatinine, and C-reactive protein (CRP) levels. Sequential Organ Failure Assessment (SOFA) score was used to assess the severity of infection at presentation [10,11].
All patients were administered intravenous amoxicillin-clavulanic acid empirically; antibiotics were modified after obtaining culture reports. Ultrasonography with high-frequency probes was used to identify the plane of abscess. All patients were taken to the operating room (incision and drainage with or without fasciotomy); timing of operation, location of pus, involvement of muscle (intra- or intermuscular) was noted. Muscle biopsy was performed in all cases, with repeat debridement when necessary. The chief outcome variables were death and length of hospital stay.
Statistical analysis
The clinical and biochemical factors of both groups were compared. Keeping level of significance at 95%, chi-square/Fisher exact test was used for qualitative factors, and unpaired Student t-test for quantitative factors.
Results
Demographics, risk factors, and clinical characteristics
Thirty patients who fulfilled the inclusion criteria were classified as IM (18/30, 60%) or PY (12/30, 40%) based on the involvement of muscle fibers on histologic evaluation. The demographic profile is shown in Table 1.
Bold indicates values that are statistically significant.
Overall, the mean age at presentation was 29.5 y (IM: 29.7 ± 16.7; PY: 25.28 ± 17.6). Despite there being no significant difference in the mean age at presentation, 50% of patients with PY were below 20 y. There was no significant difference in the male:female ratio. Intermuscular abscess occurred all over the body without any predilection for a particular region, whereas most cases of PY occurred in the lower limb and 41.7% cases had multiple site involvement (Fig. 2). It can be observed in the risk factors that most patients with PY had a history of trauma or immunocompromised state (diabetes mellitus, chronic organ failure, intravenous drug abuse).

Typical clinical features of pyomyositis: Top left, calf tenderness and scant signs of inflammation in a 14-year-old boy; top right, subsequently, a scapular abscess, pathognomic for pyomyositis, developed in the same patient; bottom left, a 34-year-old male with thigh swelling and tenderness (no fluctuation and minimum redness, who underwent fasciotomy, bottom right. Pus was present between the muscle fibers; there was minimum cavitation.
Pain, swelling, and erythema occurred in both groups while fever, tachycardia, tachypnea, hypotension, pallor and hyperesthesia were significantly higher (p < 0.05) among those in the PY group. Restriction of movement and fluctuation were present in both the groups without any significant differences.
Laboratory parameters and microbiologic aspects
Elevated CRP, blood urea, serum creatinine, leukocyte counts, and serum bilirubin were found to be significantly associated (p < 0.05) with the PY group (Table 2). Mean SOFA score at presentation was 0.33 for IM as opposed to 2.5 for those in the PY group. Staphylococcus aureus was the predominant organism in both groups; however, all four cases of methicillin-resistant S. aureus (MRSA) were isolated from the PY group. In the IM group, 15/18 cases were monomicrobial isolates.
SD = standard deviation; CRP = C-reactive protein.
Bold indicates values that are statistically significant.
Treatment and outcome
Ultrasonography was used to identify the plane of the abscess. We were able to diagnose five cases of PY based on the ultrasonographic findings. In six patients with PY, the empiric therapy with intravenous amoxicillin-clavulanic acid was changed to a culture-specific antibiotic because of the presence of gram negative infection or MRSA. All 30 patients underwent a surgical procedure. The mean number of repeat debridements for IM was 0.32, while for PY, it was 1.09. Both deaths also occurred in the PY group. The mean duration of hospital stay was 3.22 ± 1.11 d for IM and 10.27 ± 2.32 d for PY (p = 0.03).
Discussion
The differentiation of PY from IM can be difficult because of a similar clinical profile. The differentiation of PY from other soft tissue infections has been attempted in a few studies; however, these have been largely in temperate countries [2,3,7] In these areas, PY commonly presents at the inflammatory stage or stage 1, where it can mimic other types of myositis or neuralgia because pain is the main symptom. Complications such as multiorgan failure and tissue necrosis are seldom reported in cases from Western countries.
