
Abstract
Abstract
Background:
Interventions to contain two multi-drug-resistant Acinetobacter (MDRA) outbreaks reduced the incidence of multi-drug-resistant (MDR) organisms, specifically methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus, and Clostridium difficile in the general surgery intensive care unit (ICU) of our hospital. We therefore conducted a cost-effective analysis of a proactive model infection-control program to reduce transmission of MDR organisms based on the practices used to control the MDRA outbreak.
Methods:
We created a model of a proactive infection control program based on the 2011 MDRA outbreak response. We built a decision analysis model and performed univariable and probabilistic sensitivity analyses to evaluate the cost-effectiveness of the proposed program compared with standard infection control practices to reduce transmission of these MDR organisms.
Results:
The cost of a proactive infection control program would be $68,509 per year. The incremental cost-effectiveness ratio (ICER) was calculated to be $3,804 per aversion of transmission of MDR organisms in a one-year period compared with standard infection control. On the basis of probabilistic sensitivity analysis, a willingness-to-pay (WTP) threshold of $14,000 per transmission averted would have a 42% probability of being cost-effective, rising to 100% at $22,000 per transmission averted.
Conclusions:
This analysis gives an estimated ICER for implementing a proactive program to prevent transmission of MDR organisms in the general surgery ICU. To better understand the causal relations between the critical steps in the program and the rate reductions, a randomized study of a package of interventions to prevent healthcare-associated infections should be considered.
I
Two multi-drug-resistant (MDR) Acinetobacter (MDRA) outbreaks occurred at our institution, in 2004 and in 2011. Both were immediately addressed with aggressive, multi-disciplinary infection control initiatives, which included enhancing hand hygiene, closuring of medical units for deep cleaning, cohorting of infected patients, increasing the nurse to patient ratio to 1:1, and replacing all disposable supplies. The 2011 MDRA outbreak response cost the hospital approximately $371,079, not including its potential impact on personnel, reputational, or legal concerns [7].
When we analyzed these two MDRA outbreaks for quality improvement reasons, we found that in the general surgery ICU, the outbreak response was secondarily associated with a significant decrease in incidence rates of MDR organisms (methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus (VRE), and C. difficile) even though the main goal was to target the MDRA outbreak [7,8]. Incidence rates of these MDR organisms decreased by 48%–54% after the MDRA outbreak response compared with the six months before. However, the risk reduction did not persist beyond six months, suggesting that although outbreak responses can be effective in decontaminating the unit, they may need to be repeated periodically to have a sustained impact on pathogen transmission [8].
We thus aimed to determine whether a model of a proactive infection control program, designed on the basis of the MDRA outbreak response, would be cost effective in decreasing transmission of MDR organisms in the general surgery ICU compared with the current standard, which involves enhanced hand hygiene and other infection control measures and periodic environmental decontamination in response to sporadic outbreaks.
Materials and Methods
Partners Healthcare Institutional Review Board approval was obtained prior to the conduct of this project.
The 2011 MDRA outbreak occurred over nine weeks in a 793-bed acute-care hospital with a 10-bed general surgery ICU run by a multi-disciplinary team of surgeons, anesthesiologists, pulmonary critical care physicians, and emergency critical care physicians. The response occurred over a six-wk period in June–July 2011; details have been published previously [7,8]. Outbreak response measures included closing of the trauma and general surgery ICUs and transferring all of the ICU patients to an entirely different floor, which normally acts as a surge pod for the emergency department; providing specific care for MDRA patients, including contact isolation, cohorting, and 1:1 nursing care; testing and disinfecting all permanent equipment and environmental surfaces that may have come into contact with patients; replacement of all disposable supplies; and redoing the top layer of the floors of the closed ICUs and the surge pod.
We separated the excess cost of the 2011 MDRA outbreak response in the general surgery ICU from our previous analysis of the entire outbreak response [7]. We defined our clinical endpoints as the incident rate of MDR organism transmissions, which could be either infection or colonization. Our previous analysis showed that the median incident rate of infection with an MDR organism decreased after the 2011 MDRA outbreak from 7.7 cases per 1,000 patient days over six months before the outbreak to 4.0 per 1,000 patient-days over the six months after the outbreak (mean ± standard deviation 6.7 ± 4.0 and 2.7 ± 2.1, respectively), corresponding to a reduction in the absolute number of incident cases from ten to four [8]. We used these changes in absolute incidence and incidence rates as effectiveness measures for this analysis.