None of our patients presented in the myositis stage. In the abscess stage, in fact, it may be clinically indistinguishable from an IM. Some differentiation has been possible using ultrasonography and MRI and tissue biopsy [12,13]; however, clinical differentiation is still a challenge for the treating clinician. Early recognition of PY is important for effective, targeted antibiotic therapy and planned surgical management.
Clinical presentation
PY affects young individuals, mostly less than 20 years of age, and rarely over 60; this is evident in our data. The predilection of PY for a younger age group has been described by most authors. Bickels et al [1] reported the highest incidence in the first two decades of life in a large series of 676 patients with PY studied from 1960 to 2002.1 It has been postulated that sub-clinical trauma in young active persons may form a nidus for infection [2,14–16].
The involvement of multiple simultaneous muscles is pathognomic of PY; frequently involved muscles are long extensors such as quadriceps, glutei, pectoralis major, serratus anterior, biceps, iliopsoas, gastrocnemius, abdominal and spinal muscles [17–20]. Sequential or simultaneous involvement may be observed in 12%–40% of patients [21–24]. This could be partly explained by increased mobility of the limb girdle with an increased risk of trauma. In our study, the limb girdle was affected in 50% of patients. There was complete correlation between multiple site involvement and other diagnostic features.
Another indirect pointer toward the etiopathogenesis in our cases was the obvious breach of skin (insect bite, intra-muscular injection, and foreign body splinter) observed in nine cases of IM, whereas there was no breach in the PY group. Evidence of sub-clinical trauma (fall, strenuous exercise) was observed in 41.7% of patients. In the literature, the incidence of trauma as a risk factor for PY varies from 12%–42% [7,25,26]. As expected, a muscular abscess usually has a breach in the skin or an inciting event [27–29]. All our patients had negative test results for human immunodeficiency virus serology; why does a particularly virulent form of Staphylococcus afflict bruised muscles in these otherwise healthy persons?
As mentioned earlier, PY occurs in three phases; the initial phase or invasive stage has only tenderness over the affected area and no systemic symptoms. Erythema is conspicuously absent because of the deep-seated infection. This phase may resolve spontaneously, mimicking fibromyalgia, or might progress to a suppurative stage. None of our patients presented in this stage.
In the suppurative stage, patients present with fever, tachycardia, tachypnea, restriction of movement, and other systemic features [3]. Most patients, especially in tropical countries, present in the suppurative stage [30]. Sharma et al. [7] in their study of 67 patients with PY found fever, painful muscle swelling, and back pain to be the most common symptoms, concluding that 90% of patients presented in the suppurative stage. All but two of our patients with PY presented with suppuration. The classic sign of abscess—fluctuation—may not be appreciable because the overlying muscle is tense [3,30]. The final stage of PY is disseminated infection leading to septic shock and metastatic infection. In our study, two patients presented in this fulminant stage. Fulminant sepsis also differentiates PY from ordinary abscesses.
Biochemical and hematologic characters
An elevated total leukocyte count (TLC), blood urea, CRP, and high SOFA score at presentation point toward PY rather than abscess.8 CRP was elevated in 81% of our PY patients. Four patients with PY had a SOFA score >4 at presentation; two died. In an asymptomatic patient with muscle pain and no other features of infection (fever, chills, erythema) but having leukocytosis and raised erythrocyte sedimentation rate, PY should be suspected [2,3,7,30,31]. Muscle enzymes might be normal or slightly elevated; they have been shown to have low sensitivity and specificity [32,33]. A muscle enzyme test (creatine phosphokinase) may be useful in earlier stages to distinguish the deep-seated pain from other causes such as osteomyelitis or other soft tissue inflammation. It is not specific and less useful in later stages, however.
Microbiologic aspects
The most common organism isolated in both the groups was S. aureus. There were four MRSA isolates from the PY group and none from the abscess group. This association of S. aureus with PY has been reported by many authors, although the presence of MRSA is not common [1,3,7,34,35]. The virulence factor and strain that cause the severe infection seen in PY needs to be evaluated (vide infra). The PY in tropical areas is overwhelmingly from gram positive bacteria—mostly S. aureus, sometimes, Streptococcus pyogenes. In temperate areas, other bacteria such as Neisseria, Enterococcus, and Escherichia coli have been reported [2,16].