A model of a proactive infection control program for the general surgery ICU would feature a bundle of the key interventions from the 2011 MDRA outbreak response, including moving patients to a surge pod, deep-cleaning the ICU, moving patients back and cleaning the surge pod, as well as enhanced hand hygiene, an increased nurse-to-patient ratio, and replacement of all disposable supplies. The excess staffing (nursing, assistants, respiratory therapists, cleaning crew) required to perform this outbreak intervention was used to build the projected staffing for this model. The model program would take five days instead of the 6 wks needed for the 2011 outbreak response, because its aim would not be to control an outbreak but to augment routine cleaning programs. The model program would have substantially lower staffing, supply, and administrative costs than the 2011 outbreak response because it would take less time to implement (5 d vs. 6 wks, or roughly one-sixth as much time). The cleaning and costs of using a surge pod area would remain the same as during an outbreak response, because the same locations would need to be cleaned in this model program. The majority of the reduction in costs would be from the lower staffing needed for conducting the model program compared with the costs of the additional staff needed to respond to a six-wk MDRA outbreak. The program would have to be implemented at least twice a year to have a sustained impact on rates of MDR organisms, because the effectiveness of the 2004 and 2011 MDRA outbreak responses on the incidence of MDR organisms waned after six months [8].
TreeAge Pro (TreeAge Software Inc., Williamstown, MA) was used to develop a decision analytic model of an MDRA outbreak response with and without the model infection control program. The number of new cases of MDR organisms appearing in the six months before the 2011 MDRA outbreak was considered the baseline. Discounting was not deemed necessary in this analysis, as both the costs and the health effects were 2011 data. Incremental cost-effectiveness ratios (ICERs) were calculated, comparing the costs and the resultant health effects of the proactive model infection control program with current standard practices in the general surgery ICU. The base case uses the average cost estimates for each item, and incident cases of MDR organisms in the six months before and after the 2011 MDRA outbreak response to determine the ICER. We used the reduction in absolute case numbers to demonstrate the “cost per transmission averted,” and the incident rate reduction was applied to demonstrate the “cost per 1-point reduction in incident rate” as a potentially useful metric for policy makers. The ICER was calculated as:
To test the robustness of the results and explore the impact of uncertainties in cost data, univariable sensitivity analyses were performed to determine ICERs, and a probabilistic sensitivity analysis using 1000 Monte Carlo simulations was employed to create a cost-effectiveness acceptability curve. Monte Carlo simulation is a method that simulates the probability of all the possible outcomes by taking into account the uncertainty around multiple variables. The cost-effectiveness acceptability curve compares model and standard infection control strategies and presents the probability of one of the two strategies being more cost-effective than the other when different threshold values are applied for cost per transmission averted for every 1,000 patient-days. Willingness to pay thresholds was calculated to give hospitals a sense of whether a particular ICER justifies the resources required to perform the intervention.
The following parameters were varied: Costs of additional nursing hours, costs of deep cleaning, supplies, and costs of administrative time. We assumed that the four cost items followed a uniform distribution and derived ranges for each of the variables by using our model as the minimum and the costs of each variable from the 2011 outbreak response as the maximum. The cleaning costs were varied by 25% around the base case, as no other range exists.
Results
The overall excess cost borne by the hospital for the 2011 MDRA outbreak response in the general surgery ICU alone was estimated to be $160,041 (Table 1). The largest contributors to the costs were related to the extra nursing staff needed for the response (60% of total outbreak costs). Replacing supplies and equipment cost $16,428 (10%). Administrative time spent on the outbreak response cost $20,198 (13%). Effectiveness estimates are an absolute reduction in incidence by six cases or a rate reduction of 3.7 cases per 1,000 patient-days per six-mo period [8].
The costs of the model infection control program are estimated to be $34,254, with the largest component being staffing (47%) (Table 2). The program would have an annual cost of $68,509 and would be expected to result in an absolute reduction in cases of resistant pathogens by 12 or a rate reduction of 7.4 cases per 1,000 patient-days annually. The two recent MDRA outbreaks were seven years apart, and the current standard practice involves an outbreak response at a cost of $160,041 or an annual cost of $22,863 averaged across the intervening seven years.
The ICER of the base case—implementing the model infection control program twice a year compared with the existing standard infection control program with an outbreak response every seven years—is $3,804 per transmission averted per year, or $6,168 for reducing the incident rate by one point per year (Table 3; Fig. 1). Sensitivity analysis, taking into account uncertainty in cost for the four largest cost parameters, revealed ICER ranges of $3,708 and $7,682 per transmission averted. The cost-effectiveness acceptability curve comparing model and standard infection control strategies is given in Figure 2. On the basis of probabilistic sensitivity analysis, a willingness-to-pay (WTP) threshold of $14,000 per transmission averted would have a 42% probability of being cost-effective, rising to 100% at $22,000 per transmission averted.

Decision tree model. Whether pre-emptive and proactive programs are cost-effective compared with standard infection control, considering only their observed impact on multidrug resistant organisms. Cost and effect variables right to the terminal nodes denote payoffs of the model: cost of proactive programs versus cost of standard infection control program, and the effectiveness of preventing transmission of multidrug resistant organisms.
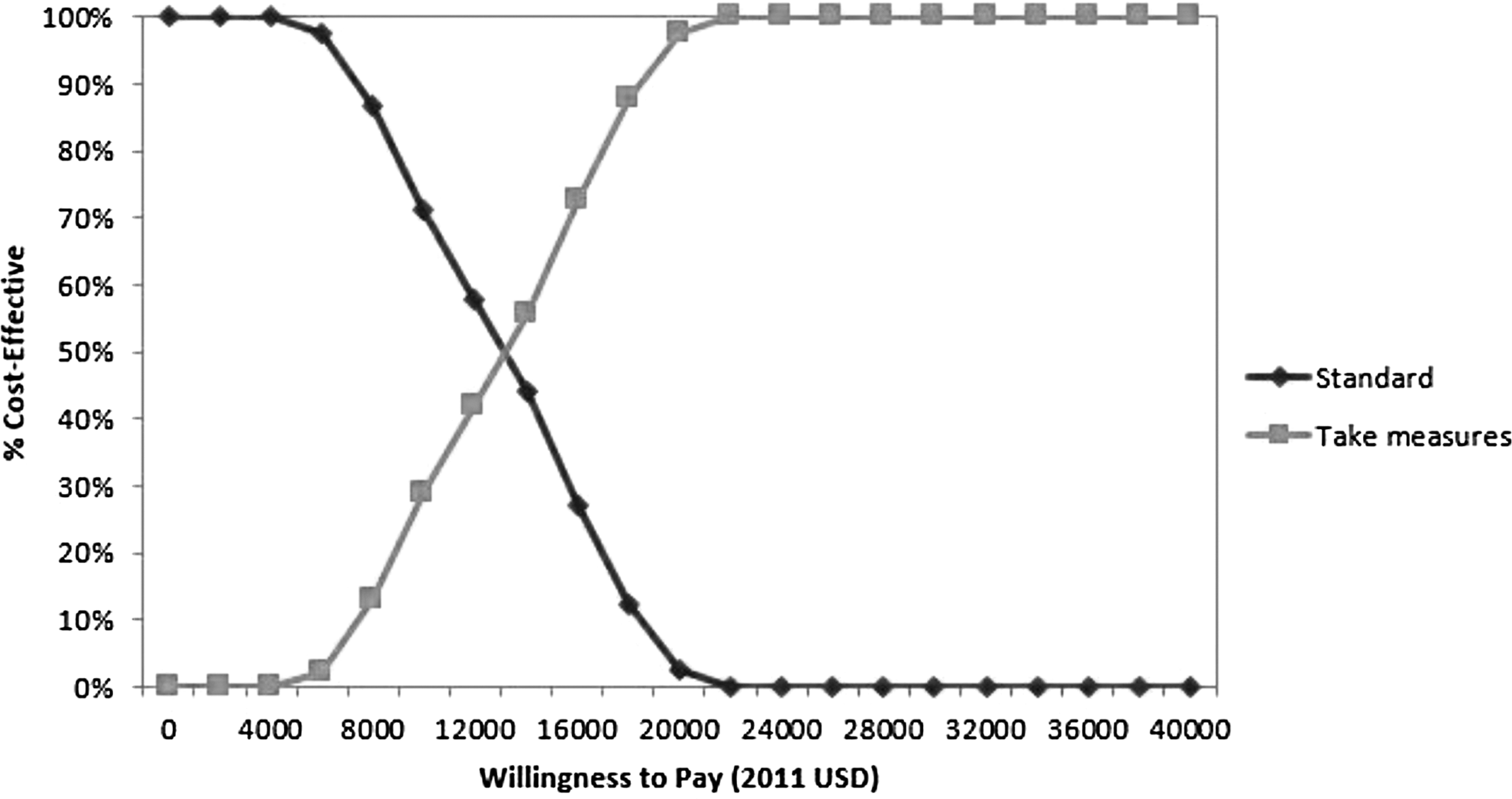
The probability of being cost-effective at different willingness-to-pay thresholds. The vertical axis represents the probability of one strategy being cost-effective. The horizontal axis represents the willingness-to-pay (WTP) thresholds (cost in 2011 US dollars per transmission averted in a 6-month period).