Radiologic aspects
Ultrasonography is noninvasive and useful during the purulent stage of PY when it may detect diffuse muscle hyperechogenicity with or without localized hypoechogenicity and diffuse hyperemia [13,36–38]. Although ultrasonography can differentiate between IM and PY, the sensitivity is low [13]. Computed tomography (CT) and magnetic resonance imaging (MRI) are the best imaging techniques for early diagnosis [39–41]. CT may reveal segments of low attenuation with loss of muscle planes and a surrounding rim of contrast enhancement as characteristic of PY. An MRI is considered the gold standard for the diagnosis of PY at all stages of infection. The MRI shows hyperintense rim on T1-weighted images with peripheral enhancement on a gadolinium diethylenetriaminepentaacetic acid scan [12,42]. Similarly, MRI may be used in differentiating PY from necrotizing soft tissue infection [12].
Treatment and outcome
The modalities of treatment are life support, antibiotics, and surgical drainage/ debridement. Three clinical stages of the disease have been noted: The initial subtle muscle inflammation, suppuration, and, finally, muscle necrosis and organ failure. The treatment would depend on the stage at presentation. With more recognition and suspicion, the earlier stages can be identified with cross-sectional imaging such as CT or MRI. Hence, the clinical presentation can overlap with necrotizing infections, which is common in our country.
The common pathogens have been listed earlier. It thus follows that broad-spectrum antibiotics with known sensitivity to locally isolated MRSA are used empirically, with de-escalation after culture reports. In our scenario, we use co-amoxyclav, linezolid, clindamycin, piperacillin-tazobactam, vancomycin, and imepenems. Evacuation of pus and debridement of necrosed muscle should be performed aggressively [3,8,43,44]. Muscle biopsy, although not performed universally, may indicate specific features of PY such as inflammatory infiltrates in muscle, muscle fiber necrosis surrounded by neutrophils, and mononuclear inflammatory cells with gram positive cocci [45].
The associated sepsis and organ failure was measured in terms of SOFA score [10,11]. Organ failure did not develop in any of our patients with IM, while four patients with PY had a SOFA score >4 with two deaths. The mortality rate has varied between 10% and 23% [2,7,23,25,26].
In our country, especially in the warmer season, we believe that affliction with PY is high; in our clinical experience, it constitutes up to 25% of all admitted hospital patients with skin and soft tissue infections (SSTIs). No published data are available yet for this association, although we have studied these patients for 5–6 y and are in the process of publishing our data. Although virulent subtypes of S. aureus (with toxins such as Panton-Valentine leukocidin) have been shown to cause other severe infections such as necrotizing pneumonia [46], we have limited data for this association with severe SSTIs [47]. The fact that the muscle biopsies of some of the advanced cases also showed specific changes may be indirect evidence of progression of the various stages of PY.
We hypothesize that PY may also be caused by specific virulent toxins capable of afflicting healthy young persons; however, we need to isolate this from a large number of cases, preferably as an epidemiologic collection in the field setting. The need for this differentiation is clearly obvious, because the therapeutic window is narrow. There are more fatal outcomes with PY than IM; with awareness and early clinical suspicion, it can be diagnosed at the inflammatory stage and patients treated with specific antibiotics such as linelozid or vancomycin, thereby reducing death. Knowing that the pus is intramuscular and likely to affect multiple long extensors during the same admission helps the surgeon plan effective operative treatment.
Limitations of the study
It is well expected that time to presentation, time to initial debridement, and local care of the wound are expected to affect outcome (death, limb loss, and hospital stay). In this article, however, our objective is not to randomize two groups to compare two treatment modalities; neither is it to analyze the factors affecting outcome. This is intended to be an observational comparative study to bring out recognition and awareness about this entity and provoke further thought into analysis of outcome. Moreover, with two deaths, the study is not adequately powered to enable determination of factors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.