Response costs for multi-drug-resistant Acinetobacter outbreak in general surgery intensive care unit.
Estimated in Table 2, per y costs.
Differences in costs per y divided by twice the change in incident cases.
Differences in costs per y divided by twice the change in incident rates.
ICER = incremental cost-effectiveness ratio.
Discussion
Hospital-acquired infections are an expensive problem [1,2], and MDRA outbreaks are especially costly in terms of both human and financial impact [9–11]. The response to the 2011 MDRA outbreak in the general surgery and trauma ICUs at our hospital cost $371,079 [7].
There has been increasing recognition of the role of the environment in infection transmission [12,13]. Enhanced cleaning methods and isolation can limit outbreaks [9,10,14–16]. Aggressive multi-pronged techniques using environmental cleaning in combination with aggressive culture change [17,18], strict hand hygiene, and other measures can reduce the rate of infections [19–27].
In this study, we estimated the value of implementing a semi-annual model infection control program to prevent the transmission of MDR organisms in a general surgical ICU compared with current standard infection control measures, with aggressive periodic responses to outbreaks. Our model program was based on the key components of an MDRA outbreak response that reduced transmission of MDR organisms and included shutting down and deep-cleaning the ICU, cohorting infected patients, increasing the nurse-to-patient ratio to 1:1, and renewing all disposable supplies.
If this model program were implemented on a twice-yearly basis in the general surgery ICU, it would cost $68,509 per year (2011 U.S.$) or $3,804 per transmission averted per year, assuming consistent costs of staffing, supplies, and number of transmissions averted. Because hospital-acquired infections have been estimated to have attributable costs of $25,694–$32,388 (2011 U.S.$), spending $3,804 to avert even one additional MDR organism transmission per year in order to reduce the rate of infection may have a substantial clinical and financial impact for the hospital, especially as federal pressure not to reimburse for hospital-acquired infections increases [2]. Taking into account the uncertainty around the cost data, the model program starts to become more cost-effective than standard infection control measures if the hospital is willing to spend more than $14,000 to avert a single infection transmission. Alternatively, current standard infection control procedures would result in hospital costs of $160,041 every seven years of treating MDRA cases, a substantial impact on staff morale, damage to the reputation in the community, and potential legal repercussions after an outbreak, as well as incurring the additional costs of transmitting MDR organisms between MDRA outbreaks. Our study may be a useful model for hospitals as they plan to mitigate the impact of MDR organisms as well as to control intermittent outbreaks of MDRA.
Nevertheless, there are many limitations to our analysis. The limitations of the cost and effectiveness data have been discussed previously [7,8]. The estimated impact of the MDRA control efforts on transmission rates of MDR organisms is based on experience from a single institution, albeit from two MDRA outbreaks [7,8]. It also could not be subjected to rigorous sensitivity analyses because of the limitations of the effectiveness data. Additionally, the reduction in the number of cases of resistant pathogens is likely to be tied to the profile and number of patients at the institution, as well as the baseline rate of resistant pathogens in the unit. We did not perform sensitivity analyses of the variance in the baseline incidence rates, and hospitals that have lower baseline rates than in our experience may find this model to be less cost-effective, whereas hospitals with greater baseline rates may find this program much more cost-effective than we describe. Therefore, this experience may not be reproducible or generalizable, although measuring the baseline incidence of resistant pathogens and comparing it with our experience would be a valuable task for hospitals. Furthermore, we did not discriminate between infection and colonization. Thus, a point reduction in incident cases does not correlate directly with a reduced number of infections. All the costs were calculated retrospectively and do not allow calculation of the impact of ICU bed limitations on operating room productivity or emergency department throughput. The secondary implications of having to close down ICUs during an outbreak were not tracked formally at our institution and certainly should be assessed prospectively by hospitals when dealing with outbreaks. Therefore, our cost data represent the minimum financial burden of dealing with an outbreak and are subject to variability across institutions, especially as patient volumes differ. However, this framework could at least suggest how costs could apply across healthcare facilities.
Efforts still are needed to identify the most critical steps in the outbreak response and to determine if each of these steps is cost-effective to conduct individually or as a package. We estimated the cost-effectiveness based on changes in transmission rates of MDR organisms, although clearly, infection by different pathogens has different associated costs. The effectiveness measure also did not differentiate between colonization and infection, and any unmeasured difference could account for an overestimate of our cost-effectiveness. The incremental cost-effectiveness ratio analysis is subject to variation of the underlying data. In order to account for some of the variations in costs and effectiveness data, we used one-way sensitivity and probabilistic sensitivity analyses to determine the most robust estimates possible. Finally, we did not attempt to assess how semi-annual intensive containment efforts might compare with less intensive, but continual, enhancements of infection control practices such as more frequent regular cleaning, the introduction of new cleaning technologies such as ultraviolet light or hydrogen peroxide vapor, or enhanced observation and training of staff in hand hygiene and other infection control practices. Furthermore, the 2011 MDRA outbreak response led to a significant rate reduction for the MDR organisms for six months only, and the rates increased in the ensuing six months [8]. Although further efforts are needed to understand better the effect of the model program on transmission of MDR organisms, these findings suggest that any proactive program would need to be done at least twice a year to have a sustained impact on transmission rates. This does not exempt increasing routine control measures but suggests the added need for, and potential benefits of, enhanced cleaning on a scheduled basis.
ICER = incremental cost-effectiveness ratio.
To understand better the causal relations between the interventions and reduction in the transmission rate of MDR organisms, a randomized controlled trial of different infection prevention packages should be considered to help identify the critical steps in a routinely scheduled program to reduce the rate of hospital-acquired infections proactively. A prospective randomized trial also would facilitate collection of cost data more reliably. Currently, standard accounting systems for daily operations do not easily capture the direct costs associated with infection control interventions, as these systems are in place for tracking health care expenditure more globally. Including cost data in future studies would be valuable for public policy.
Conclusion
This study evaluated the cost-effectiveness of implementing bundled interventions derived from the 2011 MDRA outbreak in the general surgery ICU to reduce transmission of MDR organisms in critically ill surgical patients. The 2011 MDRA outbreak response was estimated to cost $371,079 in 2011 dollars. If a proactive program was designed based on this outbreak response, the total cost is an estimated $68,509 per year. If this proactive program were implemented periodically, the incremental cost-effectiveness ratio would be $3,804 per averted transmission of an MDR organism. Further randomized analysis are needed to identify a more established causal relation between hand hygiene, deep cleaning, and the reduction in transmission of MDR organisms and to guide the design of a routine prevention scheme. Nonetheless, this cost-effectiveness analysis could serve as a reference for the design and implementation of a program aimed at reducing the transmission of MDR organisms in critically ill surgical patients.
Footnotes
Acknowledgments
We thank S.A., A.K., and the Partners Center for Clinical Excellence at Brigham and Women's Hospital for their support of this work. We are grateful to all of our patients for the opportunity to care for them, and to P.K. in particular, whose illness spurred us to ask these questions.
The Partners Centers of Expertise Quality and Patient Safety Program and Partners Graduate Medical Education supported the conduct of this project.
Author Disclosure Statement
No competing financial interests exist.